
BMP-2 is an effective, currently non-FDA-approved method of treating a chronic poor healing non-union fracture of the tibia.
Miss. Samantha Hill, Washington State University, Elson S. Floyd College of Medicine, Spokane, Washington, USA. E-mail: samantha.m.hill@wsu.edu
Abstract
Introduction: Bone morphogenetic protein-2 (BMP-2) is an osteoinductive growth factor approved for use in interbody spinal fusion and open tibial shaft fractures. Reports of its off-label application exist, but there is limited documentation regarding its use in closed tibial pseudoarthrosis. This case is notable as one of the first to describe the successful use of BMP-2 in a young male with osteoporosis and hypogonadism, conditions that further complicate fracture healing.
Case Report: A 32-year-old non-smoking Caucasian male sustained a Gustilo-Anderson grade 1 open fracture of the left tibia and fibula, initially treated with intramedullary nailing. The proximal interlocking screw was later removed for dynamization to promote axial loading, but radiographs demonstrated inadequate tibial healing. He subsequently underwent exchange intramedullary nailing with proximal and distal interlocking, fibular osteotomy, preparation of the tibial non-union site, and bone grafting from the fibular osteotomy. Despite these interventions, progressive radiographs continued to demonstrate inadequate healing. Workup revealed osteoporosis (lumbar T-score –2.5) and hypogonadism (testosterone 200 ng/dL). Medical optimization was initiated with testosterone supplementation and teriparatide injections. Due to persistent pseudoarthrosis, the patient ultimately underwent open preparation of the tibial non-union site with eburnation, application of recombinant BMP-2, and iliac crest autograft. Subsequent radiographs demonstrated healing of both the tibia and fibula, with mild valgus alignment that was clinically insignificant. The patient was pleased with the results and is doing better overall.
Conclusion: Eleven months after surgery, the tibia demonstrated radiographic healing with no significant complications. This case highlights the potential role of BMP-2 as an adjunctive therapy for difficult-to-heal closed tibial pseudoarthrosis, particularly in the setting of metabolic bone disease. Its successful use in this patient suggests that it may expand treatment options for refractory non-union beyond currently approved indications, contributing to broader orthopedic practice.
Keywords: Tibial pseudoarthrosis, bone morphogenetic protein-2, osteoporosis, hypogonadism, non-union fracture.
Bone morphogenetic proteins (BMPs) are growth factors in the transforming growth factor-beta superfamily that play key roles in development and bone formation. BMP-2 is the most widely studied and clinically used subtype due to its osteoinductive properties. Recombinant human BMP-2 (rhBMP-2), initially released in 2002, was originally used for cervical and lumbar fusions and progressive usage in open tibia fractures [1]. Since its approval, clinical use has expanded rapidly, with a marked increase in both on-label and off-label applications. Despite this growth, there is limited literature evaluating the use of BMP-2 for closed tibial pseudoarthrosis. Non-union of tibial fractures remains a challenging problem, with reported prevalence ranging from 4% to 8% depending on patient and injury characteristics. Risk factors include open fractures, infection, high-energy trauma, and metabolic bone disease [2]. Secondary osteoporosis in men, particularly when related to hypogonadism, is increasingly recognized as an underdiagnosed contributor to impaired bone healing. Hypogonadism is associated with reduced bone mineral density, higher rates of fragility fractures and impaired fracture repair [3]. Men with untreated hypogonadism are also at increased risk of major fractures, but only a small fraction of them are treated with testosterone or other bone-active agents [4]. Here, we present a case of a young male with osteoporosis and hypogonadism who developed tibial pseudoarthrosis that failed multiple surgical interventions and was ultimately managed successfully with open reduction and augmentation using BMP-2 and iliac crest autograft. To the best of our knowledge, this is among the first reported cases of closed tibial pseudoarthrosis in a young male with metabolic bone disease treated successfully with rhBMP-2.
A 32-year-old non-smoking Caucasian male sustained a left grade one open tibia and fibula fracture following a motor vehicle accident. This can be seen in Fig. 1. Initial management included open reduction and internal fixation with an interlocked intramedullary nail and irrigation and debridement of the open fracture. The patient had no history of diabetes, smoking, or alcohol abuse. Family history was negative for osteoporosis or metabolic bone disease. He reported decreased libido and fatigue but had not undergone prior endocrine evaluation.
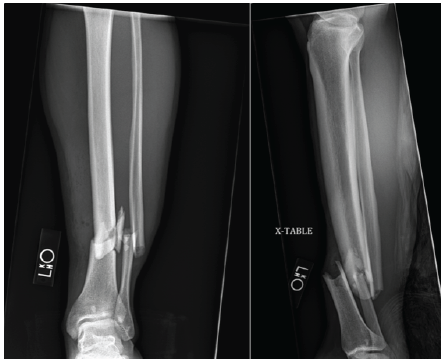
Figure 1: Radiographs of the left tibia and fibular fracture associated with a Gustilo-Anderson grade 1 open fracture with intact neurological and vascular status.

Figure 2: Radiographs identified that there was a non-union or pseudoarthrosis associated with the tibia, but there was healing associated with the fibula. The proximal interlocking screw removal is identified with the lack of a screw proximally.
At 4 months, radiographs demonstrated delayed union, as noted in Fig. 2. The proximal interlocking screws were removed to allow dynamization. Six months later, persistent non-union was present, with continued pain and difficulty bearing weight. He subsequently underwent exchange intramedullary nailing with interlocking, fibular osteotomy, local bone grafting, and debridement of the pseudoarthrosis site. Despite these procedures, serial radiographs over the following months showed no evidence of progressive healing, as seen in Fig. 3.
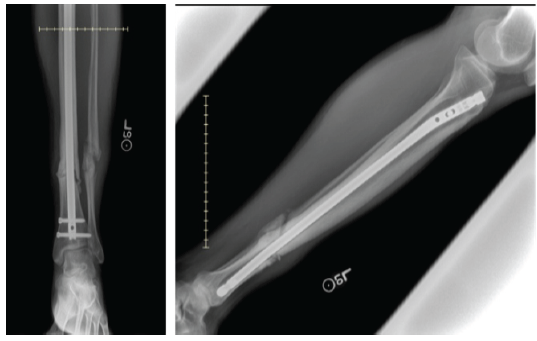
Figure 3: Radiographs prior to final surgery showing fibular pseudoarthrosis and tibial non-union despite prior interventions.
Further evaluation revealed metabolic bone disease. Dual-energy X-ray absorptiometry demonstrated osteoporosis with a lumbar spine T-score of –2.5, total hip –1.9, and femoral neck –1.5. Laboratory studies confirmed hypogonadism with low serum testosterone.
Six months after exchange nailing, the patient underwent open reduction and treatment of tibial pseudoarthrosis with augmentation of the non-union site using two pledgets of rhBMP-2 (Medtronic INFUSE™, total dose 4.2 mg) and iliac crest autograft. Intraoperatively, the pseudoarthrosis site was debrided and prepared before grafting. The intramedullary nail was retained for stability. Fig. 4 for post-operative imaging.
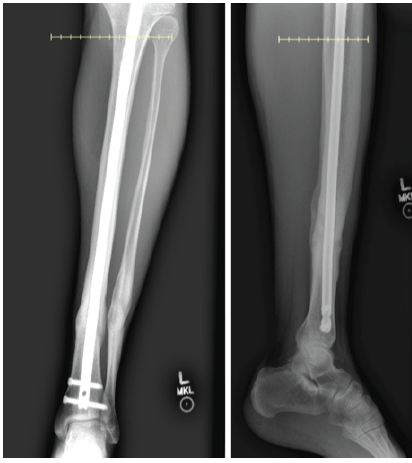
Figure 4: Radiographs demonstrate healing of the tibia and fibula after isolated tibial revision with debridement, hardware removal, bone morphogenetic protein application, and iliac crest bone grafting, without intervention at the fibular site.
At the patient’s last post-operative visit, he stated his pain as a 2/10 and occurring only occasionally. The patient reported being very satisfied with the outcome.
Successful fracture union is influenced by multiple patient and injury-related factors, including age, smoking, diabetes, obesity, high-energy trauma, open fracture, and infection [2]. Our patient, though young and otherwise healthy, had underlying hypogonadism-associated osteoporosis, a rarely described risk factor for tibial non-union. The literature suggests that osteoporosis is a risk factor for non-union, which argues that hypogonadism-associated osteoporosis is a plausible contributor to tibial non-union [5]. Non-union of tibial fractures occurs in up to 8% of cases, with higher rates in those with systemic or local risk factors [2]. One study had reported union in 25/27 of the chronic tibial non-unions that were treated with rhBMP-2 compared to 33% of union found in no-BMP control group [6]. Another similar study had found that 9 tibial non-unions that were treated with rhBMP-2 with an autograft had all united with 95.8% healed at 6 months and 100% healed at 12 months [7]. Closed tibial pseudoarthrosis is particularly challenging, as biological stimulation is often limited compared to open fractures, where soft-tissue manipulation or grafting is more feasible. Conventional options such as dynamization, exchange nailing, fibular osteotomy, and bone grafting may fail in difficult biological environments. BMP-2 provides potent osteoinductive signaling and has been shown to stimulate mesenchymal stem cell differentiation, angiogenesis, and endochondral ossification. While Food and Drug Administration (FDA) approval is limited to spinal fusion and open tibial shaft fractures, off-label applications in long bone non-unions are increasingly reported. Complications include ectopic bone formation, inflammation, wound swelling, and theoretical malignancy risk, though large trials have not consistently demonstrated significant excess risk. A review of the clinical side effects of BMP-2 found that although BMP-2 is biologically upregulated in several cancers, no evidence has been found that it increases the risk of malignant transformation and carcinogenesis [8]. In addition, there was determined to be no antibody formation or systemic illness associated with BMP-2 usage [7]. High cost remains a barrier to widespread adoption. With BMP-2 use for tibial non-union being off-label, insurance coverage is typically unavailable, leaving access dependent on institutional policy and patient resources. Conversely, its use in open tibial shaft fractures (Gustilo types I–IIIA) is FDA-approved with a labeled indication (INFUSE® Bone Graft) [9,10]. Economic models in Germany suggest that the usage of BMP-2 may actually reduce overall costs as reoperation and secondary intervention rates would be lowered [11]. For chronic non-unions, the decision is based on individual case severity, prior failures, and cost constraints. This case highlights the potential of BMP-2 in the setting of impaired bone healing compounded by metabolic bone disease. The addition of iliac crest autograft provided osteogenic and osteoconductive support, while BMP-2 supplied a powerful osteoinductive stimulus. Together, these likely created an environment conducive to union where previous surgeries had failed. The role of hypogonadism in fracture healing is increasingly recognized. Male osteoporosis accounts for nearly one-third of all fragility fractures yet remains underdiagnosed and undertreated [3]. Hypogonadism is a well-established cause of secondary osteoporosis and is associated with increased fracture risk [4]. Testosterone supplementation has been shown to improve bone mineral density and reduce fracture incidence in hypogonadal men [3]. However, little is known about how hypogonadism directly impacts fracture healing, or how biologic agents such as BMP-2 may mitigate impaired bone regeneration in this population. This case is unique in that it demonstrates successful fracture union using BMP-2 in a patient with two complicating metabolic conditions – osteoporosis and hypogonadism – that are rarely reported together in the context of pseudoarthrosis. The combined surgical and medical management highlights the importance of a multidisciplinary approach: Orthopaedic intervention with BMP-2 augmentation, and endocrine-directed management with testosterone and teriparatide.
Limitations
This is an only single case of a successful treated tibial non-union. Broader studies are required to define the efficacy, safety, and cost-effectiveness of BMP-2 in refractory tibial non-unions, particularly in patients with metabolic bone disease.
This case demonstrates that BMP-2 can promote healing of closed tibial pseudoarthrosis, even in the setting of osteoporosis and hypogonadism. Although off-label, its successful use highlights the potential role of BMP-2 as an adjunctive treatment for difficult non-unions. The case also underscores the importance of evaluating and treating underlying metabolic bone disease in young patients presenting with delayed union. Multidisciplinary care combining orthopedic, endocrine, and pharmacologic strategies may significantly improve outcomes in challenging cases. Broader investigation is needed to determine optimal patient selection and long-term results of BMP-2 in similar scenarios.
This case highlights the potential role of BMP-2 as an adjunctive treatment for refractory closed tibial pseudoarthrosis, especially in patients with underlying metabolic bone disease such as osteoporosis and hypogonadism. Early recognition and management of systemic risk factors, in collaboration with endocrine care, may improve outcomes in challenging non-union cases.
References
- 1. Valdes MA, Thakur NA, Namdari S, Ciombor DM, Palumbo M. Recombinant bone morphogenic protein-2 in orthopaedic surgery: A review. Arch Orthop Trauma Surg 2009;129:1651-7. [Google Scholar] [PubMed]
- 2. Tian R, Zheng F, Zhao W, Zhang Y, Yuan J, Zhang B, et al. Prevalence and influencing factors of nonunion in patients with tibial fracture: Systematic review and meta-analysis. J Orthop Surg Res 2020;15:377. [Google Scholar] [PubMed]
- 3. Bandeira L, Silva BC, Bilezikian JP. Male osteoporosis. Arch Endocrinol Metab 2022;66:739-47. [Google Scholar] [PubMed]
- 4. Snyder PJ, Bauer DC, Ellenberg SS, Cauley JA, Buhr KA, Bhasin S, et al. Testosterone treatment and fractures in men with hypogonadism. N Engl J Med 2024;390:203-11. [Google Scholar] [PubMed]
- 5. Zura R, Xiong Z, Einhorn T, Watson JT, Ostrum RF, Prayson MJ, et al. Epidemiology of fracture nonunion in 18 human bones. JAMA Surg 2016;151:e162775. [Google Scholar] [PubMed]
- 6. Fuchs T, Schmidmaier G, Raschke MJ. The use of bone morphogenetic protein-2 (rhBMP-2) in the treatment of non-unions: A retrospective multicentre study of 98 cases. Injury 2021;52:91-9. [Google Scholar] [PubMed]
- 7. Choi YJ, Lee JH, Kim YH, Kang YK. Bone morphogenetic protein-2 combined with autologous bone graft for treatment of long bone nonunion: A prospective study. BMC Musculoskelet Disord 2024;25:351. [Google Scholar] [PubMed]
- 8. James AW, LaChaud G, Shen J, Asatrian G, Nguyen V, Zhang X, et al. A review of the clinical side effects of bone morphogenetic protein-2. Tissue Eng Part B Rev 2016;22:284-97. [Google Scholar] [PubMed]
- 9. Rupp M, Popp D, Alt V. Prevention of infection in open fractures: Where are the pendulums now? Injury 2020;51 Suppl 2:S57-63. [Google Scholar] [PubMed]
- 10. United States Food and Drug Administration. Summary of Safety and Probable Benefit: INFUSE/MASTERGRAFT Posterolateral Revision Device (HDE H040004). Silver Spring, MD: US Department of Health and Human Services, Food and Drug Administration; 2008. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf4/h040004b.pdf [Last accessed on 2025 Sep 12]. [Google Scholar] [PubMed]
- 11. Alt V, Heissel A. Economic considerations for the use of recombinant human bone morphogenetic protein-2 in open tibial fractures in Europe: The German model. Curr Med Res Opin 2006;22 Suppl 1:S19-22. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery
July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study