
High-energy lumbar burst fractures with laminar involvement should raise suspicion for traumatic dural tears and occult nerve root entrapment, which may only be identified intraoperatively and require meticulous decompression to prevent iatrogenic neurological injury.
Dr. Dileepan Chakrawarthi, Department of Orthopedic Surgery, Soundarapandian bone and joint hospital and Research Institute, Chennai, Tamil Nadu, India. E-mail: chakdileep@gmail.com
Abstract
Background: Traumatic dural tears associated with thoracolumbar burst fractures are uncommon and are rarely complicated by entrapment of neural elements. Pre-operative diagnosis is challenging, and such injuries are often identified only during surgery. Unrecognized dural tears and entrapped nerve roots may result in further neurological injury during operative manipulation.
Case Report: A 34-year-old male presented with an L3 burst fracture following a fall from height and had an incomplete neurological deficit below the L2 level. Radiological evaluation revealed an unstable lumbar burst fracture with laminar involvement. During posterior decompression and stabilization, a large traumatic dural tear with entrapment of nerve rootlets within the laminar fracture was identified intraoperatively. Careful release of the entrapped neural elements and primary dural repair were performed, followed by posterior instrumentation. The patient showed progressive neurological recovery with no cerebrospinal fluid-related complications.
Conclusion: Traumatic durotomy with nerve root entrapment can occur in high-energy lumbar burst fractures, particularly in the presence of laminar fractures, and may be missed on pre-operative imaging. A high index of suspicion and meticulous intraoperative evaluation are essential to prevent iatrogenic neurological injury and to achieve favorable outcomes.
Keywords: Lumbar burst fracture, traumatic durotomy, nerve root entrapment, laminar fracture, case report.
High-energy thoracolumbar burst fractures are occasionally associated with traumatic dural tears, with reported incidences varying across studies. Such dural injuries may lead to complications, including persistent cerebrospinal fluid (CSF) leakage, pseudomeningocele, meningitis, and neurological deterioration. In rare instances, herniation and entrapment of neural elements such as nerve rootlets may occur through the dural defect into the fracture site, significantly increasing the risk of intraoperative neural injury.
Pre-operative identification of traumatic dural tears remains difficult. Certain radiological features – such as laminar fractures, increased interpedicular distance, reduced canal diameter, and sharply angulated retropulsed fragments – have been described as predictive markers [1,2,3,4]. However, direct visualization of entrapped neural elements on imaging is exceedingly rare, with only isolated case reports available in the literature [5,6]. We report a case of traumatic durotomy with nerve root entrapment in a lumbar burst fracture that was diagnosed intraoperatively and managed successfully.
A 34-year-old male presented to the emergency department with a history of a fall from a height of approximately 12 feet at his workplace, 3 h before presentation. He complained of severe lower back pain and had associated facial injuries. On neurological examination, the patient had weakness of bilateral hip flexion and knee extension, along with decreased sensation below the L2 dermatome bilaterally. Deep tendon reflexes at the knees and ankles were sluggish, and bladder dysfunction was noted. Neurological status was classified as American Spinal Injury Association Grade C.
Computed tomography of the lumbar spine demonstrated an L3 burst fracture (AO Spine type A4) with retropulsion of posterior fragments into the spinal canal and an associated laminar fracture (Fig. 1).

Figure 1: Pre-operative imaging demonstrating an L3 burst fracture. (a) Sagittal computed tomography (CT) scan showing an L3 burst fracture with posterior bony retropulsion into the spinal canal. (b) Axial CT scan demonstrating comminution of the L3 vertebral body with an associated laminar fracture (arrow). (c) Sagittal T2-weighted magnetic resonance imaging showing significant spinal canal compromise with compression of neural elements at the L3 level. (d) Coronal CT scan demonstrating comminution of the L3 vertebral body.
The injury was considered unstable with incomplete neurological deficit, and the thoracolumbar injury Classification and Severity Score was 7. Surgical management was planned in the form of posterior decompression and stabilization.
The patient underwent posterior decompressive laminectomy and pedicle screw fixation from L1 to L5 under general anesthesia. Intraoperatively, a longitudinal dural tear measuring approximately 7 cm was identified at the L3 level, extending into the adjacent lamina, with herniation and entrapment of nerve rootlets within the laminar fracture (Fig. 2).
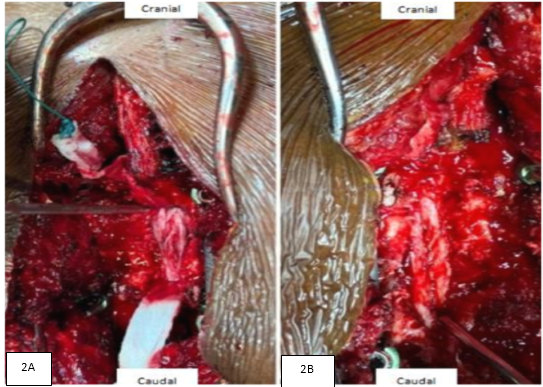
Figure 2: Intraoperative photographs following posterior decompression. (a) After laminectomy, entrapped nerve rootlets were identified and carefully released from the laminar fracture site and reduced into the thecal sac, revealing a longitudinal traumatic dural laceration measuring approximately 4 cm. (b) Primary dural repair performed using interrupted 6-0 Prolene sutures.
Multiple nerve rootlets were found to be herniated and entrapped within the laminar fracture site. A careful extension of decompression with L2 laminectomy was performed to fully expose the dural defect. The entrapped nerve rootlets were gently released, and primary dural repair was carried out using 6-0 Prolene sutures. A dural substitute patch was applied to reinforce the repair, and posterior instrumentation was completed with the addition of a cross-connector at L3.
Post-operative course
Postoperatively, the patient demonstrated gradual improvement in motor and sensory function. Post-operative radiographs confirmed appropriate implant positioning and restoration of spinal alignment (). The surgical drain output remained minimal, with no evidence of CSF leakage. The patient was maintained on strict bed rest with head-low positioning for the first 3 post-operative days, during which in-bed physiotherapy exercises were initiated. Progressive mobilization commenced from post-operative day 4, with assisted ambulation achieved by day 6. The drain was removed on post-operative day 7, and the patient was discharged on post-operative day 10.
At the 2-week follow-up, the patient was ambulatory with walker support, and the surgical wound had healed well. At 6 weeks, he was walking independently without assistive devices and had no signs of CSF-related complications.
Traumatic dural tears are a recognized but underdiagnosed entity in high-energy thoracolumbar spine injuries [3,7,8]. The presence of laminar fractures has been strongly associated with an increased risk of dural disruption, as fracture lines may propagate through the posterior elements and compromise the dura [2,3,4,9]. Entrapment of neural elements through a traumatic dural defect is a rare phenomenon and is usually identified only during surgical exploration.
Dural tears may lead to complications such as pseudomeningocele formation, meningitis, and CSF leakage if unrecognized or inadequately treated [10]. Several studies have attempted to identify imaging predictors of traumatic dural tears, including widened interpedicular distance, reduced canal ratio, and acutely angled retropulsed fragments [1,2]. Despite these indicators, pre-operative detection of neural element entrapment remains uncommon. Failure to recognize this pathology may result in inadvertent nerve injury during reduction or decompression maneuvers.
Cases of transdural nerve root entrapment, although rare, have been described in the literature and highlight the complexity of such injuries [11]. In the present case, although radiological features suggested a high-risk fracture pattern, the dural tear and nerve root entrapment were diagnosed intraoperatively. Prompt recognition, careful neural release, and watertight dural repair resulted in favorable neurological recovery without CSF-related complications, consistent with previously reported outcomes [7,12,13].
Traumatic durotomy with entrapment of nerve roots is a rare but significant complication of high-energy lumbar burst fractures, particularly when associated with laminar fractures. As pre-operative imaging may not reliably detect this condition. Awareness of risk factors and careful intraoperative evaluation are crucial. Early identification and appropriate surgical management can lead to satisfactory neurological outcomes and prevent secondary complications.
High-energy lumbar burst fractures with laminar involvement should alert surgeons to the possibility of traumatic dural tears and neural element entrapment. A high degree of intraoperative vigilance and gentle decompression techniques are essential to avoid iatrogenic neurological injury and to ensure optimal patient outcomes.
References
- 1. Lee IS, Kim HJ, Lee JS, Kim SJ, Jeong YJ, Kim DK, et al. Dural tears in spinal burst fractures: Predictable MR imaging findings. AJNR Am J Neuroradiol 2009;30:142-6. [Google Scholar] [PubMed]
- 2. Park JK, Park JW, Cho DC, Sung JK. Predictable factors for dural tears in lumbar burst fractures with vertical laminar fractures. J Korean Neurosurg Soc 2011;50:11-6. [Google Scholar] [PubMed]
- 3. Xu JX, Zhou CW, Wang CG, Tang Q, Li JW, Zhang LL, et al. Risk factors for dural tears in thoracic and lumbar burst fractures associated with vertical laminar fractures. Spine (Phila Pa 1976) 2018;43:774-9. [Google Scholar] [PubMed]
- 4. Shi X, Xiang S, Dai B, He Z. Association of the presence and its types of lamina fractures with posterior dural tear and neurological deficits in traumatic thoracic and lumbar burst fractures. BMC Musculoskelet Disord 2021;22:300. [Google Scholar] [PubMed]
- 5. Jarin IJ, Samocha Y, Houten JK, Kinon MD. Traumatic durotomy and entrapment of neural elements in a lumbar burst and laminar fracture diagnosed on preoperative imaging: Illustrative case. J Neurosurg Case Lessons 2024;8:CASE24455. [Google Scholar] [PubMed]
- 6. Shankar D, Kaif M, Kumar K. Post-traumatic lumbar nerve root entrapment into the spinous process of the lumbar spine. BMJ Case Rep 2024;17:e257802. [Google Scholar] [PubMed]
- 7. Luszczyk MJ, Blaisdell GY, Wiater BP, Bellabarba C, Chapman JR, Agel JA, et al. Traumatic dural tears: What do we know and are they a problem? Spine J 2014;14:49-56. [Google Scholar] [PubMed]
- 8. Mohamad NH, Salim AA, Yusof MI, Khoh PS, Lim HS, Bahrin Z, et al. Prevalence, implications, and risk factors of traumatic dural tears in thoracic and lumbar fractures: A retrospective study. Cureus 2024;16:e64351. [Google Scholar] [PubMed]
- 9. Milton R, Kalanjiyam GP, Shetty AP, Kanna RM. Dural injury following elective spine surgery: A prospective analysis of risk factors, management and complications. J Clin Orthop Trauma 2023;41:102172. [Google Scholar] [PubMed]
- 10. Nairus JG, Richman JD, Douglas RA. Retroperitoneal pseudomeningocele complicated by meningitis following a lumbar burst fracture: A case report. Spine (Phila Pa 1976) 1996;21:1090-3. [Google Scholar] [PubMed]
- 11. Choi JH, Kim JS, Jang JS, Lee DY. Transdural nerve rootlet entrapment in the intervertebral disc space through minimal dural tear: Report of 4 cases. J Korean Neurosurg Soc 2013;53:52-6. [Google Scholar] [PubMed]
- 12. Kareem H, Raza MH, Kontojannis V, Nimer A, Tsang K. Case series of posterior instrumentation for repair of burst lumbar vertebral body fractures with entrapped neural elements. J Spine Surg 2018;4:374-82. [Google Scholar] [PubMed]
- 13. Abolfotouh SM, Alnori O, Buser Z, Hsieh PC, Abolfotouh MA. Management of dural tears in spine surgery: A worldwide survey of current practices and complications. Global Spine J 2026;16:679-89. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report
June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report