
Intra-articular osteoid osteoma can resemble femoroacetabular impingement and delay diagnosis.
Dr. Mario Martínez-Villalobos, Shriners Hospital for Children - Hip Preservation Clinic and Arthroscopic Clinic, ABC Medical Center, Mexico City, Mexico. E-mail: drmariomartinez@yahoo.com.mx
Abstract
Introduction: Intra-articular osteoid osteoma (OO) of the hip often presents with atypical symptoms and may mimic femoroacetabular impingement, leading to delayed diagnosis.
Case Report: A 15-year-old girl presented with 2 years of right groin pain and restricted hip motion. Imaging revealed an intra-articular OO at the femoral head–neck junction. Surgical hip dislocation allowed complete excision of the nidus and restoration of the femoral head–neck offset. At 2-year follow-up, the patient was pain‑free with a full range of motion and no signs of impingement.
Conclusion: Surgical hip dislocation provides full access to the femoral head–neck junction and enables safe, complete resection of intra-articular OO in adolescents.
Keywords: Osteoid osteoma, femoroacetabular impingement, hip dislocation, adolescent, musculoskeletal pain, range of motion.
Osteoid osteoma (OO) is a benign bone tumor representing approximately 11% of benign bone tumors and 3% of all primary bone tumors. More than half occur in the long bones of the lower extremities, with the proximal femur being the most common location [1]. Intra-articular OO is uncommon, accounting for 5–12% of cases, and the hip is the joint most frequently affected [2]. Clinical manifestations and radiographic findings differ between intra-articular and extra-articular lesions. Patients often present with joint pain and restricted range of motion, which may lead clinicians to misattribute symptoms to primary joint pathology, delaying diagnosis [3].
Treatment options for symptomatic intra-articular OO include open excision, radiofrequency ablation, and arthroscopic resection [4]. Surgical hip dislocation, as described by Ganz et al., provides full access to the femoral head and acetabulum while minimizing the risk of avascular necrosis [5]. Although originally described for adults, this approach has been successfully applied in children and adolescents with hip disorders [6,7,8].
This report describes an intra-articular OO of the hip in an adolescent treated with surgical hip dislocation at a younger age than most previously reported cases using this approach. Informed consent for publication was obtained.
A 15-year-old girl presented with a 2-year history of right groin pain. Symptoms improved temporarily with analgesics and nonsteroidal anti‑inflammatory drugs, but worsened with physical activity during the previous 6 months. She denied any history of trauma. Physical examination revealed a limping gait, visible thigh muscle atrophy, and restricted hip flexion and internal rotation due to pain.
Anteroposterior pelvic radiographs were unremarkable. Computed tomography (CT) revealed a nidus consistent with OO, and magnetic resonance arthrography demonstrated anterior bone marrow edema at the femoral head–neck junction (Fig. 1).
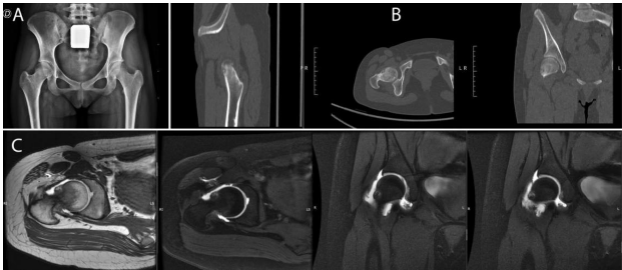
Figure 1: Imaging studies. (a) Normal appearing anteroposterior pelvic radiograph. (b) Computed tomography scan showing the osteoid osteoma nidus. (c) Magnetic resonance arthrography demonstrating anterior cortical prominence and bone marrow edema at the femoral head–neck junction.
A surgical hip dislocation was performed using the Ganz technique. After capsulotomy, 20 mL of hemorrhagic synovial fluid was aspirated. On dislocation of the femoral head, an anterior cortical prominence was identified at the femoral head–neck junction. The lesion measured approximately 1 × 1 cm. Dynamic assessment revealed that the prominence impinged beneath the anterior labrum, producing femoroacetabular impingement (FAI)–type contact. The labrum and acetabular cartilage were intact.
The lesion was excised, and the femoral head-neck offset was restored by resecting the anterior cortical bone until full sphericity of the femoral head was achieved (Fig. 2). After reduction, intraoperative assessment confirmed full, impingement-free hip motion.
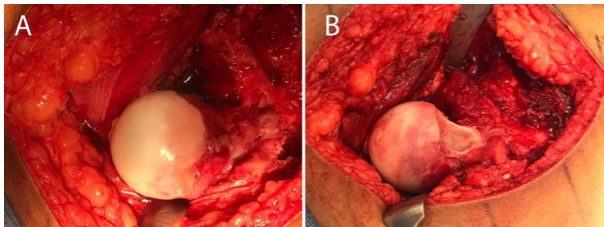
Figure 2: Intraoperative findings. (a) Anterior cortical prominence and hemorrhagic synovitis. (b) Resection of the osteoid osteoma and restoration of the femoral head–neck offset.
Post-operative management included partial weight-bearing with crutches and limiting hip flexion to 90° for 6 weeks. The patient then began a physical therapy program to restore range of motion and strength. Histological analysis confirmed the diagnosis of OO.
At 2-year follow-up, the patient was pain-free, with normal gait, full range of motion, and no clinical or radiographic signs of FAI (Fig. 3).
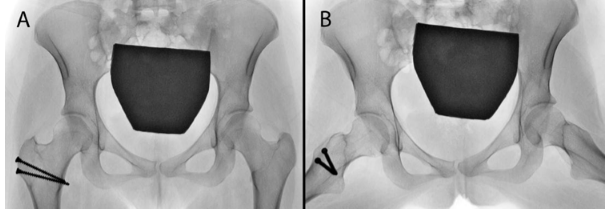
Figure 3: Two-year follow-up radiographs showing normal hip morphology. (a) Anteroposterior pelvis radiograph. (b) Lowenstein’s view of the pelvis.
Intra‑articular OO of the hip often presents atypically, leading to delayed diagnosis. May et al. reported diagnostic delays exceeding 6 months in 43% of pediatric and adolescent patients, with some undergoing surgery for presumed alternative hip disorders before the OO was identified [4]. Our patient experienced a 2-year delay due to nonspecific symptoms.
OO may mimic FAI. Pianta et al. described a 16-year-old athlete whose intra-capsular OO produced cortical changes resembling early Cam deformity, ultimately requiring lesion ablation but leaving residual motion restriction [9]. Similarly, Spiker et al. reported that many of the patients with intra-articular OO exhibited FAI-like symptoms, with several requiring Cam decompression in addition to lesion resection [2].
Surgical hip dislocation has been shown to be safe and effective in adolescents with various hip disorders [6,7,8]. Mainzer et al. reported successful treatment of an 18-year-old with intra‑articular OO using this approach, achieving complete symptom resolution [10].
Our patient represents one of the youngest reported cases treated with surgical hip dislocation for intra-articular OO. This approach provided full visualization of the femoral head–neck junction, allowed complete excision of the nidus, and enabled dynamic assessment to ensure restoration of impingement-free motion. At 2-year follow-up, the patient remains asymptomatic with excellent functional outcomes.
Intra-articular OO of the hip may mimic FAI and lead to delayed diagnosis in adolescents. CT and magnetic resonance arthrography are valuable tools for identifying the nidus. Surgical hip dislocation offers full access to the femoral head-neck junction and allows safe, complete resection of intra-articular lesions while preserving vascularity.
Intra-articular osteoid osteoma of the hip may mimic femoroacetabular impingement and lead to delayed diagnosis in adolescents. Surgical hip dislocation provides full access to the femoral head–neck junction, allowing safe and complete resection of the nidus with excellent functional outcomes.
References
- 1. Lee EH, Shafi M, Hui JH. Osteoid osteoma: A current review. J Pediatr Orthop 2006;26:695-700. [Google Scholar] [PubMed]
- 2. Spiker AM, Rotter BZ, Chang B, Mintz DN, Kelly BT. Clinical presentation of intra-articular osteoid osteoma of the hip and preliminary outcomes after arthroscopic resection: A case series. J Hip Preserv Surg 2018;5:88-99. [Google Scholar] [PubMed]
- 3. Song MH, Yoo WJ, Cho TJ, Chung CY, Park MS, Cheon JE, et al. Clinical and radiological features and skeletal sequelae in childhood intra-/juxta-articular versus extra-articular osteoid osteoma. BMC Musculoskelet Disord 2015;16:3. [Google Scholar] [PubMed]
- 4. May CJ, Bixby SD, Anderson ME, Kim YJ, Yen YM, Millis MB. Osteoid osteoma about the hip in children and adolescents. J Bone Joint Surg Am 2019;101:486-93. [Google Scholar] [PubMed]
- 5. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-24. [Google Scholar] [PubMed]
- 6. Guindani N, Eberhardt O, Wirth T, Surace MF, Fernandez FF. Surgical dislocation for pediatric and adolescent hip deformity: Clinical and radiographical results at 3 years follow-up. Arch Orthop Trauma Surg 2017;137:471-9. [Google Scholar] [PubMed]
- 7. Rebello G, Spencer S, Millis MB, Kim YJ. Surgical dislocation in the management of pediatric and adolescent hip deformity. Clin Orthop Relat Res 2009;467:724-31. [Google Scholar] [PubMed]
- 8. Shin SJ, Kwak HS, Cho TJ, Park MS, Yoo WJ, Chung CY, et al. Application of Ganz surgical hip dislocation approach in pediatric hip diseases. Clin Orthop Surg 2009;1:132-7. [Google Scholar] [PubMed]
- 9. Pianta M, Crowther S, McNally D, Panu A, Lambert RG. Proximal femoral intra-capsular osteoid osteoma in a 16-year-old male with epiphyseal periostitis contributing to Cam-type deformity relating to femoro-acetabular impingement. Skeletal Radiol 2013;42:129-33. [Google Scholar] [PubMed]
- 10. Mainzer J, Ganz R, Tibor L, Leunig M. Not all hip pain is impingement: Femoral neck osteoid osteoma in a patient with a coexisting cam deformity: A case report. JBJS Case Connect 2012;2:e31. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases
June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases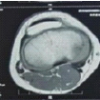 June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum
June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum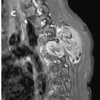 June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report
June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report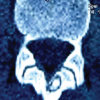 May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report
May 1, 2026 Navigation-Assisted Endoscopic Excision of Lumbar Vertebral Osteoid Osteoma: A Case Report