
Spinal osteoid osteoma is a rare tumor that can present atypically with radiculopathy and poor NSAID response when near neural structures, with CT as the diagnostic gold standard, and although radiofrequency ablation is often effective, management should be tailored to lesion location when proximity to neural elements.
Dr. Mehmet Erkilinc, Department of Orthopedic Surgery, St. Louis University, Saint Louis University School of Medicine, SSM Health Cardinal Glennon Children’s Hospital, 1465 South Grand Blvd, Saint Louis - 63104, Missouri, United States. E-mail: mehmet.erkilinc@ssmhealth.com
Abstract
Introduction: Osteoid osteoma (OO) is a benign osteogenic tumor that most commonly affects long bones, accounting for 2–3% of primary bone tumors. Spinal involvement is relatively rare, representing 6–20% of cases, with the lumbar spine being the most frequently affected region. Typical spinal OO presents with painful scoliosis and nocturnal pain relieved by non-steroidal anti-inflammatory drugs (NSAIDs). However, atypical presentations may occur when lesions are located adjacent to neural structures, leading to radicular symptoms and poor NSAID response. This case report describes an unusual presentation of OO in the L4 superior articular process, manifesting with back and leg pain, minimal NSAID responsiveness, and nerve root irritation.
Case Report: A 17-year-old male presented with a 6-month history of back and leg pain, fluctuating between 3/10 and 7/10 in severity, with associated numbness in the L3 dermatome. Examination revealed painful paraspinal palpation and a positive straight leg raise on the right side, without motor weakness or reflex abnormalities. Magnetic resonance imaging demonstrated non-specific inflammatory changes, whereas computed tomography (CT) confirmed a 9 × 9 mm nidus in the right superior articular process of L4. Given the lesion’s proximity to neural structures, radiofrequency ablation was deemed unsafe, and surgical excision was performed. The patient underwent open resection of the nidus with preservation of the inferior facet joint. Immediate post-operative resolution of leg pain was noted, and at 3-month follow-up, the patient reported complete resolution of both back and leg pain, with no recurrence of symptoms.
Conclusion: This case highlights an atypical presentation of spinal OO, characterized by radicular symptoms and poor NSAID response due to nerve root inflammation. It underscores the importance of considering OO in the differential diagnosis of adolescent back and leg pain, even in the absence of classic features. CT imaging remains essential for definitive diagnosis, and surgical excision provides safe and effective treatment when minimally invasive options are contraindicated by lesion proximity to neural structures.
Keywords: Osteoid osteoma, spine, radiculopathy, surgical excision, lumbar facet joint.
Osteoid osteoma (OO) is a benign osteogenic tumor that typically affects long bones and accounts for approximately 2–3% of all primary bone tumors [1,2]. Although most cases occur in the appendicular skeleton, spinal involvement has been reported in 6–20% of patients, with the lumbar spine being the most frequently affected region [1,2,3]. Within the spine, OOs most often arise in the posterior elements, and their proximity to neural structures can lead to distinctive clinical challenges. The classic presentation of spinal OO includes painful scoliosis, nocturnal pain, and marked relief with non-steroidal anti-inflammatory drugs (NSAIDs) [3,4,5]. This characteristic response to NSAIDs is considered a hallmark of the disease and often guides clinical suspicion. However, atypical presentations may occur, particularly when the lesion induces inflammatory changes in adjacent neural structures, resulting in radicular symptoms rather than isolated mechanical pain. Management strategies for spinal OO vary depending on lesion location, accessibility, and symptom severity. Observation and NSAID therapy may suffice in typical cases, whereas minimally invasive techniques such as percutaneous radiofrequency ablation (RFA) have emerged as safe and effective options when medical management fails [6,7]. RFA, however, requires careful consideration when lesions are located within 1 cm of neural elements, as thermal injury risk necessitates protective measures [6,8]. In such scenarios, open surgical resection remains the preferred approach, particularly when the tumor is inaccessible to percutaneous methods or situated in close proximity to critical neurovascular structures [6]. Here, we present the case of a 17-year-old male with an OO of the L4 superior articular process. Unlike the typical presentation of painful scoliosis with NSAID responsiveness, this patient developed back and leg pain with minimal relief from NSAID therapy. The unusual clinical course was attributed to tumor-induced nerve root inflammation, resulting in radicular symptoms. Given the lesion’s proximity to neural structures and poor response to conservative measures, surgical resection was performed. This case highlights a rare and atypical presentation of spinal OO and underscores the importance of individualized management in complex spinal lesions.
A 17-year-old male presented with a 6-month history of persistent back and leg pain. The pain was predominantly localized to the lumbar region but occasionally radiated to the right leg, with reported numbness in the L3 dermatomal distribution. Pain intensity fluctuated between 3/10 and 7/10, with back pain being most prominent. Analgesic response was minimal with NSAIDs, though partial relief was noted with Flexeril and a Medrol dose pack. On physical examination, the lumbar spine was mildly flexible, and palpation of paraspinal muscles elicited pain. The straight leg raise was negative on the left but positive on the right. Neurological examination revealed no motor weakness and normal reflexes. The patient presented to us with a previous X-ray and magnetic resonance imaging (MRI) of the lumbar spine. Plain radiographs of the lumbar spine performed before presentation did not reveal significant pathology. MRI demonstrated:
- Minimal soft-tissue enhancement in the right paraspinal region at the L3 vertebral body level, extending into the right L3–L4 neural foramina with enhancement of the right L3 nerve root. These findings were suggestive of infectious or inflammatory changes, though post-traumatic changes could not be excluded
- Enhancement of the right L3 and L4 transverse processes and pedicles, consistent with marrow edema.
Given the non-specific MRI findings, a computed tomography (CT) scan was obtained. CT revealed a rounded lesion in the right superior articular process of L4, measuring 9 × 9 mm, with surrounding sclerosis and a central lucent nidus. The lesion was located at the level of the facet joint, consistent with OO (Fig. 1).

Figure 1: Computerized tomography scan of the L4 superior articular process osteoid osteoma.
Treatment options were discussed with the patient and family. Interventional radiology deemed RFA unsafe due to the lesion’s proximity to neural structures and pre-existing nerve root inflammation. The patient and family elected to proceed with surgical excision.
A posterior approach was performed. Following fluoroscopic confirmation of the level, sharp dissection exposed the facet joint elements. The most proximal 1 cm of the superior articular process was excised with an osteotome. The nidus was completely removed with a 1–2 mm macroscopic margin (Fig. 2). Bone wax was applied to the exposed bone surface, and the inferior part of the facet joint capsule was preserved. The wound was irrigated, and hemostasis was achieved without complication.
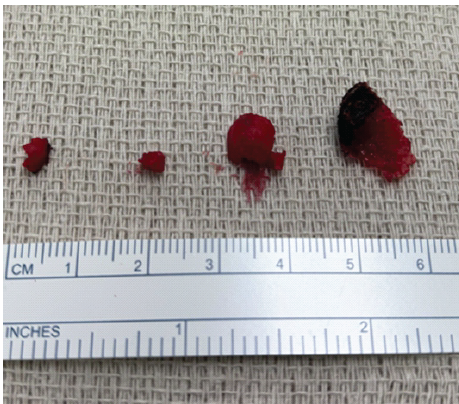
Figure 2: Macroscopic image of osteoid osteoma and nidus formation after surgical excision.
Postoperatively, the patient experienced immediate resolution of leg pain. At follow-up visits, he reported complete resolution of back pain. At 3 months, the patient remained asymptomatic, with no recurrence of back or leg pain.
OO is a benign osteogenic tumor most commonly affecting long bones, particularly the femur and tibia, and accounts for approximately 2–3% of all primary bone tumors [1]. Spinal involvement is relatively uncommon, representing about 10% of cases, with a predilection for the posterior elements of the lumbar spine. The classic clinical presentation includes nocturnal pain and painful scoliosis, with symptoms typically relieved by NSAIDs [3,9]. In contrast, our patient presented with back and leg pain, numbness in the L3 dermatome, and minimal response to NSAIDs. This atypical presentation can be explained by tumor-induced inflammation of the adjacent nerve root, resulting in radicular symptoms rather than isolated mechanical pain. Such radiculopathy has been described in rare cases of spinal OO, where proximity to neural structures alters the clinical picture. In one case, the patient presented with lower extremity contracture due to nerve root inflammation [10]. Imaging plays a critical role in diagnosis. While MRI is sensitive to marrow and soft-tissue changes, it is often non-specific and may mimic infection or trauma. CT remains the gold standard for identifying the nidus, typically a small lucent lesion with surrounding sclerosis. In our case, MRI suggested inflammatory changes but failed to clearly identify the nidus, whereas CT confirmed the diagnosis [3,11]. Treatment options for spinal OO include conservative management with NSAIDs, percutaneous RFA, and surgical excision. RFA is considered safe and effective in most cases, but its use is limited when lesions are located within 1 cm of neural structures due to the risk of thermal injury [6,12]. Thermal protection techniques during RFA are defined and can be used to mitigate the risks [13,14]. Our patient underwent surgical excision with complete nidus removal, resulting in immediate and sustained symptom resolution.
Spinal OO is an uncommon entity that typically presents with painful scoliosis and nocturnal pain relieved by NSAIDs. However, atypical presentations may occur when lesions are located adjacent to neural structures, resulting in radicular symptoms and poor response to conservative therapy. In this case, a 17-year-old male presented with back and leg pain, minimal NSAID responsiveness, and nerve root irritation due to an OO of the L4 superior articular process. Definitive diagnosis was achieved with CT imaging, and surgical excision was performed due to the lesion’s proximity to neural elements, precluding safe RFA. The patient experienced immediate and sustained resolution of symptoms following surgery. This case highlights the importance of considering OO in the differential diagnosis of atypical lumbar pain in adolescents, recognizing its variable clinical presentations, and tailoring management strategies to lesion location and patient-specific factors.
With spinal OO accounting for a minority of cases and typically presenting with painful scoliosis responsive to NSAIDs, our report highlights an unusual scenario of radicular symptoms and poor NSAID response due to nerve root inflammation. This case emphasizes the importance of considering OO in the differential diagnosis of adolescent back and leg pain, even when classic features are absent. It also reinforces that surgical excision remains a safe and effective option when RFA is contraindicated by proximity to neural structures.
References
- 1. Tepelenis K, Skandalakis GP, Papathanakos G, Kefala MA, Kitsouli A, Barbouti A, et al. Osteoid osteoma: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features, and treatment option. In Vivo 2021;35:1929-38. [Google Scholar] [PubMed]
- 2. Hakim DN, Pelly T, Kulendran M, Caris JA. Benign tumours of the bone: A review. J Bone Oncol 2015;4:37-41. [Google Scholar] [PubMed]
- 3. Farid AR, Liu DS, Morcos MM, Hogue GD. Spinal osteoid osteoma in the pediatric population: A management algorithm and systematic review. J Child Orthop 2023;17:428-41. [Google Scholar] [PubMed]
- 4. Aydinli U, Ozturk C, Ersozlu S, Filiz G. Results of surgical treatment of osteoid osteoma of the spine. Acta Orthop Belg 2003;69:350-4. [Google Scholar] [PubMed]
- 5. Burn SC, Ansorge O, Zeller R, Drake JM. Management of osteoblastoma and osteoid osteoma of the spine in childhood. J Neurosurg Pediatr 2009;4:434-8. [Google Scholar] [PubMed]
- 6. Sangiorgio A, Oldrini LM, Candrian C, Errani C, Filardo G. Radiofrequency ablation is as safe and effective as surgical excision for spinal osteoid osteoma: A systematic review and meta-analysis. Eur Spine J 2023;32:210-20. [Google Scholar] [PubMed]
- 7. Faddoul J, Faddoul Y, Kobaiter-Maarrawi S, Moussa R, Rizk T, Nohra G, et al. Radiofrequency ablation of spinal osteoid osteoma: A prospective study. J Neurosurg Spine 2017;26:313-8. [Google Scholar] [PubMed]
- 8. Yu X, Wang B, Yang S, Han S, Jiang L, Liu X, et al. Percutaneous radiofrequency ablation versus open surgical resection for spinal osteoid osteoma. Spine J 2019;19:509-15. [Google Scholar] [PubMed]
- 9. Tekaya AB, Moalla M, Salah MB, Saidane O, Tekaya R, Hadhri K, et al. Spinal osteoid osteoma revealed by radiculopathy: Case report and literature review. Int J Spine Surg 2021;14 Suppl 4:S26-32. [Google Scholar] [PubMed]
- 10. Clohisy JC, Rubio DR, Gupta MC. Severe contracture in the lower extremity resulting from an osteoid osteoma of the lumbar spine in close proximity to neural elements in an adolescent: A case report. Spine Deform 2022;10:727-31. [Google Scholar] [PubMed]
- 11. Kirwan EO, Hutton PA, Pozo JL, Ransford AO. Osteoid osteoma and benign osteoblastoma of the spine. Clinical presentation and treatment. J Bone Joint Surg Br 1984;66:21-6. [Google Scholar] [PubMed]
- 12. Albisinni U, Facchini G, Spinnato P, Gasbarrini A, Bazzocchi A. Spinal osteoid osteoma: Efficacy and safety of radiofrequency ablation. Skeletal Radiol 2017;46:1087-94. [Google Scholar] [PubMed]
- 13. Klass D, Marshall T, Toms A. CT-guided radiofrequency ablation of spinal osteoid osteomas with concomitant perineural and epidural irrigation for neuroprotection. Eur Radiol 2009;19:2238-43. [Google Scholar] [PubMed]
- 14. Rybak LD, Gangi A, Buy X, La Rocca Vieira R, Wittig J. Thermal ablation of spinal osteoid osteomas close to neural elements: Technical considerations. AJR Am J Roentgenol 2010;195:W293-8. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report
May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report
August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report September 10, 2022 Osteoid Osteoma of the Distal Phalanx of Little Finger
September 10, 2022 Osteoid Osteoma of the Distal Phalanx of Little Finger June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center
June 1, 2026 Survivorship and Functional Outcomes after Surgery for Metastatic Spinal Disease Including Cord Compression: Single-Surgeon Cohort Series from UK Tertiary Center