
Peroneus longus tendon autograft provides a larger and more predictable graft diameter with comparable knee stability and lower donor-site morbidity than hamstring tendon, making it a reliable alternative for primary ACL reconstruction
Dr. Mrudul Kyada, Department of Orthopedics, GMERS Medical College, Vadnagar, Gujarat, India. E-mail: mrudulkyada@ymail.com
Abstract
Background: Anterior cruciate ligament (ACL) injury remains one of the most common causes of functional knee instability among young and active individuals. Autografts, especially hamstring tendon (HT) grafts, have long been considered the standard of care; however, concerns regarding variable graft diameter, harvest-related muscle weakness, and donor-site morbidity have led to interest in alternative grafts. The peroneus longus tendon (PLT) has gained attention due to its adequate length, favorable biomechanical strength, and minimal functional deficit at the donor site. This randomized controlled trial compared the clinical, functional, and stability outcomes of PLT autografts with HT autografts in primary ACL reconstruction.
Methods: A prospective randomized controlled trial was conducted on 50 patients undergoing primary ACL reconstruction. Participants were randomized into two equal groups: Group A received PLT autograft (n = 25), and Group B received HT autograft (n = 25). Baseline characteristics, intraoperative parameters, post-operative pain, knee stability, donor-site morbidity, and functional outcomes were assessed using International Knee Documentation Committee (IKDC), Lysholm, and Tegner scores at 3 and 6 months. KT-1000 arthrometer measurements, Lachman and pivot-shift tests were used for objective stability assessment. Data were analyzed using the Statistical Package for the Social Sciences, with P < 0.05 considered statistically significant.
Results: Baseline demographic variables were comparable between groups. PLT grafts demonstrated significantly larger mean graft diameter (8.9 ± 0.6 mm) compared to HT grafts (8.1 ± 0.7 mm; P = 0.001). Operative time was significantly shorter in the PLT group (78.6 ± 11.3 min vs. 86.2 ± 12.7 min; P = 0.02). Early post-operative pain scores were lower in the PLT group (P < 0.05). At 6 months, the PLT group showed significantly higher IKDC (82.6 ± 6.3 vs. 78.9 ± 7.4; P = 0.04) and Lysholm scores (89.4 ± 5.8 vs. 85.1 ± 6.4; P = 0.03). Knee stability outcomes, including Lachman grade, pivot shift, and KT-1000 measurements, were comparable across groups. Donor-site morbidity was significantly lower in the PLT group, with minimal ankle strength deficit compared to notable hamstring weakness in the HT group. Complication rates were low and similar across both groups.
Conclusion: PLT autograft demonstrated larger graft diameter, reduced post-operative pain, better early functional outcomes, and lower donor-site morbidity compared with the traditional hamstring autograft while maintaining equivalent knee stability. PLT appears to be a reliable and effective graft option for primary ACL reconstruction, especially in individuals where preservation of hamstring strength is desirable.
Keywords: Anterior cruciate ligament reconstruction, autograft comparison, knee stability, hamstring tendon, peroneus longus tendon.
Anterior cruciate ligament (ACL) injury remains one of the most prevalent and debilitating knee injuries encountered in orthopedic and sports medicine, accounting for nearly half of all ligamentous knee injuries and affecting predominantly young, active individuals engaged in pivoting sports, such as football, basketball, and handball [1]. An untreated ACL tear leads to recurrent instability, impaired functional performance, and a significantly higher risk of meniscal damage and early-onset osteoarthritis, thus making surgical reconstruction the preferred treatment in symptomatic or high-demand patients [2]. Over the past decades, graft selection for primary ACL reconstruction has continued to evolve, with autografts – particularly hamstring tendon (HT) and bone–patellar tendon–bone (BPTB) grafts – remaining the gold standard due to their biological incorporation, lower risk of disease transmission, and superior long-term outcomes compared to allografts [3]. However, HT autografts, though widely used, have certain limitations, including variable graft diameter, donor site morbidity, residual hamstring weakness, and potential for inadequate rotational stability in high-demand athletes [4]. These limitations have prompted interest in alternative autograft sources, such as the peroneus longus tendon (PLT), which has emerged as a promising substitute because of its sufficient length, consistent diameter, biomechanical strength, and minimal functional deficits at the donor site [5].
Biomechanically, the PLT exhibits tensile strength comparable to the native ACL and hamstring grafts, with several cadaveric and in vivo studies demonstrating that its ultimate load to failure exceeds 4000 N – similar to or greater than quadrupled semitendinosus–gracilis grafts [6]. In addition, harvesting the PLT results in minimal morbidity because the peroneus longus muscle has functional redundancy with the peroneus brevis, allowing preservation of ankle eversion and stability even after tendon harvesting [7]. Early clinical studies have shown encouraging results, with patients undergoing ACL reconstruction using PLT grafts demonstrating comparable Lachman, pivot-shift, and KT-1000 measurements, along with similar functional outcomes based on International Knee Documentation Committee (IKDC), Lysholm, and Tegner scores, when compared with HT grafts [8]. Furthermore, PLT grafts are associated with fewer complaints of donor-site pain, reduced post-operative weakness, and faster early rehabilitation, which may offer functional advantages in active populations [9]. Despite these promising findings, evidence remains limited by small sample sizes, heterogeneity in surgical techniques, and the absence of long-term outcomes, creating a need for adequately powered randomized controlled trials to compare the effectiveness and safety of PLT versus HT grafts.
On the other hand, HT autografts continue to be widely favored due to their minimally invasive harvest technique, reduced anterior knee pain, low donor morbidity, and acceptable long-term graft survival [10]. Yet concerns persist regarding graft diameter variability – particularly in individuals with smaller body habitus – where grafts <8 mm show higher rates of graft failure and revision surgery [11]. In addition, harvesting both semitendinosus and gracilis tendons can compromise dynamic knee stability by reducing flexor strength, particularly at deep knee flexion angles, potentially affecting athletes involved in sprinting or martial arts [12]. Comparative studies between PLT and HT autografts have shown that while both grafts provide satisfactory stability and functional outcomes, PLT offers more predictable graft size, lower donor-site morbidity, and potentially superior graft biomechanics [13]. However, questions remain regarding long-term ankle biomechanics following PLT harvest, including subtle deficits in plantarflexion strength or gait alterations, warranting robust comparative evidence [14]. Therefore, a randomized controlled trial evaluating these two autograft options is essential to establish definitive evidence on graft performance, post-operative stability, functional recovery, donor-site morbidity, and long-term patient satisfaction. The present study aims to fill this knowledge gap by providing a systematic comparison of PLT and HT autografts in primary ACL reconstruction, offering high-quality clinical data that can guide surgeons in selecting the most effective and functional graft for individual patient needs.
Study design
The present study was designed as a prospective, randomized controlled trial that evaluated and compared the clinical, functional, and radiological outcomes of PLT autografts and HT autografts used for primary ACL reconstruction. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Study setting
The study was conducted in the Department of Orthopaedics at a tertiary care teaching hospital equipped with arthroscopy facilities and post-operative rehabilitation services.
Study duration
The total study duration spanned 18 months. This duration included 3 months for preparatory activities, such as protocol development, obtaining ethical approval, staff training, and pilot-testing of data collection tools.
Participants
Inclusion criteria
- Patients aged 18–50 years
- Individuals diagnosed with primary ACL tear confirmed by magnetic resonance imaging (MRI)
- Patients presenting with symptomatic knee instability demanding surgical reconstruction
- Those willing to undergo either graft option if randomized
- Patients able to follow the post-operative physiotherapy protocol
- Patients who provided written informed consent.
Exclusion criteria
- Revision ACL reconstruction cases
- Multiligamentous knee injuries requiring additional grafts
- Associated fractures around the knee
- Severe osteoarthritis (Kellgren–Lawrence grade ≥3)
- Chronic neuromuscular disorders affecting lower limb biomechanics
- Patients with systemic infection, uncontrolled diabetes, or vascular insufficiency
- Patients unwilling to participate or comply with follow-up visits.
Study sampling
A purposive sampling technique was applied initially to screen all ACL injury cases presenting to the outpatient and emergency departments. Eligible participants who fulfilled the inclusion criteria were subsequently enrolled into the study. Random sampling was performed only after recruitment through a computer-generated randomization list to distribute patients equally between the PLT and HT groups. The sampling strategy ensured that every eligible participant had an equal chance of allocation into either group once enrolled.
Study sample size
A total sample size of 50 participants was finalized for the study. Twenty-five participants were assigned to the PLT autograft group, and the remaining twenty-five were allocated to the HT autograft group. The sample size was determined based on expected differences in functional scores between the two grafts, using pilot data from similar published studies. A confidence level of 95%, a power of 80%, and an anticipated dropout rate of 10% were considered during estimation.
Study groups
- Group A – PLT Autograft (n = 25): Participants underwent arthroscopic ACL reconstruction using ipsilateral PLT as the graft source
- Group B – HT Autograft (n = 25): Participants underwent ACL reconstruction using a quadrupled semitendinosus–gracilis tendon autograft.
Both groups followed an identical post-operative rehabilitation protocol.
Study parameters
The study evaluated multiple parameters, including demographic variables, graft diameter, operative time, intraoperative complications, post-operative knee stability (Lachman test, pivot shift test, and KT-1000 arthrometer values), thigh circumference, ankle evertor strength for the PLT group, range of motion, donor-site morbidity, and functional outcomes assessed using IKDC score, Lysholm score, and Tegner activity scale.
Study procedure
All participants underwent standard arthroscopic ACL reconstruction performed by the same surgical team. Under spinal or general anesthesia, diagnostic arthroscopy was first performed. For Group A, the PLT was harvested through a small incision above the lateral malleolus. For Group B, the semitendinosus and gracilis tendons were harvested from the medial aspect of the knee. Grafts were prepared, measured, and passed through anatomically drilled femoral and tibial tunnels using the transportal technique. Fixation was achieved using interference screws or suspensory devices as per standard protocol. Post-operatively, both groups received analgesia, cryotherapy, and commenced a supervised rehabilitation program focusing on early mobilization and strengthening.
Study data collection
Data were collected at baseline (pre-operative), the immediate post-operative period, and follow-up visits at 6 weeks, 3 months, and 6 months. Clinical examinations, stability tests, and functional scores were recorded using validated scoring systems. Data were captured in structured pro formas and later transferred to digital spreadsheets for analysis. A blinded evaluator assessed post-operative functional and stability outcomes to reduce observer bias.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences software. Continuous variables were summarized as mean ± standard deviation and compared using independent t-tests or Mann–Whitney U tests based on distribution. Categorical variables were compared using the chi-square or Fisher’s exact test. A P < 0.05 was considered statistically significant. Intention-to-treat analysis was applied to minimize the impact of dropouts.
Ethical considerations
The study adhered to the ethical guidelines of the Declaration of Helsinki. Approval was obtained from the Institutional Ethics Committee before commencement. Written informed consent was obtained from all participants after explaining the nature, purpose, and possible risks of the study. Confidentiality of patient data was strictly maintained, and participants retained the right to withdraw from the study at any point without affecting their treatment.
Both groups were comparable at baseline with no statistically significant differences in age, sex distribution, side of injury, or injury-to-surgery interval (P > 0.05). This indicates successful randomization (Table 1).
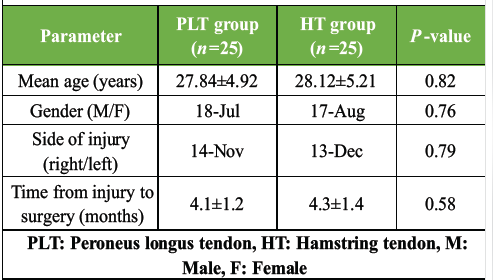
Table 1: Demographic characteristics of study participants
PLT grafts had a significantly larger diameter than HT grafts (P = 0.001). PLT harvest also resulted in shorter operative time. Complication rates were low and comparable (Table 2).
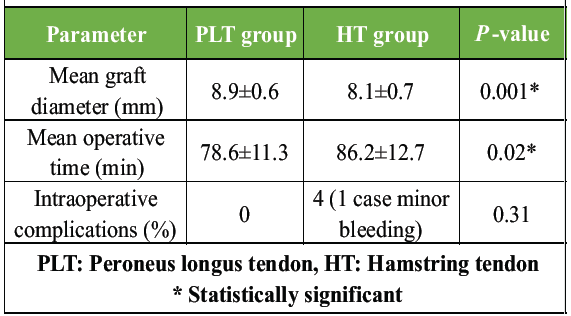
Table 2: Intraoperative findings
The PLT group had significantly lower early post-operative pain (day 1 and week 1). By week 6, pain levels were comparable (Table 3 and Fig. 1).
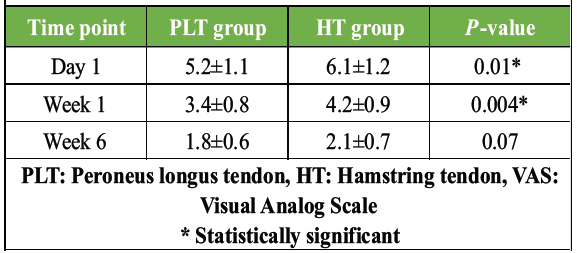
Table 3: Post-operative pain score (VAS)
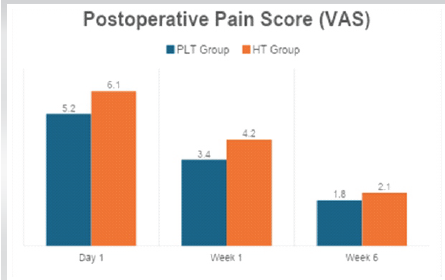
Figure 1: Post-operative pain score (Visual Analog Scale).
Both groups demonstrated equally good post-operative stability, with no statistically significant differences in Lachman, pivot shift, or KT-1000 measurements (Table 4).
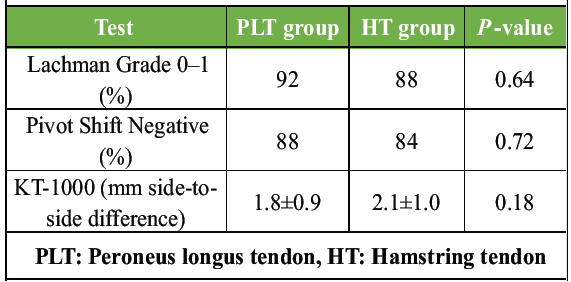
Table 4: Knee stability assessment
Functional outcomes at 3 months were similar in both groups without statistical significance (Table 5 and Fig. 2).
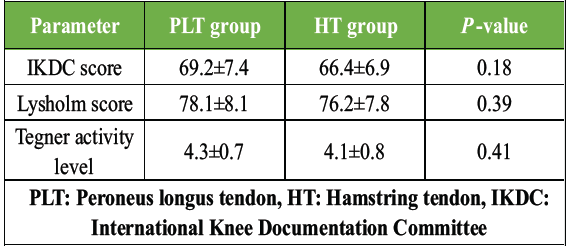
Table 5: Functional scores at 3 months
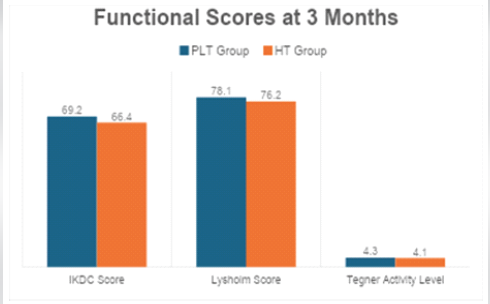
Figure 2: Functional scores at 3 months.
At 6 months, the PLT group showed significantly better functional outcomes in IKDC and Lysholm scores – suggesting faster recovery and better early knee function (Table 6 and Fig. 3).
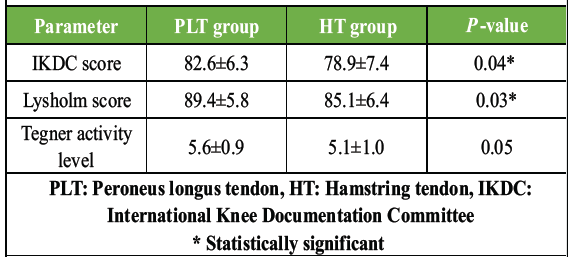
Table 6: Functional scores at 6 months
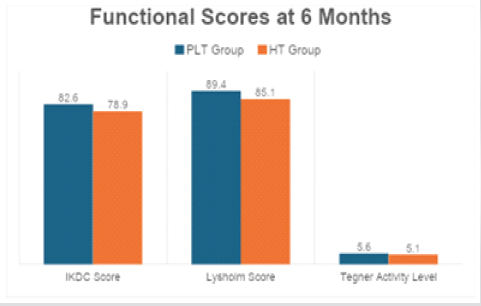
Figure 3: Functional scores at 6 months.
Both groups regained full functional range of motion with no significant differences (P > 0.05) (Table 7 and Fig. 4).
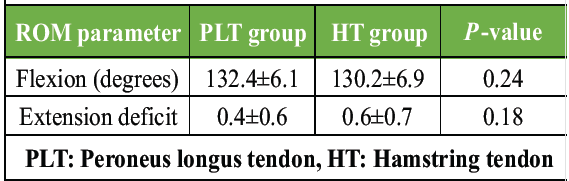
Table 7: Range of motion (ROM) at 6 months
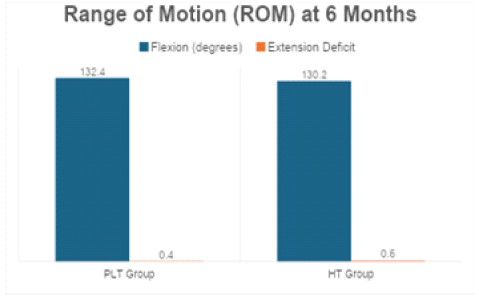
Figure 4: Range of motion at 6 months.
The PLT group showed minimal ankle strength reduction, whereas the HT group showed significant hamstring weakness. Donor-site pain was significantly lower in the PLT group (Table 8).
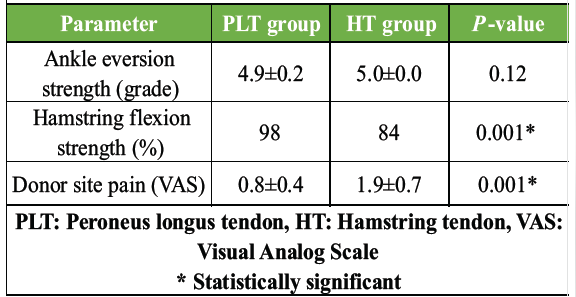
Table 8: Donor site morbidity
Complications were rare and similar across both groups. One graft failure occurred in the HT group (Table 9 and Fig. 5).
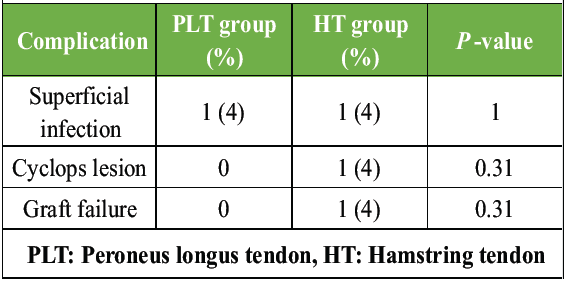
Table 9: Complication rates
Figure 5: Complication rates.
Although not statistically significant, a greater proportion of PLT patients returned to pre-injury activity, and they did so slightly earlier than HT patients (Table 10).
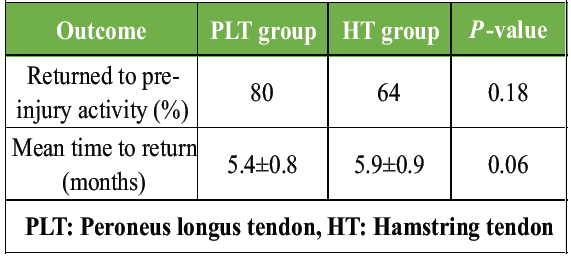
Table 10: Return to activity/sports
The present randomized controlled trial compared PLT and HT autografts in primary ACL reconstruction and found that PLT grafts provided larger graft diameters, slightly shorter operative times, comparable knee stability, better early functional scores at 6 months, and lower donor-site morbidity, particularly with respect to hamstring strength and donor-site pain. These findings are largely consistent with, and in some aspects slightly more favorable than, a growing body of comparative literature evaluating PLT as an alternative to HT in ACL reconstruction.
Our observation that PLT grafts had significantly larger diameters than HT grafts parallels the comparative series by Gök et al., who reported mean PLT graft diameters of 8.56 ± 0.93 mm versus 7.44 ± 0.60 mm for hamstring grafts in 106 patients, with PLT also associated with shorter harvest times and less donor-site morbidity [11]. Similarly, Punnoose et al. demonstrated that PLT autografts yielded better graft diameter, less morbidity, and enhanced muscle recuperation compared with HT grafts, reinforcing the concept that PLT is an “advantageous” graft in terms of intraoperative characteristics and early recovery [12]. These clinical observations are biomechanically plausible, given that cadaveric work comparing tendon tensile strength has shown the PLT to have strength comparable to – or not inferior to – HTs, supporting its suitability as a primary ACL graft [13]. Our finding of a shorter overall operative time in the PLT group also aligns with randomized and comparative studies in which PLT harvesting was reported to be technically straightforward, with reduced harvest time compared to multi-strand hamstring graft preparation.
Knee stability outcomes in our trial, assessed by Lachman, pivot-shift, and KT-1000 measurements, were comparable between PLT and HT groups, with high rates of grade 0–1 Lachman and negative pivot-shift in both arms. This is in agreement with multiple comparative cohorts and randomized trials that have reported equivalent anteroposterior and rotational stability between PLT and HT autografts at short- to mid-term follow-up. Keyhani et al. [14] found no significant differences in Lachman or pivot-shift tests and similar failure rates at a mean 2-year follow-up between PLT and HT reconstructions. Rhatomy et al., [15] in a single-bundle ACL reconstruction study, even suggested that PLT may be “superior” to HT based on comparable stability with potential advantages in donor-site morbidity. A broader meta-analysis by Park et al. [16] pooling six randomized controlled trials (683 patients) concluded that PLT is a non-inferior alternative to HT, with no significant differences in Lysholm or IKDC scores at 12–24 months and comparable graft diameters and stability, while demonstrating fewer donor-site complications in the PLT group. Our stability data therefore reinforce the emerging consensus that PLT does not compromise mechanical knee stability when used as an ACL graft.
In terms of functional outcomes, our study showed that both groups improved substantially over time, but the PLT group had significantly higher IKDC and Lysholm scores at 6 months, suggesting faster early functional recovery. This pattern is compatible with several recent comparative studies that reported either similar or slightly better early patient-reported outcomes with PLT. Gök et al. [11] observed similar IKDC and Lysholm scores between PLT and HT at final follow-up but noted faster rehabilitation and reduced thigh hypotrophy in the PLT arm, which may translate into earlier subjective improvement. Saeed et al., [17] in a JBJS Open Access study, found that doubled PLT autografts allowed an earlier return to sports and less donor-site morbidity compared with quadrupled hamstring grafts, although long-term clinical scores converged by 2 years. Similarly, Phatama et al. [18] reported in a randomized comparative study that PLT grafts had longer graft length, shorter surgery time, and fewer donor-site complications, with functional scores similar or slightly better than HT at early follow-up. The meta-analysis by Park et al. [16] also noted that although pre-operative and early post-operative scores sometimes favored HT, there were no significant differences by 12–24 months, implying that both grafts ultimately provide comparable long-term function. Our finding of superior 6-month scores in the PLT arm fits within this pattern of PLT supporting at least equivalent, if not faster, early functional recovery without compromising long-term expectations.
A key strength of PLT in our study was the favorable donor-site morbidity profile. We found significantly less hamstring weakness and lower donor-site pain in the PLT group compared with the HT group, with only a minimal reduction in ankle eversion strength that remained near-normal grades on clinical testing. This aligns closely with the narrative emerging from both single-arm PLT series and comparative studies. Nair et al., [19] in a 120-patient prospective series, reported marked improvements in IKDC and Lysholm scores with PLT grafts and excellent donor ankle function, with mean American Orthopaedic Foot and Ankle Society (AOFAS) and Foot and Ankle Disability Index scores above 98 at 1 year and no meaningful loss of ankle stability. The dedicated ankle-focused study by Singh et al. [20] in the Journal of Orthopaedic Case Reports showed that, although a high proportion of patients reported mild early donor-site pain and swelling, AOFAS and Visual Analog Scale-foot and ankle scores improved significantly over time, and ankle function at 6 months remained good, suggesting that PLT harvesting leads to minimal and largely transient ankle morbidity. Our findings of preserved ankle function with PLT, combined with reduced hamstring weakness compared to HT, parallel these results and support the concept that peroneus brevis and appropriate tenodesis can compensate effectively for the harvested PLT, preserving eversion strength and gait.
By contrast, the HT group in our trial demonstrated greater hamstring strength deficit and higher donor-site pain scores, an observation that is consistent with broader ACL literature describing donor-site muscle weakness and discomfort after hamstring harvest. Meta-analyses and long-term follow-up studies of HT autografts have highlighted issues, such as flexor strength deficits, thigh hypotrophy, and altered muscle balance, even when overall knee function and stability remain acceptable. For instance, Gök et al. [11] documented significantly greater thigh hypotrophy and donor-site symptoms in the HT group compared with PLT, and Punnoose et al. emphasized enhanced muscle recuperation with PLT relative to HT [12]. These data help contextualize our findings: While HT remains an established and successful graft with excellent long-term results; PLT may offer a more favorable donor-site profile, especially in patients where preservation of hamstring strength is desirable.
Our low complication rates and absence of graft failure in the PLT group are also reassuring and in keeping with previous series. Singh et al. similarly concluded that PLT harvesting is safe, with most ankle symptoms mild and improving over time [20]. In the wider graft choice literature, systematic reviews comparing BPTB and HT autografts have shown comparable failure rates but differing donor-site problems (anterior knee pain vs. flexor weakness). Our results suggest that PLT fits into this landscape as a third option that maintains low failure rates while potentially reducing both anterior knee and hamstring-specific morbidity.
Taken together, our trial adds to the growing body of evidence that PLT is a reliable alternative to HT for primary ACL reconstruction. The combination of larger graft diameter, efficient harvesting, comparable or superior early functional outcomes, and a favorable donor-site morbidity profile is in line with recent comparative studies, randomized trials, and meta-analyses supporting PLT as a viable, and in some contexts, preferable, graft option. Nonetheless, our follow-up was limited to 6 months, whereas several key studies have reported outcomes at 1–3 years or longer. Longer-term follow-up in our cohort is needed to confirm the durability of functional gains, monitor graft failure rates, and exclude late-onset ankle or knee degenerative changes. Future multicenter randomized trials with larger sample sizes and standardized outcome measures, integrated with biomechanical and patient-reported data, would further clarify the optimal indications for PLT versus HT, particularly in high-demand athletic populations and revision settings.
This study has several limitations that should be acknowledged. The relatively small sample size (n = 50) may limit statistical power and the ability to detect smaller yet clinically meaningful differences between grafts. Being a single-center study conducted at a tertiary care institution, the findings may not be fully generalizable to other settings with different patient demographics or surgical practices. The follow-up period of 6 months is insufficient to assess long-term graft survival, late failures, degenerative changes, or sustained return-to-sport outcomes. Parameters, such as re-injury rates, long-term activity levels, and competitive sports participation were not evaluated. Objective ankle biomechanics, isokinetic muscle strength testing, and gait analysis were not performed, which may underestimate subtle donor-site deficits after PLT harvest. Imaging-based assessment of graft maturation, tunnel integration, and ligamentization using MRI or second-look arthroscopy was not undertaken. Although pivot-shift testing was performed, more sensitive quantitative rotational stability tools were not utilized. All surgeries were performed by a single surgical team without surgeon blinding, which improves procedural consistency but may introduce performance bias and limit external validity. The restricted age group (18–50 years) and exclusion of multiligament injuries, revision ACL reconstructions, severe osteoarthritis, and other complex cases limit applicability to broader patient populations. BPTB grafts were not included for comparison. Economic evaluation was not performed, and donor-site morbidity assessment relied primarily on clinical evaluation without comprehensive patient-reported outcome measures. Rehabilitation compliance could not be fully controlled, and subgroup analyses based on activity level were not conducted. Early functional advantages observed with the PLT graft may not necessarily translate into long-term superiority, and subtle learning-curve effects related to the harvest technique cannot be entirely excluded. Multicenter randomized trials with larger and more diverse populations are warranted to validate these findings.
In this randomized controlled trial comparing PLT and HT autografts for primary ACL reconstruction, the PLT graft demonstrated several clinical advantages, including a consistently larger graft diameter, shorter operative time, reduced early post-operative pain, and significantly lower donor-site morbidity, particularly with preservation of hamstring strength. Functional outcomes at 6 months – reflected by higher IKDC and Lysholm scores – indicated faster early recovery in the PLT group, while both grafts provided comparable knee stability on clinical and instrumented assessment. Complication rates were minimal and similar in both groups. Overall, the findings support PLT autograft as a safe, effective, and biomechanically reliable alternative to the traditional hamstring graft, making it a valuable option for ACL reconstruction, especially in patients requiring preservation of hamstring function or in cases where HTs are inadequate in size.
PLT autograft is a safe and effective alternative to HT for primary ACL reconstruction, offering predictable graft size, comparable knee stability, and reduced donor-site morbidity, making it particularly useful in young and active patients.
References
- 1. Acharya K, Mody A, Madi S. Functional outcomes of anatomic single bundle primary ACL reconstruction with peroneus longus tendon (without a peroneal tenodesis) versus hamstring autografts. Arch Bone Jt Surg 2024;12:116-22. [Google Scholar] [PubMed]
- 2. Acevedo RJ, Rivera-Vega A, Miranda G, Micheo W. Anterior cruciate ligament injury: Identification of risk factors and prevention strategies. Curr Sports Med Rep 2014;13:186-91. [Google Scholar] [PubMed]
- 3. Agarwal A, Singh S, Singh A, Tewari P. Comparison of functional outcomes of an anterior cruciate ligament (ACL) reconstruction using a peroneus longus graft as an alternative to the hamstring tendon graft. Cureus 2023;15:e37273. [Google Scholar] [PubMed]
- 4. Agel J, LaPrade RF. Assessment of differences between the modified Cincinnati and international knee documentation committee patient outcome scores: A prospective study. Am J Sports Med 2009;37:2151-57. [Google Scholar] [PubMed]
- 5. Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lázaro-Haro C, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc 2009;17:705-29. [Google Scholar] [PubMed]
- 6. Arastu MH, Grange S, Twyman R. Prevalence and consequences of delayed diagnosis of anterior cruciate ligament ruptures. Knee Surg Sports Traumatol Arthrosc 2015;23:1201-5. [Google Scholar] [PubMed]
- 7. Bae JM. A suggestion for quality assessment in systematic reviews of observational studies in nutritional epidemiology. Epidemiol Health 2016;38:e2016014. [Google Scholar] [PubMed]
- 8. Bi M, Zhao C, Zhang S, Yao B, Hong Z, Bi Q. All-inside single-bundle reconstruction of the anterior cruciate ligament with the anterior half of the peroneus longus tendon compared to the semitendinosus tendon: A two-year follow-up study. J Knee Surg 2018;31:1022-30. [Google Scholar] [PubMed]
- 9. Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med 2009;37:890-7. [Google Scholar] [PubMed]
- 10. Buoncristiani AM, Tjoumakaris FP, Starman JS, Ferretti M, Fu FH. Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy 2006;22:1000-6. [Google Scholar] [PubMed]
- 11. Gök B, Kanar M, Tutak Y. Peroneus longus vs hamstring tendon autografts in ACL reconstruction: A comparative study of 106 patients’ outcomes. Med Sci Monit 2024;30:e945626. [Google Scholar] [PubMed]
- 12. Punnoose DJ, Varghese J, Theruvil B, Thomas AB. Peroneus longus tendon autografts have better graft diameter, less morbidity, and enhanced muscle recuperation than hamstring tendon in ACL reconstruction. Indian J Orthop 2024;58:979-86. [Google Scholar] [PubMed]
- 13. Opoku M, Abdramane AM, Ibrahim AA, Xiao W. Can peroneus longus tendon autograft become an alternative to hamstring tendon autograft for anterior cruciate ligament reconstruction: A systematic review and meta-analysis of comparative studies. J Orthop Surg Res. 2025;20:719. [Google Scholar] [PubMed]
- 14. Keyhani S, Qoreishi M, Mousavi M, Ronaghi H, Soleymanha M. Peroneus longus tendon autograft versus hamstring tendon autograft in anterior cruciate ligament reconstruction: A comparative study with a mean follow-up of two years. Arch Bone Jt Surg 2022;10:695-701. [Google Scholar] [PubMed]
- 15. Rhatomy S, Asikin AI, Wardani AE, Rukmoyo T, Lumban-Gaol I, Budhiparama NC. Peroneus longus autograft can be recommended as a superior graft to hamstring tendon in single-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2019;27:3552-9. [Google Scholar] [PubMed]
- 16. Park JY, Fernandes A, Park SY, Lim H, Sayudo IF, Leibovitch L, et al. Comparative effectiveness of peroneus longus tendon autografts versus hamstring tendon autografts in anterior cruciate ligament reconstruction: A comprehensive systematic review and meta-analysis. Eur J Orthop Surg Traumatol 2024;34:2691-9. [Google Scholar] [PubMed]
- 17. Saeed UB, Ramzan A, Anwar M, Tariq H, Tariq H, Yasin A, et al. Earlier return to sports, reduced donor-site morbidity with doubled peroneus longus versus quadrupled hamstring tendon autograft in ACL reconstruction. JB JS Open Access 2023;8:e23.00051. [Google Scholar] [PubMed]
- 18. Phatama KY, Hidayat M, Mustamsir E, Pradana AS, Dhananjaya B, Muhammad SI, et al. Tensile strength comparison between hamstring tendon, patellar tendon, quadriceps tendon and peroneus longus tendon: A cadaver research. J Arthrosc Joint Surg 2019;6:114-16. [Google Scholar] [PubMed]
- 19. Nair NM, Krishnan J, Roy AS, Francis CJ, Shibu R. Arthroscopic primary anterior cruciate ligament reconstruction using peroneus longus autograft: Functional and clinical outcome. J Med Sci Res 2024; 12(2):108-112 [Google Scholar] [PubMed]
- 20. Singh MP, Verma M, Agrawal DR, Gaur TN, Maravi DS, Dhanopeya A. Evaluation of ankle complications after peroneus longus tendon harvesting for ACL reconstruction. J Orthop Case Rep 2025;15:207-12. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Randomized Controlled Study Comparing Hamstring Graft and Peroneus Longus Tendon Graft in Arthroscopic ACL Reconstruction
November 1, 2024 Randomized Controlled Study Comparing Hamstring Graft and Peroneus Longus Tendon Graft in Arthroscopic ACL Reconstruction July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction
June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction