
Rare presentation of tumor with unusual symptoms and to avoid possible misdirection and misdiagnosis leading to inappropriate treatment.
Dr. Ninad Kishor Honwadkar, Department of Orthopaedics, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospital, Pune, Maharashtra, India. E-mail: drninadhonwadkar@gmail.com
Abstract
Introduction: Osteochondromas (OCs) are benign hamartomatous lesions composed of cartilage and bone, arising from aberrant growth-plate cartilage. They characteristically project from the bone surface through the cortex and grow by endochondral ossification beneath the periosteum. Lesion growth usually parallels skeletal growth and typically ceases after physeal closure, although minimal growth of the cartilage cap may persist and generally stops by the third decade of life. This developmental mechanism explains the predilection for involvement of the distal femur, proximal tibia, and proximal humerus. Most OCs are asymptomatic and do not require surgical intervention. However, intra-articular or atypically located lesions may produce pain, restricted joint movement, or compression of adjacent neurovascular structures, necessitating operative management.
Case Report: A 39-year-old male presented to the outpatient department with complaints of left-sided hip pain associated with restricted range of motion and radiating pain along the posterior aspect of the left thigh, accompanied by buttock pain for 6 months. The symptoms had gradually progressed and were aggravated by activity. The patient also reported mild paresthesia over the anteromedial aspect of the left knee and the dorsum of the left foot. He noticed a gradually enlarging, ill-defined mass in the left gluteal region during the same period. On clinical examination, a firm, immobile mass measuring approximately 10 × 6 cm was palpated in the left buttock. Left hip flexion was limited to 60° due to pain. Neurological examination revealed weakness of both plantar flexion and dorsiflexion of the left ankle. The patient had previously received conservative treatment, including rest, non-steroidal anti-inflammatory drugs, and physiotherapy at another institution, with no improvement in symptoms.
Results: The lesion was excised through a posterior approach with the patient positioned in the right lateral decubitus position, as described by Yu et al. The sciatic nerve was identified, carefully dissected, and protected throughout the procedure. The OCs were excised using an osteotome. Intraoperative assessment of the femoral neck revealed no cortical defects or fractures, and no fixation was required. Histopathological examination confirmed the diagnosis of OCs with a cartilaginous cap measuring <1 cm.
Conclusion: Sciatic nerve compression symptoms in non-traumatic cases in young adults may result due to intra or extraspinal causes, depending on the anatomical site of involvement. Lumbar intervertebral disc prolapse and spinal canal stenosis constitute the most frequent intraspinal causes. Extraspinal etiologies are comparatively rare and include conditions such as piriformis syndrome and pelvic bone lesions. Benign bone tumors, particularly OCs, though uncommon, should be considered as a potential source of sciatic nerve compression. OCs arising from the femoral neck with intra-articular or posterior extension are rare, particularly in adults, and may present with pain, mechanical restriction of movement, and neurological symptoms due to mass effect. Awareness of such atypical presentations is essential to avoid misdiagnosis and delays in appropriate management.
Keywords: Osteochondroma, proximal femur, sciatic nerve, neurological.
Osteochondromas (OCs) are benign hamartomatous lesions composed of cartilage and bone, arising from aberrant growth-plate cartilage. They characteristically project from the bone surface through the cortex and grow by endochondral ossification beneath the periosteum. The lesion growth usually parallels skeletal growth and typically ceases after physeal closure. However, minimal growth of the cartilage cap may persist and generally stops by the third decade of life. Nearly 90% of OCs present as solitary lesions, while multiple lesions are associated with hereditary multiple exostosis (HME) [1]. Solitary lesions most commonly present during the second and third decades, whereas HME-related lesions usually manifest in childhood [2]. OCs are typically extra-articular and arise from the metaphyseal region of long bones. This developmental mechanism explains the predilection for involvement of the distal femur, proximal tibia, and proximal humerus [3]. Most OCs are asymptomatic and do not require surgical intervention. However, intra-articular or atypically located lesions may produce pain, restricted joint movement, or compression of adjacent neurovascular structures, necessitating operative management [4,5]. This report describes a rare and atypical presentation of OCs involving the femoral neck in an adult patient, highlighting the potential for diagnostic confusion.
A 39-year-old male presented to the outpatient department with complaints of left-sided hip pain associated with restricted range of motion and radiating pain along the posterior aspect of the left thigh, accompanied by buttock pain aggravated for 6 months with complaints persisting since 1 year. The symptoms had gradually progressed and were aggravated by activity. The patient also reported mild paresthesia over the anteromedial aspect of the left knee and the dorsum of the left foot. He noticed a gradually enlarging, ill-defined mass in the left gluteal region during the same period. On clinical examination, a firm, immobile mass measuring approximately 10 × 6 cm was palpated in the left buttock. Left hip flexion was limited to 60° due to pain. Neurological examination revealed weakness of both plantar flexion and dorsiflexion of the left ankle. The patient had previously received conservative treatment, including rest, non-steroidal anti-inflammatory drugs, and physiotherapy at another institution, with no improvement in symptoms.
Assessment
Plain radiographs of the pelvis and left hip demonstrated a bony protuberance arising from the posteroinferior aspect of the left femoral neck (Fig. 1 and 2). There was no radiological evidence of fracture or underlying joint pathology such as osteoarthritis or osteonecrosis.

Figure 1 & 2: Routine X-rays.
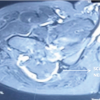
Axial T1-weighted magnetic resonance images revealed a bony outgrowth arising from the posteroinferior region of the femoral neck, extending toward the lesser trochanter (Fig. 3).
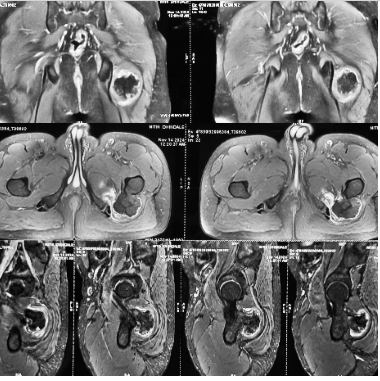
Figure 3: Magnetic resonance imaging scans indicate a hypointense lesion in the proximal femur.
The lesion showed continuity with the metaphyseal marrow cavity, and a thin peripheral high-signal rim was noted on fat-suppressed T2-weighted sequences, consistent with a cartilage cap. Based on magnetic resonance imaging, a needle biopsy was done which was suggestive of OCs (Fig. 4) following which the patient was taken up for operative intervention.
Figure 4: Needle biopsy report.
Management
The lesion was excised through a posterior approach with the patient positioned in the right lateral decubitus position, as described by Yu et al. [5]. The sciatic nerve was identified, carefully dissected, and protected throughout the procedure (Fig. 5). The OCs were excised using an osteotome. Intraoperative assessment of the femoral neck revealed no cortical defects or fractures, and no fixation was required. A 6 × 4 cm mass was excised as shown (Fig 5).
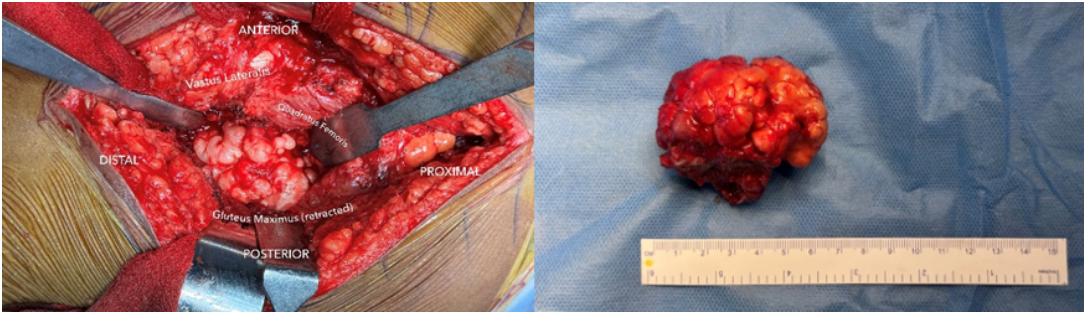
Figure 5: Intraoperative images.
Histopathological examination confirmed the diagnosis of OCs with a cartilaginous cap measuring <1 cm (Fig. 6 and 7). Post-operative radiographs show no residual lesion present (Fig. 8 and 9).
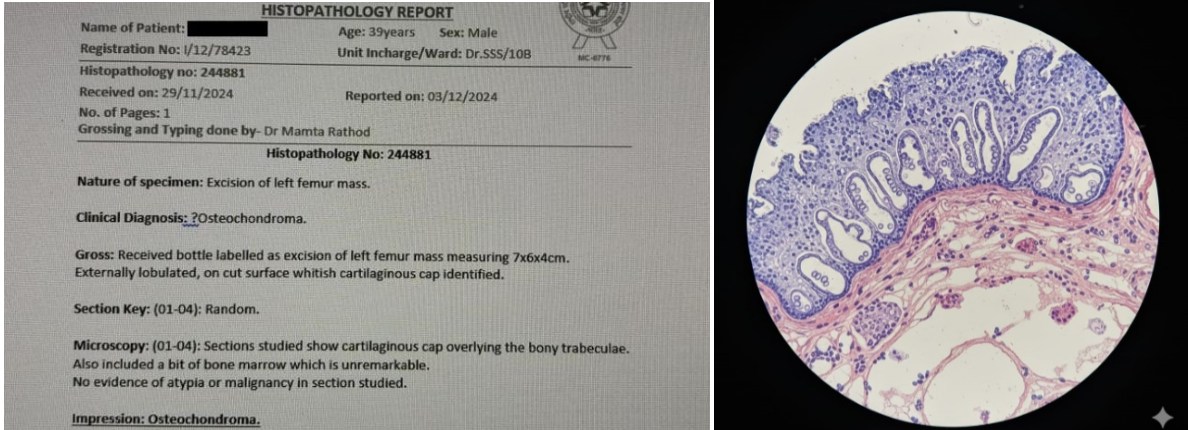
Figure 6 & 7: Histopathological evidence.
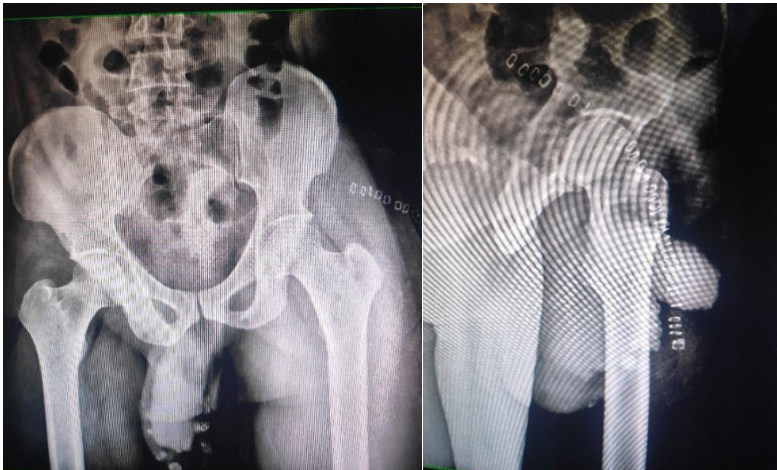
Figure 8 & 9: Post-operative X-rays.
Sciatic nerve compression in non-traumatic young adults may arise from either intraspinal or extraspinal pathology, depending on the anatomical site of involvement. Lumbar intervertebral disc prolapse and spinal canal stenosis constitute the most frequent intraspinal causes. Extraspinal etiologies are comparatively rare and include conditions such as piriformis syndrome and pelvic bone lesions. Benign bone tumors, particularly OCs, though uncommon, should be considered as a potential source of sciatic nerve compression. Other less frequently reported causes include vascular anomalies, infective processes, hereditary multiple exostoses, and neoplasms of bone or soft tissue origin [6,7,8,9,10,11,12,13,14]. Intraspinal causes typically present with associated low back pain, often precipitated by physical exertion or heavy lifting, and symptoms are usually aggravated by forward bending, axial loading, or prolonged sitting. In contrast, piriformis syndrome results from compression of the sciatic nerve due to muscle hypertrophy or spasm and is characterized by sciatica that worsens with activity, walking, or sustained sitting. The diagnosis of piriformis syndrome remains clinical and is established only after exclusion of spinal pathology [15]. Myositis ossificans, most commonly developing following trauma or neurological insult, may mimic bony lesions, causing sciatic nerve compression. However, it can be distinguished on imaging by the presence of well-defined peripheral ossification, a relatively radiolucent central zone, and cleavage planes separating the heterotopic bone from the adjacent cortex, aiding in accurate differentiation [16,17,18,19]. OCs arising from the femoral neck with intra-articular or posterior extension are rare, particularly in adults, and may present with pain, mechanical restriction of movement, and neurological symptoms due to mass effect. Awareness of such atypical presentations is essential to avoid misdiagnosis and delays in appropriate management [20]. (Fig. 10).
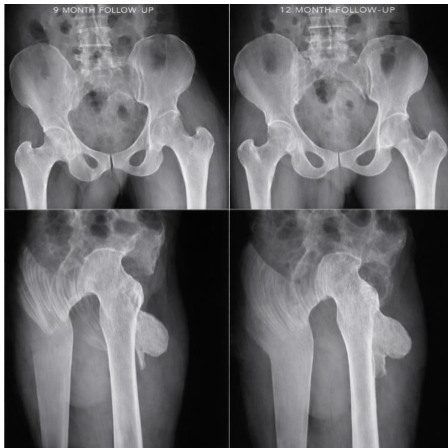
Figure 10: 9 and 12-month follow-up X-rays.
With proper written informed consent, postoperatively, the patient experienced improvement in paresthesia and numbness of the left foot, although mild buttock pain persisted initially. At 10-month follow-up, complete resolution of both sensory and motor deficits of the sciatic nerve was observed. Follow-up radiographs demonstrated no evidence of heterotopic ossification or avascular necrosis of the hip.
Although OCs are commonly asymptomatic and extra-articular, atypical intra-articular or femoral neck lesions can present in adulthood with neurovascular symptoms. A high level of clinical awareness, along with careful and comprehensive imaging evaluation, is a key to arriving at the correct diagnosis and initiating timely treatment.
References
- 1. Rains HA, Mann CV. Tumours of bones and joints. In: Bailey H, Rains AJ, Mann CV, Love RJ, editors. Bailey and Love’s Short Practice of Surgery. 20th ed. London: HK Lewis; 1988. p. 372-9. [Google Scholar] [PubMed]
- 2. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar] [PubMed]
- 3. Giudici MA, Moser RP Jr., Kransdorf MJ. Cartilaginous bone tumors. Radiol Clin North Am 1993;31:237-59. [Google Scholar] [PubMed]
- 4. Scarborough MT, Moreau G. Benign cartilage tumors. Orthop Clin North Am 1996;27:583-9. [Google Scholar] [PubMed]
- 5. Yu K, Meehan JP, Fritz A, Jamali AA. Osteochondroma of the femoral neck: A rare cause of sciatic nerve compression. Orthopedics 2010;33:574. [Google Scholar] [PubMed]
- 6. Kulcu DG, Naderi S. Differential diagnosis of intraspinal and extraspinal non-discogenic sciatica. J Clin Neurosci 2008;15:1246-52. [Google Scholar] [PubMed]
- 7. Kirschner JS, Foye PM, Cole JL. Piriformis syndrome, diagnosis and treatment. Muscle Nerve 2009;40:10-8. [Google Scholar] [PubMed]
- 8. Paik NJ, Han TR, Lim SJ. Multiple peripheral nerve compressions related to malignantly transformed hereditary multiple exostoses. Muscle Nerve 2000;23:1290-4. [Google Scholar] [PubMed]
- 9. Bickels J, Kahanovitz N, Rubert CK, Henshaw RM, Moss DP, Meller I, et al. Extraspinal bone and soft-tissue tumors as a cause of sciatica. Clinical diagnosis and recommendations: Analysis of 32 cases. Spine (Phila Pa 1976) 1999;24:1611-6. [Google Scholar] [PubMed]
- 10. Lin PP, Moussallem CD, Deavers MT. Secondary chondrosarcoma. J Am Acad Orthop Surg 2010;18:608-15. [Google Scholar] [PubMed]
- 11. Kransdorf MJ, Meis JM. From the archives of the AFIP. Extraskeletal osseous and cartilaginous tumors of the extremities. Radiographics 1993;13:853-84. [Google Scholar] [PubMed]
- 12. Siebenrock KA, Ganz R. Osteochondroma of the femoral neck. Clin Orthop Relat Res 2002;394:211-8. [Google Scholar] [PubMed]
- 13. Turan Ilica A, Yasar E, Sanal HT, Duran C, Guvenc I. Sciatic nerve compression due to femoral neck osteochondroma: MDCT and MR findings. Clin Rheumatol 2008;27:403-4. [Google Scholar] [PubMed]
- 14. Peterson HA. Multiple hereditary osteochondromata. Clin Orthop Relat Res 1989;239:222-30. [Google Scholar] [PubMed]
- 15. Bottner F, Rodl R, Kordish I, Winkelmann W, Gosheger G, Lindner N. Surgical treatment of symptomatic osteochondroma. A three- to eight-year follow-up study. J Bone Joint Surg Br 2003;85:1161-5. [Google Scholar] [PubMed]
- 16. Makhdom AM, Jiang F, Hamdy RC, Benaroch TE, Lavigne M, Saran N. Hip joint osteochondroma: Systematic review of the literature and report of three further cases. Adv Orthop 2014;2014:180254. [Google Scholar] [PubMed]
- 17. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar] [PubMed]
- 18. Wang SI, Park EH, Yoon SJ, Kim JR. Intra-articular osteochondroma of the posteroinferior femoral neck associated with hip joint osteochondromatosis: A case report. Mol Clin Oncol 2017;7:915-8. [Google Scholar] [PubMed]
- 19. Saglik A, Altay M, Unal VS, Basarir K, Yildiz Y. Manifestations and management of osteochondromas: A retrospective analysis of 382 patients. Acta Orthop Belg 2006;72:748-55. [Google Scholar] [PubMed]
- 20. De Souza AM, Júnior RZ. Osteochondroma: Ignore or investigate? Rev Bras Ortop 2014;49:555-64. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor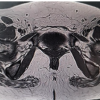 July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report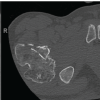 July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review