
Reconstruction with autografts provides superior strength and biological integration in chronic patellar tendon ruptures or failed primary repairs, with hamstring grafts commonly used and peroneus longus serving as a reliable alternative, particularly in revision cases for restoring patellar height and knee biomechanics.
Dr. T T Unais, Department of Trauma and Emergency (Orthopaedics), All India Institute of Medical Sciences, Bhubaneswar - 751019, Odisha, India. E-mail: unaisstt@gmail.com
Abstract
Introduction: Although uncommon, chronic patellar tendon rupture and failure of primary repair can be challenging to treat and compromise the knee extensor mechanism. When tendon quality is poor and there is quadriceps contracture or fibrosis, repair may be limited, making patellar tendon reconstruction the preferred treatment approach. However, no unified view exists on the optimal graft selection for reconstruction of the patellar tendon.
Case Series: This is a case series of five patients treated in a tertiary care facility between 2022 and 2025 for chronic or failed primary patellar tendon ruptures. In all five patients, reconstruction was performed using the ipsilateral hamstring or peroneal autografts. The harvested tendon was passed in a figure-of-eight fashion through trans-osseous tunnels created on the patella and the tibial tuberosity. The graft was then fixed to the tibia with bioabsorbable screws and suture anchors. Functional outcomes were evaluated at the final follow-up of 6 months, focusing on the range of motion, extensor lag, radiographic patellar height, and complications observed post-surgery.
Results: At final follow-up, four out of five patients gained full active knee extension without any extensor lag, while one patient still had an extension lag of 20°. The range of knee flexion was 100–130°. No cases of re-rupture or fixation failure were observed. There was minimal donor-site morbidity, and no significant ankle instability was noted in patients who underwent peroneus longus tendon harvest.
Conclusion: Patellar tendon reconstruction using autografts provides reliable restoration of knee extensor function in chronic ruptures and failed primary repairs. Both hamstring and peroneus longus tendons are effective graft options, and graft selection should be individualized based on tendon defect size, tissue quality, and intraoperative findings. Accurate restoration of patellar height is critical for optimal functional outcomes.
Keywords: Chronic patellar tendon rupture, failed patellar tendon repair, hamstring autograft, peroneus longus tendon, patellar tendon reconstruction.
A rupture of the patellar tendon is an infrequent condition that significantly impairs knee extension, leading to functional limitations. It typically occurs following eccentric stress or direct trauma, most often seen in younger, physically active patients [1]. Epidemiological studies estimate the incidence of patellar tendon ruptures to range from approximately 0.5–1/100,000 people [2,3]. This will ultimately lead to quadriceps atrophy, a high-riding patella, and an inability to extend the knee actively. In acute rupture, end-to-end repair or augmentation can be tried. But in chronic cases where direct primary repair cannot be performed, reconstructive surgery remains the preferred treatment, with the primary objective of restoring active knee extension [4]. The failure rate of primary repair alone is significant in these situations. Various strategies, such as staged procedures, the use of autograft or allograft tissue, and synthetic grafts have been described for managing subacute and chronic patellar tendon defects [5,6]. Similarly, there is no general agreement on graft choice and the methods of quadriceps lengthening in neglected patellar tendon rupture [7]. Nonetheless, most of the research uses hamstring grafts, quadriceps turndown flaps, free fascia lata grafts, achilles tendon grafts, contralateral bone-patellar tendons, and even artificial tendons, such as ligament advanced reinforcement systems [8]. This case series outlines a method of patellar tendon reconstruction utilizing either an ipsilateral hamstring or peroneus longus autograft, routed through bone tunnels in the patella and tibial tuberosity, and secured to the tibia with a combination of suture anchors and bioabsorbable screws. Outcome measures were evaluated clinically and functionally, along with the complications at 6 months.
Between 2022 and 2025, a total of five patients (four males and one female) with chronic patellar tendon rupture or failed primary repair were treated at All India Institute of Medical Sciences, Bhubaneswar. The mean age was 34.1 years. Four patients had chronic neglected rupture, and the remaining one presented with failed primary repair. All the patients presented with an extensor lag and an inability to actively extend their knees. Their lateral radiographs were suggestive of patella alta. All patients underwent magnetic resonance imaging (MRI) to confirm patellar tendon discontinuity and to evaluate the tendon quality. The Insall-Salvati ratio was calculated preoperatively to assess patellar height [9]. The selection of graft and fixation method was based on intraoperative findings, quality of the tendon and bone, and the availability of tendon.
Patient demographics are given in Table 1.
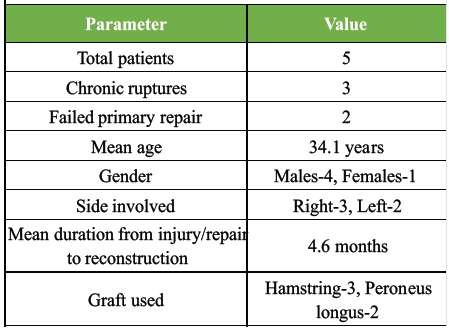
Table 1: Patient demographics
Case 1
A 19-year-old, known diabetic, male presented with a machine-cut injury to the left anterior knee. The patellar tendon was visibly torn with superior migration of the patella (Fig. 1).

Figure 1: Visibly torn patellar tendon with open knee joint.
The patient exhibited loss of active knee extension capability. Radiographs showed an inferior patellar pole avulsion and patella alta. The wound was debrided, and antibiotics were administered. A cylindrical slab was applied after debridement, with a window created over the wound for regular dressing. The patient developed knee stiffness during the course of wound healing. Gradual knee bending was started and attained 90° flexion within two months. MRI was done to confirm the diagnosis (Fig. 2).
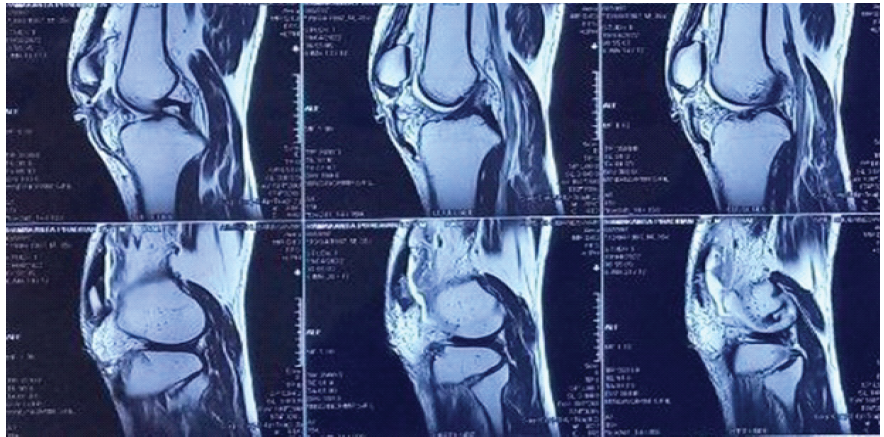
Figure 2: Magnetic resonance imaging showing patellar tendon rupture.
Reconstruction was planned with the hamstring tendon, but during surgery, the tendon was found to be thin. Hence, the ipsilateral peroneus tendon was used for reconstruction. Reattachment of the inferior patellar pole was performed using a suture anchor placed at the superior pole of the patella (Fig. 3).

Figure 3: Postoperative radiograph showing suture anchor on the superior pole of the patella and bioscrew on the proximal tibia.
At six months follow-up, the patient achieved full knee extension with 130° of flexion and no extensor lag.
Case 2
A 27-year-old male patient presented with the inability to extend his right knee. He met with a road traffic accident five months back and sustained bilateral open shaft of femur fracture and open left leg fracture. He was then managed with debridement and external fixation of the bilateral femur and left leg. Definitive fixation was done after 3 weeks, once the patient was stabilized. On presentation after five months, the clinical examination revealed an extensor lag with knee stiffness beyond 70° flexion. Imaging was suggestive of patellar tendon rupture. Physiotherapy was done to improve the knee range of motion (ROM). The patient was taken up for patellar tendon reconstruction once ROM exceeded 90°. The hamstring tendon was used for reconstruction. At final follow-up, the patient had a 20° extension lag (Fig. 4) and 100° flexion with some anterior knee pain.

Figure 4: Postoperative extensor lag.
Case 3
A 37-year-old male, with a history of a fall from a bike six months back, presented with decreased ROM of the right knee, difficulty in standing from a seated position, and painless limping during walking. Initial evaluation at a local hospital revealed no bony abnormality on radiographs, resulting in the patellar tendon rupture being overlooked. On presentation to our hospital, there was a visible gap on inspection and a palpable gap below the patella. ROM was between 45° and 100° with an extension lag of 45°. Radiographs revealed patella alta, and MRI was suggestive of a complete patellar tendon tear with a lateral meniscal tear. A diagnosis of chronic patellar tendon rupture was made. Reconstruction was done using the ipsilateral hamstring tendon autograft. By the final follow-up, the patient demonstrated complete knee extension and achieved 120° of active flexion.
Case 4
A 42-year-old male presented with persistent right knee instability and extension lag, 4 months following primary repair of an acute patellar tendon rupture. He reported difficulty with ambulation and stair climbing. Clinical examination demonstrated quadriceps weakness and inability to achieve full active extension, while passive ROM was nearly 130°. Radiographs revealed patella alta, indicating failure of the initial repair and disruption of the extensor mechanism. In view of poor functional recovery and compromised tendon integrity, revision reconstruction was performed using an ipsilateral peroneus longus tendon autograft. At final follow-up, the patient achieved full active extension and 130° of knee flexion without pain or instability, reflecting successful functional restoration after revision surgery.
Case 5
A 36-year-old female presented with an inability to actively extend the left knee and difficulty in walking for 6 months after undergoing primary repair for traumatic patellar tendon rupture following a road traffic accident. Clinical evaluation demonstrated extensor lag, quadriceps weakness, and proximal migration of the patella consistent with chronic disruption of the extensor mechanism. She underwent reconstruction using an ipsilateral hamstring tendon autograft to restore patellar height and tendon continuity. On postoperative day 5, she developed fever and purulent discharge from the surgical site. Prompt wound exploration, drainage, and thorough debridement were performed, followed by culture-directed intravenous antibiotics. The infection resolved with appropriate management. At final follow-up, the patient achieved full active knee extension and 120° of flexion, with good quadriceps strength and satisfactory functional recovery.
A case-wise summary is listed in Table 2.
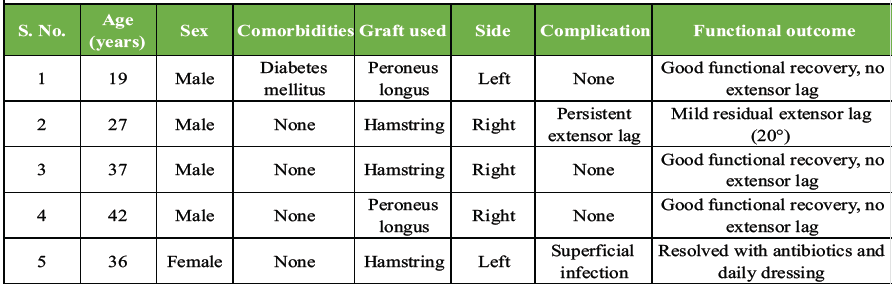
Table 2: Case-wise summary
Each procedure was carried out with the patient under spinal anesthesia in a supine position, and a pneumatic tourniquet was consistently used. Exposure of the patellar tendon was achieved through an anterior midline incision extending from the patellar upper border down to the tibial tuberosity, with medial and lateral flaps raised for adequate visualization.
The patella could be lowered to its anatomical position following meticulous dissection and the release of the parapatellar retinaculum. In hamstring tendon reconstruction, the semitendinosus with or without the gracilis tendon was harvested through a standard pes anserinus incision, or in some cases, the incision for patellar tendon exposure was utilized for hamstring harvest. Whereas, in peroneus longus tendon reconstruction, the graft was obtained through a limited incision positioned just behind the lateral malleolus, while giving attention not to injure the peroneus brevis tendon. The choice between hamstring and peroneus longus was made based on intraoperative findings. Considering the ease of harvest and well-established use, the primary option in every case was a hamstring graft. But in cases where the hamstring tendons were inadequate (Insufficient diameter or poor quality) or if additional length was required, peroneus longus was selected. The harvested hamstring tendon provided a length between 20 and 25 cm when doubled, whereas the peroneus longus tendon yielded a length of approximately 22–28 cm, offering adequate length for patellar tendon reconstruction. The harvested graft was prepared and subsequently directed through a bone tunnel fashioned in the lower pole of the patella. Bone tunnels were created under fluoroscopic guidance using a guidewire followed by drilling with a cannulated drill of appropriate size (typically 4.5–5 mm), ensuring bicortical purchase while preserving cortical integrity. The graft is then taken out through a horizontal tunnel created posterior to the tibial tuberosity in a figure-of-eight fashion (Fig. 5).

Figure 5: Harvested tendon in figure-of-eight fashion.
The patella was pulled down and positioned such that the effective length of the repaired tendon and the patellar height were equivalent. The patellar height was restored under fluoroscopy guidance. A bioabsorbable screw was used to secure the graft under tension in this position to the tibia tunnel (Fig. 6).
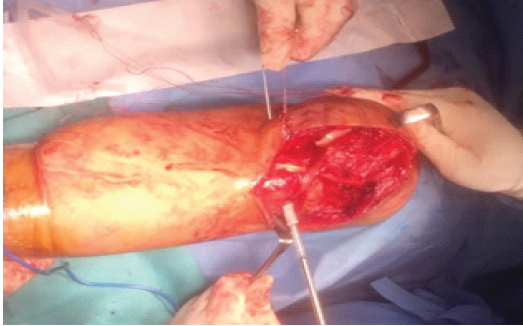
Figure 6: Bio screw insertion.
For additional stability, suture anchors were implanted on the proximal tibia, and the threads were used to augment the reconstructed patellar tendon. Even though the quality of the native patellar tendon in all seven cases was poor, it was sutured onto the reconstructed tendon.
Postoperative protocol:
• Post-operative radiographs were taken in all cases to confirm and document the patella height
• The operated knee was kept immobilized with a hinged brace secured in full extension
• Partial weight bearing was permitted as tolerated, advancing progressively to full weight-bearing status over 6 weeks
• Passive ROM was initiated after 2 weeks, with a target of 90° flexion by 6 weeks
• Ankle pumps, Static quadriceps exercises, and hip abductor strengthening from the 1st post-operative day.
All the patients were followed up regularly at 2 weeks, 6 weeks, 3 months, and 6 months. Radiographs were taken at 6 weeks, 3 months, and 6 months to assess the patella height. At final follow-up, four patients achieved restoration of active knee extension without extension lag, and one patient had an extension lag of 20°. Flexion ranged from 100° to 130°. No re-rupture or fixation failures were observed. Three patients experienced mild donor site pain following hamstring harvesting. It resolved spontaneously before the final follow-up. No ankle instability or functional deficit was noticed in patients who underwent peroneus longus harvest, consistent with previously published studies [10,11]. The mean knee flexion improved from 96° preoperatively to 120° at final evaluation. Preoperative extension lag was present in all patients and resolved in four of the five patients following surgery. Functional scores demonstrated significant improvement. The mean Lysholm score increased from 38 ± 6 to 86 ± 7, and the mean Kujala score improved from 44 ± 8 to 88 ± 6 at final follow-up. Overall, the series showed substantial improvement in knee ROM, extensor mechanism function, and patient-reported outcomes (functional outcome is listed in Table 3).
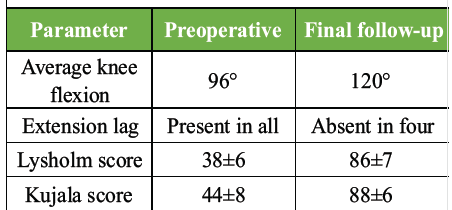
Table 3: Functional outcome
In this series of five patients, complications were minimal. One patient developed a superficial surgical site infection, which was managed successfully with oral antibiotics and local wound care, with no progression to deep infection or need for surgical intervention. Persistent extensor lag was observed in one patient at final follow-up despite rehabilitation; however, this did not significantly compromise overall functional recovery. No cases of re-rupture were noted during the follow-up period (complications are listed in Table 4).
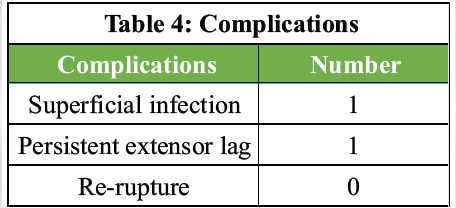
Table 4: Complications
For an orthopedic surgeon, chronic patellar tendon rupture and primary repair failure are challenging clinical situations. Significant proximal migration of the patella, quadriceps muscle shortening, poor tendon quality, fibrosis, and altered patellofemoral biomechanics are characteristics of this disease that, in contrast to acute ruptures, jeopardize the viability and longevity of direct repair. As a result, transplant tissue repair is frequently recommended as the best course of action in these situations.
Challenges related to recurrent rupture and failure of initial tendon repair
Patella alta and extensor mechanism insufficiency result from quadriceps contracture and retraction of the patellar tendon ends when presentation is delayed past 6 weeks [12]. In revision cases, there may be inadequate remaining tendon tissue because the initial repair failed due to weak fixation, premature mobilization, infection, or underlying tendon degeneration [13]. Several reconstructive techniques have been reported, including biological and synthetic materials, such as autografts, artificial ligaments, cerclage wiring, and donor grafts, such as Achilles tendon or bone-patellar tendon-bone constructs. However, every method has its own drawbacks. While synthetic materials are linked to foreign body reactions and long-term failure, allografts offer hazards of disease transfer, delayed integration, and increased expense [14,15].
Role of autografts in patellar tendon reconstruction
Hamstring tendon autografts are among the most used grafts for patellar tendon reconstruction. They are easy to harvest with minimal donor-site morbidity and satisfactory tensile strength [16]. Reports from multiple studies have shown good functional outcomes using hamstring tendons in cases of chronic patellar tendon ruptures [17]. In cases with significant patellar tendon migration or large tendon defects, the use of the hamstring tendon as a reconstruction option is limited by its inadequate length or diameter. This makes it difficult to use hamstring tendons in revision cases [10]. In such cases, alternative autograft options that provide greater length and strength may be advantageous.
Peroneus longus tendon as an autograft option
The peroneus longus tendon has recently gained attention as a viable autograft choice for reconstructing knee ligaments and the extensor mechanism. Tensile strength of the peroneus tendon is comparable to or exceeding that of hamstring tendons [11]. Furthermore, because of its length, which permits flexibility in graft configuration, it is especially well-suited for chronic and revision cases requiring substantial reconstruction. According to clinical research, harvesting the peroneus longus while preserving the peroneus brevis tendon minimizes donor-site complications and does not substantially influence ankle eversion strength and gait pattern [18,19]. In this case series, one patient experienced transient ankle eversion weakness that resolved completely with physiotherapy, consistent with previously reported outcomes [19].
Restoration of patellar height and biomechanics
Restoration of the patellar height is a crucial component of successful patellar tendon reconstruction. Patella alta, if not restored, leads to increased patellofemoral contact forces, extensor lag, quadriceps weakness, and inferior functional outcomes [20]. In this case series, patellar height was restored intraoperatively using fluoroscopic guidance by comparing with the contralateral knee and referencing standard indices (eg., Insall-Salvati ratio). The patella was gradually pulled distally by applying controlled traction on the graft until the appropriate length was achieved, and the graft was fixed under adequate tension in 30° knee flexion. Routine use of fluoroscopy, comparison with the opposite knee, maintaining proper knee flexion during fixation, and confirming the patellar tracking before final graft fixation are the main points to keep in mind. Previous authors have emphasized that accurate restoration of patellar height is as important as graft selection in achieving good outcomes [21].
Outcomes in chronic rupture versus failed primary repair
Both chronic ruptures and failed primary repairs demonstrated significant functional improvement following reconstruction in this series. All patients achieved improved ROM, and six of seven patients had complete resolution of extension lag. The single patient with residual extension lag had multiple fractures and was treated with multiple surgical procedures. He had a longer duration of chronicity as well, which may have contributed to persistent quadriceps weakness. There were no re-rupture cases in either of the categories, which is consistent with the reported low rupture rates with autograft reconstruction, when proper fixation methods are advocated [17].
Comparison with existing literature
The functional outcomes of this case series were evaluated using the Lysholm and the Kujala scores. The improvements in both scores were comparable with those reported in previous studies on chronic patellar tendon reconstruction using hamstring and peroneus longus autograft [10,16,17]. Even though the hamstring tendon remains the most common autograft for patellar tendon reconstruction, this series adds credence to the growing body of data that supports the peroneus longus tendon as a reconstruction option [11,18,19]. The use of both graft types allowed individualized treatment based on defect size, tissue quality, and surgical requirements.
Retrospective design, small sample size, and lack of a control group are the major limitations of this series. In addition, extended follow-up is needed to evaluate potential long-term complications, such as patellofemoral arthritis. However, this case-based analysis provides valuable information on the management of complex patellar tendon deficiencies.
Patellar tendon reconstruction in cases of chronic rupture or failed primary repair provides satisfactory functional outcomes when proper graft harvesting and fixation techniques are used. Tailoring both the choice of graft and the fixation method to each patient is essential for a successful reconstruction. Autografts, either hamstring or peroneus longus tendons, can be successfully harvested and fashioned to restore the patellar tendon function with excellent length, strength, and minimal donor site morbidity.
1. Chronic ruptures are best treated with reconstruction rather than repair
2. Autografts can provide better strength and longevity for reconstruction
3. Hamstring grafts are effective but may be limited in chronic/revision cases
4. The peroneus longus tendon offers excellent length and strength with minimal morbidity and is an excellent choice in revision surgeries
5. Restoration of patellar height is critical for better results.
References
- 1. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am 1981;63:932-7. [Google Scholar] [PubMed]
- 2. O’Dowd JA, Lehoang DM, Butler RR, Dewitt DO, Mirzayan R. Operative treatment of acute patellar tendon ruptures. Am J Sports Med 2020;48:2686-91. [Google Scholar] [PubMed]
- 3. Lyons JG, Mian HM, Via GG, Brueggeman DA, Krishnamurthy AB. Trends and epidemiology of knee extensor mechanism injuries presenting to United States emergency departments from 2001 to 2020. Phys Sportsmed 2023;51:183-92. [Google Scholar] [PubMed]
- 4. Gilmore JH, Clayton-Smith ZJ, Aguilar M, Pneumaticos SG, Giannoudis PV. Reconstruction techniques and clinical results of patellar tendon ruptures: Evidence today. Knee 2015;22:148-55. [Google Scholar] [PubMed]
- 5. Kovacev N, Antic J, Gvozdenovic N, Obradovic M, Vranjes M, Milankov M. Patellar tendon rupture–treatment results. Med Pregl. 2015;68:22-28. [Google Scholar] [PubMed]
- 6. Brinkman JC, Reeson E, Chhabra A. Acute patellar tendon ruptures: An update on management. J Am Acad Orthop Surg Glob Res Rev.2024 Apr 3;8(4):e24.00060. [Google Scholar] [PubMed]
- 7. Ginesin EZ, Wojnowski NM, Patel RM. Patellar tendon reconstruction for a chronic extensor mechanism deficit using an Achilles tendon allograft with hamstring autograft and suture augmentation. Arthrosc Tech 2020;9:e469-75. [Google Scholar] [PubMed]
- 8. Haj Shehadeh T, Kawtharani F. Delta technique reconstruction of a failed patellar tendon repair: A case report. J Orthop Exp Innov 2023;4:1-4. [Google Scholar] [PubMed]
- 9. Insall J, Salvati E. Patella position in the normal knee joint. Radiology 1971;101:101-4. [Google Scholar] [PubMed]
- 10. Gilmore JH, Clayton-smith ZJ, Aguilar M, Pneumaticos SG, Giannoudis PV. Reconstruction techniques for chronic patellar tendon ruptures. Am J Sports Med 2015;43:182-9. [Google Scholar] [PubMed]
- 11. Kerimoğlu S, Aynaci O, Saraçoğlu M, Aydin H, Turhan AU. Anterior cruciate ligament reconstruction with the peroneus longus tendon. Acta Orthop Traumatol Turc 2008;42:38-43. [Google Scholar] [PubMed]
- 12. Maffulli N, Del Buono A, Oliva F, Giai Via A, Frizziero A.Chronic rupture of the patellar tendon.The Journal of Bone and Joint Surgery. British Volume. 2006;88-B(11):1479–1485PD [Google Scholar] [PubMed]
- 13. McNally, EA Marcelli Reconstruction of chronic patellar tendon ruptures with Achilles tendon allograft. Clin Orthop Relat Res 1998;349:159-65. [Google Scholar] [PubMed]
- 14. Chen B, Li R, Zhang S.Synthetic ligament reconstruction for patellar tendon rupture. Knee 2012;19:523-528. [Google Scholar] [PubMed]
- 15. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am. 1979;61:884-6. [Google Scholar] [PubMed]
- 16. Sundararajan SR, Srikanth KP, Rajasekaran S.Neglected patellar tendon ruptures: a simple modified reconstruction using hamstrings tendon graft. [Google Scholar] [PubMed]
- 17. International Orthopaedics (SICOT). 2013;37(11):2159–2164. [Google Scholar] [PubMed]
- 18. Temponi EF, Camelo N, Tuteja S, Thaunat M, Sonnery-Cottet B.Reconstruction of chronic patellar tendon rupture with hamstring tendons: a surgical technique.Knee Surgery, Sports Traumatology, Arthroscopy. 2016;24(8):2465–2471. [Google Scholar] [PubMed]
- 19. Zhang H, Chen S, Wang Y, Li X, Jiang J, Hua Y.Biomechanical comparison of the peroneus longus tendon and hamstring tendons for anterior cruciate ligament reconstruction.Clinical Biomechanics. 2017;44:96–101. [Google Scholar] [PubMed]
- 20. Rhatomy S, Asikin AI, Wardani AE, Rukmoyo T, Lumban-Gaol I, Budhiparama NC.Peroneus longus tendon autograft for anterior cruciate ligament reconstruction: a systematic review.Arthroscopy: The Journal of Arthroscopic and Related Surgery. 2019;35(6):1882–1890. [Google Scholar] [PubMed]
- 21. Ozkan K, Aydin A, Ozkan FU, Onder H, Ozalay M.Reconstruction of chronic patellar tendon ruptures with peroneus longus tendon autograft.Archives of Orthopaedic and Trauma Surgery. 2010;130(1):107–112. [Google Scholar] [PubMed]
- 22. Angthong C, Chernchujit B, Apivatgaroon A, Chaijenkit K, Nualon P, Suchao-in K. Donor-site morbidity after peroneus longus harvest. Foot Ankle Int 2015;36:1113-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Case of Chronic Neglected Patellar Tendon Rupture Reconstruction Using Semitendinosus and Gracilis Tendon Autologous Graft
March 1, 2026 Case of Chronic Neglected Patellar Tendon Rupture Reconstruction Using Semitendinosus and Gracilis Tendon Autologous Graft July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study May 1, 2026 Comparative Evaluation of Peroneus Longus Tendon and Hamstring Tendon Autografts in Primary Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial
May 1, 2026 Comparative Evaluation of Peroneus Longus Tendon and Hamstring Tendon Autografts in Primary Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial