
Perthes’ disease, infective arthritis, and developmental dysplasia of the hip are the most prevalent pediatric hip pathologies in Eastern India, with alarmingly high rates of late clinical presentation that necessitate urgent improvements in early screening and referral system
Dr. Abhishek Kumar, Department of Orthopaedics, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India. E-mail: abhishek.kumarjjv123@gmail.com
Abstract
Introduction: Hip disorders in children are a diverse group of conditions that may arise due to traumatic, developmental, infectious, neoplastic, metabolic, and miscellaneous causes. These pathologies can lead to significant morbidity if undiagnosed and not treated promptly, resulting in permanent deformities, gait abnormalities, chronic pain, and compromised quality of life.
Objectives: The objective of the study was to determine the relative incidence and spectrum of various hip pathologies in pediatric patients (aged <16 years) presenting to a major tertiary care Center in Eastern India and to analyze the demographic and clinical presentation patterns.
Materials and Methods: This study was approved by the Ethics Committee of Indira Gandhi Institute of Medical Sciences (IGIMS) PATNA (Ethics Code: 989/IEC/IGIMS/2023) on April 10, 2023. All participants provided written informed consent before enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. This was a prospective, observational, and non-randomized study conducted over 18 months at the Department of Orthopedics, IGIMS, Patna. A total of 120 patients with exclusive hip pathology were included after screening 5,830 pediatric patients. Data collected included demographics, clinical presentation (pain, limp, fever, etc.), and final diagnosis based on clinical, radiological, and biochemical assessments.
Results: The overall incidence of hip pathology among children reporting to the Orthopedics department was 2.05% (120 out of 5830). Non-traumatic conditions (87%) significantly outnumbered traumatic conditions (13.34%). The most common diagnoses were: Perthes’ disease (31.93%), followed by Infective Arthritis (24.16%) and developmental dysplasia of the hip (DDH) (15.9%). The highest frequency of cases was observed in the 5–11 years age group (44.53%) and in males (63%). Perthes’ disease showed a strong male preponderance (84% males), while DDH was predominant in females (73.68%). Limp (70.83%) and pain (57.5%) were the most common presenting symptoms. A significant proportion of patients with DDH (68.4%) and Septic Arthritis (86.97%) presented late.
Conclusion: Perthes’ disease, infective arthritis, and DDH are the most prevalent hip pathologies in this region of Eastern India. The high rates of infective conditions and late presentations for both DDH and septic arthritis highlight critical gaps in early diagnosis, screening, and referral systems in the primary healthcare infrastructure. Region-specific management protocols and increased public health awareness are urgently needed.
Keywords: Slipped capital femoral epiphysis, developmental dysplasia of hip, limb length discrepancy, Legg-calve-Perthes disease.
Hip disorders in the paediatric population (patients <16 years) represent a varied collection of conditions ranging from traumatic, developmental, infectious, neoplastic, and metabolic causes [1]. These pathologies, if not promptly diagnosed and treated, frequently result in long-term morbidity, including permanent deformities, chronic pain, gait abnormalities, and compromised quality of life in adulthood [1,2]. The unique developmental anatomy of the pediatric hip, characterized by the presence of a vulnerable physeal plate and changing vascular patterns, contributes to its susceptibility to specific age-related diseases [3]. Common non-traumatic paediatric hip disorders include developmental dysplasia of the hip (DDH) (Fig. 1), Legg-Calvé-Perthes disease (Perthes’) (Fig. 2 and 3), slipped capital femoral epiphysis (SCFE) (Fig. 4), and infective conditions such as septic arthritis (Fig. 5) and tubercular arthritis [3].
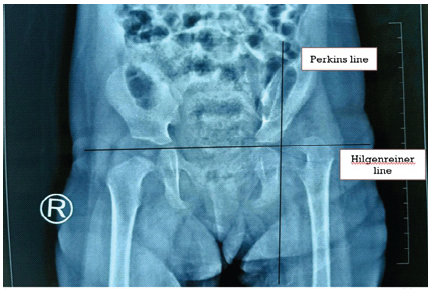
Figure 1: Image showing the small dysplastic femur head outside the shallow acetabulum cavity in upper outer quadrant.
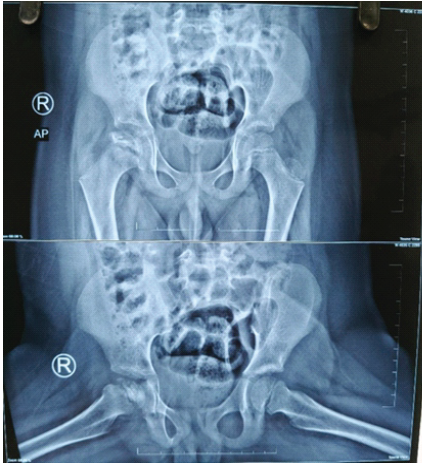
Figure 2: Radiographic image of Perthes disease showing loss of sphericity of the femoral head with cystic changes.
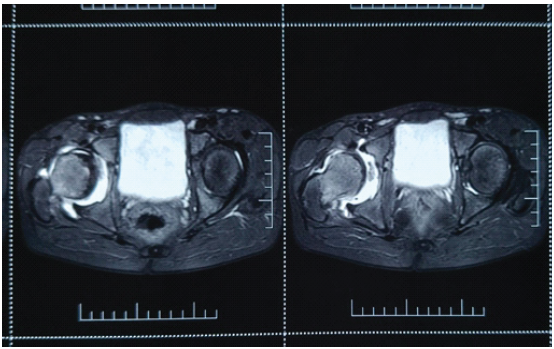
Figure 3: Magnetic resonance imaging image of Perthes disease right hip showing femoral head irregularities, cystic changes, hyperintense lesion in femoral head.

Figure 4: Left slipped capital femoral epiphysis.

Figure 5: Septic arthritis of hip right side with reduced hip joint space and osteopenic femoral neck.
The prevalence and incidence of these conditions are known to vary significantly across different geographical, ethnic, and socioeconomic populations [4]. Common traumatic conditions include neck of femur fracture, hip dislocation.
In the Indian context, available epidemiological data are often limited, stemming primarily from isolated studies in South and West India [4]. Specifically, there is scarcity of region-specific data concerning the spectrum of pediatric hip pathology in Eastern India, including the state of Bihar. Due to distinct socioeconomic, nutritional, and healthcare access variables in our region, identifying local disease patterns is crucial for developing effective intervention strategies.
Study design and setting
This was a prospective, observational, and non-randomized study conducted over an 18-month period (April 2023–October 2024) in the Department of Orthopedics at the Indira Gandhi Institute of Medical Sciences (IGIMS), Patna. Ethical clearance was obtained from the Institutional Ethics Committee of IGIMS, Patna (989/IEC/IGIMS/2023).
Participants and sample size
A total of 135 pediatric patients presenting with hip problems were screened. 15 Patients were excluded for incomplete workup, multiple diagnoses, or denial of consent. Based on a sample size calculation derived from a prior study on transient synovitis (Krul et al., [5]), a minimum number of 120 patients were required. Finally, 120 patients were included in the study.
Data collection
Patients were consecutively recruited from outpatient, inpatient, and referral departments. Data collection followed a standardized pro forma and included:
- Demographics: Age, gender, and district of residence.
- Clinical assessment: Detailed history (pain, limp, fever, trauma, etc.), comprehensive physical examination (gait, range of motion, special tests like Ortolani/Barlow, telescopy), and prior treatment history.
- Imaging: First-line imaging (X-rays, ultrasound [USG]) was performed, with advanced imaging (magnetic resonance imaging [MRI], computed tomography) indicated for inconclusive cases, early avascular necrosis, or preoperative planning.
- Biochemical/hematological assessment: Included markers like complete blood count, erythrocyte sedimentation rate, C-reactive protein, along with specific tests for infective conditions (Pus Culture and sensitivity, GeneXpert, AFB staining) or metabolic (PTH, Vit D3) conditions.
Statistical analysis
Data were compiled and analyzed using MS EXCEL and the Statistical Package for the Social Sciences Software. Descriptive statistics were used to determine frequencies, percentages, and 95% confidence intervals (CI).
Total patients included in our study were 120. Minimum age group included neonate and maximum age 16 years. Maximum patients were in the age group 5–11 years (54), and minimum no. of patients were in the age group 0–2 years (7) (Table 1).
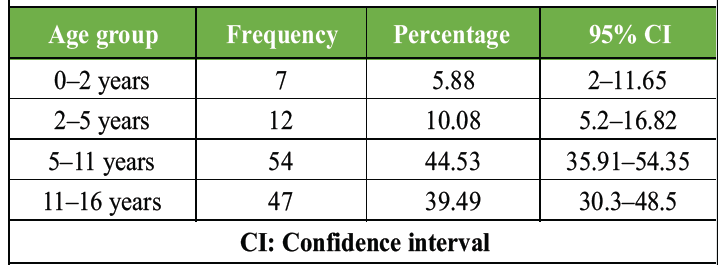
Table 1: Frequency distribution of patients according to age group.
Out of the total participants, 75 were male (62.5%) (95% CI: 53.6–71.6%), while females comprised 45 patients (37.5%) (95% CI: 28.4–46.4%) (Table 2). %), Perthes disease was the most frequent condition (38 cases, 31.66%), peaking in 5–11-year-olds (26 cases, 68.42%), while coxa vara was the rarest (just 1 case, 0.9%).
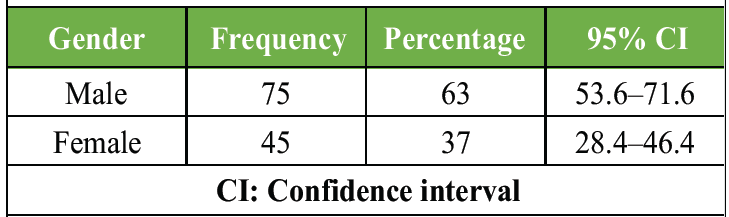
Table 2: The gender distribution of disease
Infective arthritis was highest in 11–16-year (16 cases, 55.17%), whereas DDH was most common in 2–5-year (9 cases, 47.36%), while 0–2 years had the fewest (7 cases, 6.7%). Maximum trauma cases were in 11–16-year age group (9, 56.25%). Male preponderance was seen in traumatic hip conditions (13 out of 16) and Perthes disease (32 out of 38). Female preponderance was seen in DDH (14 out of 19). Septic arthritis was nearly equal (14 males and 15 females) (Fig. 6). Out of 120 patients, traumatic cases were 16 and non-traumatic cases were 104 (Table 3).
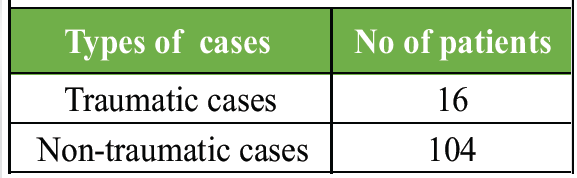
Table 3: Distribution of traumatic and non-traumatic cases
The left side was involved predominantly in DDH (14), trauma (11), and septic arthritis (17). 3 bilateral cases were seen in DDH and Perthes’ disease (Fig. 7). It was observed that most patients presented with limp (84), the second most common presentation was hip pain. (66) (Fig. 8).
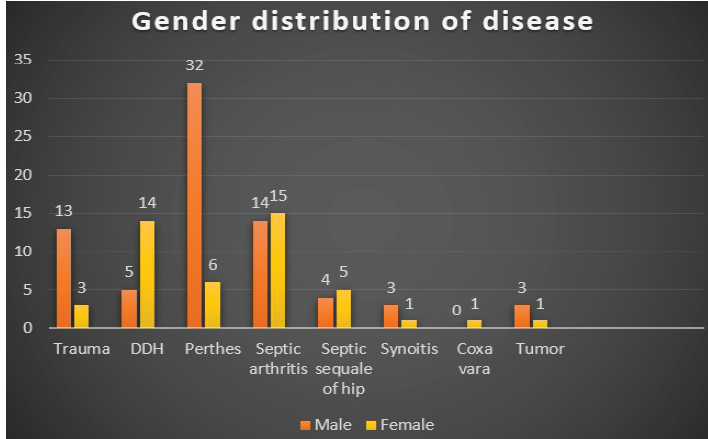
Figure 6: Chart showing the frequency distribution of various diseases in male and female.
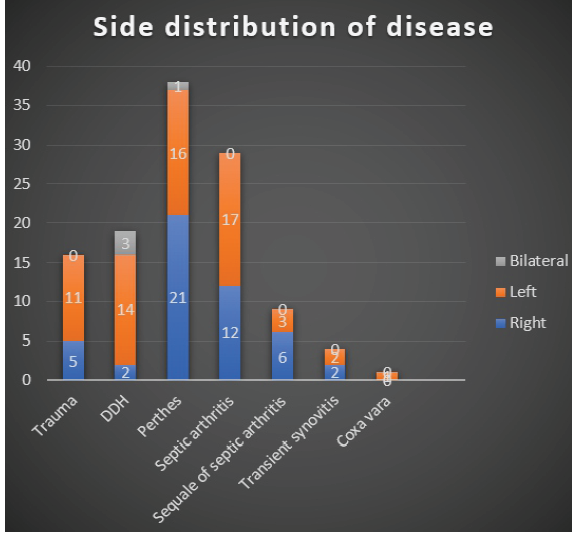
Figure 7: Chart showing the side distribution of various diseases in the study population.
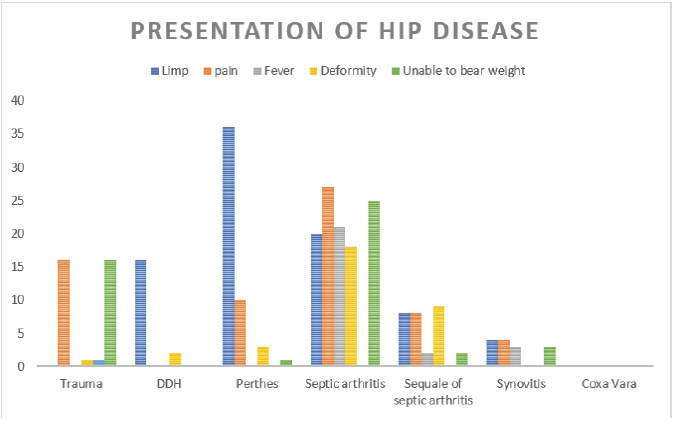
Figure 8: Chart showing various types of presentation of disease.
The study confirms a high burden of pediatric hip pathology, with an incidence of 2.05% among the screened population, which is higher than reported in other hospital-based or population studies [5]. This elevated figure likely reflects the status of IGIMS as a tertiary referral Center, attracting more complex and specialized cases from a broad catchment area across Eastern India.
Overview and prevalence
Our study screened 5830 patients aged <16 years. Among these, 120 patients had exclusive hip pathology (2.05%), with non-traumatic hip pathology accounting for 1.78%. This incidence is significantly higher than similar studies, such as Krul et al. [5] (0.06%) and Cristaldi et al. [6] (0.42%). The higher rate in our study is attributed to it being a hospital-based study at a tertiary care Center receiving an increased number of referrals for both acute and chronic conditions. The incidence of hip pathology peaked in the 5–11 years age group (44.5%), followed by 11–16 years (39.5%). The lowest incidence was in the 0–2 years group (6%). This aligns with findings by Cristaldi et al. [6] attributed to changes in vascular patterns, bone growth, and behavioral changes in this age bracket.
Gender based analysis of hip problems:
Considering all hip conditions together, males were 63% in our study population and 37% were females. In traumatic conditions 81.25% males and 18.75% females were affected (Ratio 4.33:1). This is consistent with a study done by Mirdad [7] and Azouz et al. [8], likely due to higher risk-taking behavior in males. In their study on etiology of atraumatic causes of limping child in Switzerland, Cristaldi et al. [6] found that 62% were males and 38% were females. Ragab et al. [9] in a MRI based study in Egypt on non-traumatic hip disorders found 55.6% males and 44.4% females were affected. The incidence of atraumatic hip pathology in our study is comparable with other studies. It also shows that geographical area doesn’t affect the gender incidence of atraumatic hip pathology. In our study, traumatic hip conditions were seen in 81.25% males and 18.75% females. The male vs female preponderance was 4.33: 1. In another study by Azouz et al. [8], the male incidence was 63%, and 37% were females. In a retrospective study done by Lee et al. [10] (2020) found that 68.1% males and 31.9% females were affected with fracture neck of femur. In our study, 84% males and 16% females were affected by Perthes’ disease. Rowe et al. [11] found a similar incidence as ours, that is, 82% males and 18% females. In India, a study done by Joseph et al. [4] found the overall male preponderance 72.22% and 27.78% in females. Overall, the findings in our study are comparable to the available data. In our study, the incidence of DDH was 26.32% in males and 73.68% in females. Goiano et al. [12] (2020) conducted a study in which they found that among DDH patients, 14.8% were males and 85.2% were females. Zhu and Zhu [13] (2022) conducted a study on USG-based screening of DDH and found the condition present in 82% females and 18% males. In all studies, female predominance is seen, as in our study. Among patients reporting with septic arthritis and its sequelae, in our study, 47.36% were males and 52.64% were females. In a systematic review on septic arthritis done by Nannini et al. [14], they found 54.3% were males and 45.7% were females. In a retrospective analysis on septic arthritis by Pääkkönen et al. [15], 51.61% were males and 48.38 were females. In contrast to previous studies, we found a female preponderance, which may be due to malnutrition and neglect of the female child. In our study, out of four patients who presented to us with transient synovitis 75% were males and 25% were females. These results are similar to the study done by Krul et al. [5] involving 66.6% males and 33.3% females. Vijlbrief et al. [16] conducted a study in the Dutch population on transient synovitis and found 73.68% males and 26.32% females were affected. In all studies on transient synovitis, the male preponderance was noted. In our study, four cases with tumors around hip region were included. We found 75% males and 25% females. Ruggieri et al. [17] conducted a retrospective study on musculoskeletal tumors from 1959 to 1999 in USA on 752 pediatric (0–14) patients with male predominance (64%) and females (36%). Choraria et al. [18] found that out of 59 pediatric patients with tumors around hip joint, 67.8% were males and 32.2% were females. Thus, our study results are comparable with previous studies. In our study, coxa vara was seen in only one patient. Hence, we could not comment on the incidence. As per the literature, this condition is equally seen in males and females [1].
Incidence of hip problems:
In our study, the incidence of traumatic hip condition was 2.7/1000 CHILDREN. In a study by Söylemez et al. [19], the incidence was 0.45/100 000 children aged ≤16 years. The incidence was higher in our study, as our study was patient-based. The incidence of various hip conditions shows variation on the basis of region also. In our study, the incidence of DDH was 3.26/1,000 live birth. This study result shows the incidence in Bihar, which is in the eastern part of India.
Kaushal et al. [20] (1976) reported the incidence of DDH 9.2/1,000 among 2,500 children in Chandigarh. Gupta et al. [21] observed the incidence of 18.7/1,000 in a study on 6,029 children in Delhi. All these cities are in northern part of India. Various studies have been done on DDH in South Indian states previously. Bhat and Babu [22] reported an incidence of 0.32/1,000 among 12,337 children in Pondicherry. Bhalvani and Madhuri [23] documented the incidence of to be 1/1,000 among 1,000 children in Vellore. The incidence of DDH was higher in northern states compared to southern states of India. It may be due to swaddling practices predominant in northern part of India [24]. In our study, we found the incidence of Perthes’ to be 6.52/1,000 in children presenting to our hospital with hip pathologies. Various studies from other countries have reported differing incidence rates of Perthes’ disease. Rowe et al. [11] conducted a retrospective study in South Korea to find out the incidence of Perthes; the incidence was 3.8/100,000, while Loder and Skopelja [25] documented a significantly higher incidence of 29/100,000 in Denmark. These variations in incidence may be influenced by factors such as race, ethnicity, and socioeconomic status Joseph et al. [4] conducted a questionnaire-based survey on Perthes’ disease which involved 16,838 school-attending children in Karnataka and Kerala. They found the incidence to be 0.5/100,000 in Vellore region and a higher incidence of Perthes’ disease, with an incidence of 4.4/100,000 in Udupi. The higher incidence of Perthes’ disease in our study can be attributed to our hospital-based study and being a tertiary referral Centre so we mostly get specialized cases. In our study, the incidence of infective arthritis and its sequelae was 49/10,000 patients. Incidence of infective arthritis was 2–6/10,000 population according to a systematic review by Momodu and Savaliya [26]. According to Krogstad et al. [27], the annual incidence of septic arthritis was 4–5 children per 10,000 population in developed countries. The incidence of septic arthritis in our region is high, which may be due to poor hygiene practices, low socioeconomic status, and poor penetration of health care policies. The incidence of transient synovitis in our study was 0.00045/100,000 person years. In a study done by Krul et al. [5] in Dutch population, they found the incidence of transient synovitis of 76.2/100,000 person years. The incidence of transient synovitis in our study was less, which may be due to self-resolution of this condition, lack of awareness among the border and rural areas, and lack of adequate connectivity from the peripheral areas. The incidence of tumors in our study was 0.69/1,000 population. Arndt et al. [28] found the incidence of tumor in children 4.4 per million. In our study, we found Ewing sarcoma proximal femur (1), Osteoid osteoma greater trochanter (1), Benign lytic lesion in neck of femur (1), and Aneurysmal bone cyst (1). The incidence in our study is higher, as our study is hospital-based and their study is based on population.
Disease distribution according to age group:
In our study, 13.33% patients had traumatic hip conditions. Out of all hip pathology maximum traumatic hip conditions were in the age group of 11–16 years (56.25%) followed by 5–11 years of age group (43.75%), In a study done by Ratliff [29] on 71 pediatric patients of proximal femur fracture, the maximum number of patients were in the age group of 11–15 year (60.56%) followed by 14.08% in 5–11 year age group. In a study on pediatric femoral neck fracture in children, Azouz et al. [8] found that the maximum no of patients were in the age group of 10–13 years. Thus our results were similar to previous studies. The hip trauma is noticed high in late childhood and adolescent age group. It may be due to high-impact sports and risk-taking behavior. In non-traumatic hip conditions, most of the DDH patients reported in the 2–5 years age group (47.36%), followed by 5–11 years age group (31.57%). This data correlates with the study done by Rebello and Joseph [30] (2003). They found that 47% of children (19/44) affected with DDH presented in the age group of 1–5 years. Tej et al. [31] found maximum prevalence of DDH in the age group 1–5 years (82.92%).In all these studies, by 5 years of age, most of the patients with DDH presented to the physician. In our study, Perthes’ disease presented mostly in 5–11 years of age (68.42%). Our results were similar to the systematic review conducted by Loder and Skopelja [25] (2011). They found the most common age group affected by Perthes’ was 4–8 years. According to Johansson et al. [32], the mean age of diagnosis of Perthes’ was 8 years in males and 9 years in females. Our observation was comparable with their studies on Perthes’ disease. In our study, infective conditions and its sequelae most commonly presented in the 11–16 years age group (55.17%), followed by 37.9% in 5–11 years age group and 6.8% in 0–2 year of age group. In a retrospective study conducted by Mills and Burroughs [33] in Singapore on 75 patients (<16 years age) on septic arthritis from 1999 to 2014, they found that the maximum no of cases were in the age group of 4–10 years (37%), followed by 26% in 10–16 years age group. Possibly the cause of the difference compared to our study is due to difference in the healthcare access, lower literacy rate, awareness, and doctor- patient ratio. The incidence is lower in children <5 years of age because in infancy, it often presents with atypical or minimal symptoms, leading to delayed diagnosis. The prevalence of transient synovitis in our study was 75% in the age group of 11–16 years and 25% in the 5–11 years age group. Cristaldi et al. [6] found the maximum no of transient synovitis (56.96%) in the age group of 3–10 year. In our study, the reporting of transient synovitis was late compared to other study. It may be due to poor healthcare access, low awareness, and early resolution in lesser age group. The mean age of presentation of tumors in our study was 10 years. Ruggieri et al. [17] found the mean age of presentation 9 years. In our study, one coxa vara patient presented at age of 9 year The mean age of presentation was 9.4 year according to study done by Aarabi et al. [34].
Percentage distribution of various disease:
Considering all hip conditions, atraumatic conditions were more common in pediatric population presenting to us. Perthes’ disease was the commonest in our study, that is, 32%. It was followed by infective arthritis and its sequelae 31.5%, developmental hip dysplasia 16%, traumatic hip conditions 13%, post-septic sequelae 7.5%, transient synovitis 3.4%, and tumors around the hip 3.4%. Krul et al. [5] studied the incidence and presentation of non-traumatic hip pathology in 2010. They found that transient synovitis was the most common condition at (46%) followed by Perthes’ disease (7%) and SCFE was (3.5%). Cristaldi et al. [6] found that transient synovitis was the most common cause in 34% patients with limping. In our study, transient synovitis incidence is low, that is, 3.4%, which can be attributed to self-limiting nature of the disease and delayed presentation to our institute due to lack of connectivity in the rural and border areas, widespread quack practices and lack of awareness.
Side distribution of disease:
In traumatic cases, the majority of the cases were left sided 68.75%, in right side 31.25%. Our results were similar to the study done by Lee et al. [10] in China for traumatic neck of femur fracture in children, that is, 77.8% were left-sided, and 22.2% were right side. In our study, Perthes’ was predominantly present on the right side (55.26%), the left side was affected in 42.12%, and 2.6% cases were bilateral. Similar results were found by Rowe et al. [11] (2005). They found 52% right side involvement and 48% left side involvement. In our study, DDH was predominantly left-sided (73.68%), right-sided involvement was 10.52%, and bilateral was 15.78%. Similar observation was found by Sharpe et al. [35]. They observed 66.66% cases were left-sided and 11.11% right side, 22.22% cases were bilateral. Loder and Skopelja [24] (2011) found the similar results in DDH, left side predominance in (60%), right side was affected in 37% and bilateral in 3% cases. Some studies suggest developmental asymmetries and intrauterine positioning may contribute to this phenomenon in DDH [24]. In our study, on septic arthritis and its sequelae, 41.38% had right-sided affection and 58.62% were left-sided. In contrast, a study done by Ahmad et al. [36] in 52 children of the eastern Indian state with acute septic arthritis, 44.23% patients were right-sided, 36.53% were left-sided, and 19.23% cases were bilateral. In a systematic review, Nannini et al. [14] concluded that the right side is more affected. Hence, in our study, the dominant side is different from previous studies. In transient synovitis, both sides were equally affected in our study. Ehrendorfer et al. [37] noted left-sided predilection in 66.07% patients and right-sided involvement in 33.92% patients. Similar to transient synovitis, tumors around the hip were equally seen in left and right side. In a study done by Choraria et al. [18] on children affected with tumors around the hip joint, the right hip was involved in 31 (52.5%) children, the left hip in 27 (45.8%), while one child (1.7%) had bilateral hip involvement. Only one case of Coxa Vara presented to us, where side affected cannot be judged. As per the present literature, no data are given on the side distribution. Ranade et al. [38] found the bilateral cases 42.4% and unilateral in 57.6%.
Clinical presentation of disease:
The patients of hip pathology usually presented with a variety of clinical symptoms, including limp, pain, fever, deformity, limb shortening, and inability to bear weight. Limping was the most common presenting symptom observed in 70.83% of cases, followed by pain in 57.5%, refusal to bear weight in 39.66%, deformity in 27.5%, and fever in 21.66%. Pain was the most frequent symptom reported in our study. It was present in 100% case of trauma and synovitis. It was a major symptom in septic hip conditions and tumors around the hip, but inconsistent in Perthes disease, Nelitz et al. [39] found that only 25% of Perthes’ disease presented with pain. In a study done by Cristaldi et al. [6], pain was present in 84.92% cases of transient synovitis and septic arthritis. Limp was the second most common symptom reported. It was a major symptom in cases of DDH and Perthes’ disease. Those with LLD due to sepsis and coxa vara also presented with limp. The same was mentioned by Momodu and Savaliya [26], limp as presentation was most commonly reported in Perthes’ disease (94.73% cases). Cristaldi et al. [6] reported that limp was seen in all patients of Perthes’. This finding is consistent with the reports by Joseph et al. [4] (1988) for Perthes’ disease, who described limp as a common presenting complaint. In our study, 84.21% patients of DDH presented with limp. Dezateux and Rosendahl [40], 2007 found that 89.47% cases of DDH presented with limp. Thus, our results were similar to others study. In our study, limp was seen in 65.78% of septic arthritis and its sequelae. Paakonen found that limping was present in 90% cases of septic arthritis. Our results differ from Paakonen [15] as the majority of patients presented late and were unable to bear weight. In our study, all patients of transient synovitis presented with limping. Fischer and Baettie [41] conducted a study on limping children and found 39.5% patients of transient synovitis presented with limping. Painless limp is seen in coxa vara, which is due to shortening. In our study, fever was primarily associated with septic arthritis (68.42% cases). Our results were similar to a study done by Momodu and Savaliya [26], they found that fever was associated in 40–60% of patients with septic arthritis. Fever was also present in 75% cases of transient synovitis in our study. Whitelaw and Varacallo [42] (2024) found that 50% patients of septic arthritis and 30% of patients of transient synovitis presented with fever. Compared to Whitelaw and Varacallo, the fever as a presenting symptom in transient synovitis was high. It may be due to the higher age group of patients in our study. Inability to bear weight was the most common presentation in trauma (87.5%). About 12.5% cases of traumatic hip conditions were able to bear weight, as these patients were of traumatic SCFE, there were largely asymptomatic. About 75% of transient synovitis patient were unable to bear weight in our study. About 78% patients of septic arthritis and its sequelae were unable to bear weight in our study. Donders et al. [43] study showed that 50% of patients affected with septic arthritis presented with refusal to bear weight. According to a study done by Momodu and Savaliya [26], >60% of patients of transient synovitis and septic arthritis presented with refusal to bear weight. The results in our study are comparable.
Time duration of disease presentation:
In our study, 56.25% traumatic cases were reported within 48 h. While 43.75% traumatic cases were reported late, usually after 4 weeks, due to paucity of symptoms. In our study of traumatic conditions, we included traumatic SCFE which were presenting usually after 4 weeks. Traumatic SCFE patients were able to walk, and their pain was minimal. The study done by Green et al. [44] (2022) on SCFE found that the average delay in presentation was 2.5 months and 52% incidence of apparent missed diagnosis for SCFE by the primary care system. In our study, 68.4% of DDH presented late, missing the period of non-surgical management. Higher percentage of late-presenting DDH in our region is due to a lack of screening system, a large rural population, and a lack of referral system. The incidence of late-presenting DDH in our study was 4.37/1000 study population. In a study done by Sharpe et al. [35], the prevalence of late diagnosed DDH (>3 months) was 0.15 cases per 1000 live births. Our study has a higher percentage of late-presenting DDH due to a lack of screening system, a large rural population, and a lack of referral system. In Perthes disease, 55% of our cases presented after the age of >7 years. The Perthes disease study by Joseph et al. [4] found that older children are more likely to have greater epiphyseal extrusion in 40% of cases. In Septic arthritis, 86.97% of our cases presented late after 5 days. In a study done by Chand et al. [45] on septic arthritis, all cases presented late, that is, >5 days. It may be due to trial of medicines at home or in pre-hospital setting. Nearly half (36.66%) of the children in our study had received some form of treatment before presenting to IGIMS. 6.66% had undergone operative treatment. However, the majority had not been managed (55%) properly, pointing to delayed referrals, lack of awareness, and possible gaps in primary healthcare infrastructure. This underlines the need for improving early detection strategies and awareness among frontline healthcare workers.
Geographical distribution of disease:
An analysis of patient distribution by district in our study reveals that the highest number of cases reported from East Champaran (15), Saharsa (11), and Patna (10). Moderate frequencies were observed from Muzaffarpur (8), Samastipur (8), Araria (7), Bhagalpur (6), Purnea (5), Vaishali (5), and Madhubani (5). In contrast, districts such as Kishanganj, Supaul, Darbhanga, Ara, Katihar, Jehanabad, Nawada, Madhepura, Gopalganj, Nalanda, Lakhisarai, Sheohar, Buxar, Aurangabad, and Arwal reported fewer cases (1–4), which may be due to smaller populations, better access to primary healthcare facilities, or lower referral rates to our center. The geographical distribution predominantly covers northern and northeastern Bihar, aligning with the catchment area of our tertiary care center. The higher frequency of cases from certain districts like East Champaran and Saharsa may be influenced by factors such as population density, healthcare access, and regional disease prevalence. The incidence of hip problems in Patna is higher due to easy access to healthcare services. Overall, our findings underscore the significant burden of pediatric hip pathologies in Eastern India, a problem that is heavily exacerbated by delayed presentations and systemic gaps in primary healthcare screening. However, when interpreting these results, several methodological and practical constraints must be considered. While our study provides valuable insights into pediatric hip pathology in Eastern India, our study encountered several limitations which must be acknowledged.
Limitations
- Single-Center, hospital-based study the study was conducted at a single tertiary care referral Center (IGIMS, Patna), which likely over represents complex and late-stage cases, limiting generalizability to the broader community population.
- Referral bias as a tertiary referral Center, the hospital receives complicated and advanced cases, potentially inflating the apparent incidence and severity of certain pathologies such as Perthes’ disease and septic arthritis.
- Cross-sectional design being a cross-sectional observational study, causal relationships and disease progression patterns cannot be established.
- Limited external validity findings may not be applicable to other regions of India or rural primary-care settings due to differences in healthcare access, socioeconomic factors, and screening practices.
- Incidence calculation constraints the reported “incidence” is hospital-based (2.05% among attendees) rather than true population-based incidence, which may misrepresent actual community prevalence.
- Short study duration (18 months) an 18-month study period may not adequately account for seasonal variation, long-term trends, or fluctuations in referral patterns.
- Exclusion of incomplete cases 15 patients were excluded due to incomplete workup or denial of consent, which could introduce selection bias.
- Lack of longitudinal follow-up the study focuses on presentation patterns and incidence without long-term follow-up data regarding functional outcomes, complications, or disease progression.
- Potential diagnostic variability although standardized investigations were performed, diagnostic confirmation relied on clinician judgment and imaging interpretation, which may introduce inter-observer variability.
- Absence of standardized severity grading conditions, such as DDH, Perthes’ disease, and septic arthritis were not stratified using validated severity classifications (e.g., Catterall, Herring, Tönnis), limiting deeper clinical correlation.
- Limited socioeconomic data analysis although socioeconomic factors are discussed, the study does not quantitatively analyze income, parental education, nutritional status, or healthcare accessibility.
- Underrepresentation of self-limiting conditions transient synovitis appears underrepresented, possibly due to spontaneous resolution or lack of tertiary referral, leading to spectrum bias.
- Potential reporting bias in late presentation data definition of “late presentation” may vary between conditions and was not uniformly standardized across diagnoses.
- No multivariate statistical analysis only descriptive statistics were used; risk factor analysis or regression modeling could have identified predictors of late presentation or specific pathologies.
- Geographic distribution interpretation limitations district-wise case distribution may reflect referral patterns rather than true regional disease burden, limiting epidemiological accuracy.
This study provides vital region-specific epidemiological data on pediatric hip pathology in Eastern India. The spectrum is dominated by Perthes’ disease, infective arthritis, and DDH. The high proportion of cases presenting late – especially DDH missing the window for non-surgical treatment and septic arthritis delaying life-altering intervention – is the most critical finding. Addressing these late presentations requires urgent public health intervention focusing on:
1. Establishing universal neonatal hip screening for DDH.
2. Educating primary healthcare providers and pediatricians on recognizing “red-flag” signs (fever, inability to bear weight) for infective conditions.
3. Developing streamlined referral protocols to improve timely access to tertiary care.
Further multicentric studies are necessary to validate these regional trends and inform the development of robust, region-specific management protocols.
Pediatric hip disorders in Eastern India are predominantly non-traumatic, with Perthes’ disease, infective arthritis, and DDH forming the major disease burden. A significant proportion of children present late, particularly those with DDH and septic arthritis, thereby missing the critical window for early, non-operative or joint-preserving management early neonatal screening for DDH and improved awareness at the primary care level are essential to prevent long-term disability. Timely referral to tertiary Centers can significantly reduce complications such as deformity, limb length discrepancy, avascular necrosis, and early osteoarthritis. Strengthening early detection systems, establishing universal hip screening programs, and educating frontline healthcare providers are critical steps to reduce preventable morbidity from pediatric hip pathologies in this region.
References
- 1. Herring JA. Tachdjian’s Pediatric Orthopaedics. 5th ed. Philadelphia, PA: Saunders; 2014. [Google Scholar] [PubMed]
- 2. Ribeiro SC, Barreto KS, Alves CB, Almendra Neto OL, Da Nóbrega MV, Braga LR. Hip pain in childhood. Radiol Bras 2020;53:63-8. [Google Scholar] [PubMed]
- 3. Palocaren T. Femoral neck fractures in children: A review. Indian J Orthop 2018;52:501-6. [Google Scholar] [PubMed]
- 4. Joseph B, Chacko V, Rao BS, Hall AJ. The epidemiology of Perthes’ disease in South India. Int J Epidemiol 1988;17:603-7. [Google Scholar] [PubMed]
- 5. Krul M, Van Der Wouden JC, Schellevis FG, Van Suijlekom-Smit LW, Koes BW. Acute non-traumatic hip pathology in children: Incidence and presentation in family practice. Fam Pract 2010;27:166-70. [Google Scholar] [PubMed]
- 6. Cristaldi S, Boni A, Ferro V, Musolino A, Della Vecchia N, Boccuzzi E, et al. Atraumatic limping child, a challenge for pediatricians: An observational age-related study in a pediatric emergency department. Children (Basel) 2024;11:185. [Google Scholar] [PubMed]
- 7. Mirdad T. Fractures of the neck of femur in children: An experience at the Aseer Central Hospital, Abha, Saudi Arabia. Injury 2002;33:823-7. [Google Scholar] [PubMed]
- 8. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC. Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-20. [Google Scholar] [PubMed]
- 9. Ragab Y, Nabih M, Aly I, Kamal A, Abd-Allah MA, El-Refai R, et al. Magnetic resonance imaging features of hip disorders in an Egyptian pediatric population. Reumatismo 2015;67:68-77. [Google Scholar] [PubMed]
- 10. Lee C, Chau WW, Illescas V, Ng BK. Twenty years of experience of fracture neck of femur in pediatric population in Southern China. J Orthop Joint Surg 2020;2:26-30. [Google Scholar] [PubMed]
- 11. Rowe SM, Jung ST, Lee KB, Bae BH, Cheon SY, Kang KD. The incidence of Perthes’ disease in Korea: A focus on differences among races. J Bone Joint Surg Br 2005;87:1666-8. [Google Scholar] [PubMed]
- 12. Goiano O, Akkari M, Pupin JP, Santili C. The epidemiology of developmental dysplasia of the hip in males. Acta Ortop Bras 2020;28:26-30. [Google Scholar] [PubMed]
- 13. Zhu D, Zhu H. Incidence and epidemiological characters of developmental dysplasia of the hip in Lianyungang: Based on ultrasound screening: A retrospective study. Int J Gen Med 2022;15:8547-55. [Google Scholar] [PubMed]
- 14. Nannini A, Giorgino R, Bianco Prevot L, Bobba A, Curci D, Cecchinato R, et al. Septic arthritis in the pediatric hip joint: A systematic review of diagnosis, management, and outcomes. Front Pediatr 2023;11:1311862. [Google Scholar] [PubMed]
- 15. Pääkkönen M, Kallio MJ, Peltola H, Kallio PE. Pediatric septic hip with or without arthrotomy: Retrospective analysis of 62 consecutive nonneonatal culture-positive cases. J Pediatr Orthop B 2010;19:264-9. [Google Scholar] [PubMed]
- 16. Vijlbrief AS, Bruijnzeels MA, Van Der Wouden JC, Van Suijlekom-Smit LW. Incidence and management of transient synovitis of the hip: A study in Dutch general practice. Br J Gen Pract 1992;42:426-8. [Google Scholar] [PubMed]
- 17. Ruggieri P, Angelini A, Montalti M, Pala E, Calabrò T, Ussia G, et al. Tumours and tumour-like lesions of the hip in the paediatric age: A review of the Rizzoli experience. Hip Int 2009;19 Suppl 6:S35-45. [Google Scholar] [PubMed]
- 18. Choraria A, O’Donnell P, Saifuddin A. Differential diagnosis of hip pain in children referred to a specialist bone tumour service. Br J Radiol 2022;95:20211397. [Google Scholar] [PubMed]
- 19. Söylemez MS, Bingöl İ, Yaşar NE, Dumlupınar E, Ayvalı MO, Ata N, et al. Epidemiology and demographics of pediatric proximal femur fractures in Türkiye: Results from a government-based health registry. J Pediatr Orthop B 2024;33:443-51. [Google Scholar] [PubMed]
- 20. Kaushal V, Kaushal SP, Bhakoo ON. Congenital dysplasia of the hip in Northern India. Int Surg 1976;61:29. [Google Scholar] [PubMed]
- 21. Gupta AK, Kumari S, Arora PL, Kumar R, Mehtani AK, Sood LK. Hip instability in newborns in an Urban community. Natl Med J India 1992;5:269-72. [Google Scholar] [PubMed]
- 22. Bhat BV, Babu L. Congenital malformations at birth–a prospective study from South India. Indian J Pediatr 1998;65:873-81. [Google Scholar] [PubMed]
- 23. Bhalvani C, Madhuri V. Ultrasound profile of hips of South Indian infants. Indian Pediatr 2011;48:475-7. [Google Scholar] [PubMed]
- 24. Loder RT, Skopelja EN. The epidemiology and demographics of hip dysplasia. ISRN Orthop 2011;2011:238607. [Google Scholar] [PubMed]
- 25. Loder RT, Skopelja EN. The epidemiology and demographics of legg- calvé-perthes’ disease. ISRN Orthop 2011;2011:504393. [Google Scholar] [PubMed]
- 26. Momodu II, Savaliya V. Septic arthritis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/nbk538176 [Accessed May 15, 2025]. [Google Scholar] [PubMed]
- 27. Krogstad P. Osteomyelitis and septic arthritis. In: Feigin RD, Cherry JD, editors. Textbook of Pediatric Infectious Diseases. 6th ed. Philadelphia, PA: Saunders; 2009. p. 725-48. [Google Scholar] [PubMed]
- 28. Arndt CA, Rose PS, Folpe AL, Laack NN. Common musculoskeletal tumors of childhood and adolescence. Mayo Clin Proc 2012;87:475-87. [Google Scholar] [PubMed]
- 29. Ratliff AH. Fractures of the neck of the femur in children. J Bone Joint Surg Br Vol 1962;44B:528-42. [Google Scholar] [PubMed]
- 30. Rebello G, Joseph B. Developmental dysplasia of the hip in children from Southwest India-will screening help? Indian J Orthop 2003;37:210-4. [Google Scholar] [PubMed]
- 31. Tej BY, Shetty BC, Hegde AH. Evaluation of avascular necrosis during midterm follow up in DDH cases treated by single stage surgery in the walking age group. J Crit Rev 2020;7:4251-9. [Google Scholar] [PubMed]
- 32. Johansson T, Lindblad M, Bladh M, Josefsson A, Sydsjö G. Incidence of Perthes’ disease in children born between 1973 and 1993. Acta Orthop 2017;88:96-100. [Google Scholar] [PubMed]
- 33. Mills S, Burroughs KE. Legg-calve-perthes disease. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. [Google Scholar] [PubMed]
- 34. Aarabi M, Rauch F, Hamdy RC, Fassier F. High prevalence of coxa vara in patients with severe osteogenesis imperfecta. J Pediatr Orthop 2006;26:24-8. [Google Scholar] [PubMed]
- 35. Sharpe P, Mulpuri K, Chan A, Cundy PJ. Differences in risk factors between early and late diagnosed developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed 2006;91:158-62. [Google Scholar] [PubMed]
- 36. Ahmad E, Singh P, Pradhan P, Singh VK, Sharma B. Epidemiological and clinical profiles of septic arthritis in children of 0-2 years of age in Eastern Uttar Pradesh, India . Int J Contemp Pediatr [Internet]. 2024 May 27 [cited 2026 Mar. 28];11(6):757-62. Available from: https://www.ijpediatrics.com/index.php/ijcp/article/view/6037 [Google Scholar] [PubMed]
- 37. Ehrendorfer S, LeQuesne G, Penta M, Smith P, Cundy P. Bilateral synovitis in symptomatic unilateral transient synovitis of the hip: An ultrasonographic study in 56 children. Acta Orthop Scand 1996;67:149-52. [Google Scholar] [PubMed]
- 38. Ranade A, McCarthy JJ, Davidson RS. Acetabular changes in coxa vara. Clin Orthop Relat Res 2008;466:1688-91. [Google Scholar] [PubMed]
- 39. Nelitz M, Lippacher S, Krauspe R, Reichel H. Perthes disease: Current principles of diagnosis and treatment. Dtsch Arztebl Int 2009;106:517-23. [Google Scholar] [PubMed]
- 40. Dezateux C, Rosendahl K. Developmental dysplasia of the hip. Lancet 2007;369:1541-52. [Google Scholar] [PubMed]
- 41. Fischer SU, Beattie TF. The limping child: Epidemiology, assessment and outcome. J Bone Joint Surg Br 1999;81:1029-34. [Google Scholar] [PubMed]
- 42. Whitelaw CC, Varacallo MA. Transient synovitis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. [Google Scholar] [PubMed]
- 43. Donders CM, Spaans AJ, Van Wering H, Van Bergen CJ. Developments in diagnosis and treatment of paediatric septic arthritis. World J Orthop 2022;13:122-30. [Google Scholar] [PubMed]
- 44. Green DW, Reynolds RA, Khan SN, Tolo V. The delay in diagnosis of slipped capital femoral epiphysis: A review of 102 patients. HSS J 2005;1:103-6. [Google Scholar] [PubMed]
- 45. Chand S, Srivastava S, Afaque SF, Yadav A, Verma V, Qidwai S, et al. Late-presenting septic arthritis of the hip in children: Variations in presentation and a review of 25 hips after surgical debridement. Cureus 2023;15:e47717 [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A 5-Year Outcome of Closed Reduction and Screw Fixation for an Atypical Slipped Capital Femoral Epiphysis Associated with Hypogonadism: A Case Report
June 1, 2026 A 5-Year Outcome of Closed Reduction and Screw Fixation for an Atypical Slipped Capital Femoral Epiphysis Associated with Hypogonadism: A Case Report May 1, 2026 Delayed Slipped Capital Femoral Epiphysis Following Surgical Fixation of a Femoral Neck Fracture in a Child: A Rare Case Report
May 1, 2026 Delayed Slipped Capital Femoral Epiphysis Following Surgical Fixation of a Femoral Neck Fracture in a Child: A Rare Case Report April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report
April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report February 1, 2026 A Prospective Study of Comparison between Stable and Unstable Pediatric Femoral Shaft Fractures Treated With Titanium Elastic Nails
February 1, 2026 A Prospective Study of Comparison between Stable and Unstable Pediatric Femoral Shaft Fractures Treated With Titanium Elastic Nails