
In this pilot study, multimodal rehabilitation using either Therapeutic Exercise or Muscle Energy Technique combined with TENS was associated with improvements in pain, range of motion, and functional outcomes during early recovery following ACL reconstruction. These findings are preliminary and should be interpreted with caution.
Dr. Danishta, NIMS University, Jaipur, Rajasthan, India. E-mail: drdanishtaupums@gmail.com
Abstract
Introduction: Anterior cruciate ligament (ACL) reconstruction is frequently followed by post-operative pain, restricted knee range of motion (ROM), and functional limitations. Multimodal rehabilitation approaches, such as therapeutic exercise (TE), muscle energy technique (MET), and transcutaneous electrical nerve stimulation (TENS) are commonly used; however, comparative evidence on combined interventions remains limited. This study aimed to compare the effects of TE combined with TENS and MET combined with TENS on pain intensity, knee ROM, and functional outcomes following ACL reconstruction.
Materials and Methods: A prospective, non-randomized pilot study was conducted on 40 participants (18–40 years) who had undergone ACL reconstruction. Participants were allocated into two groups: Group A received TE plus TENS, and Group B received MET plus TENS. Interventions were administered for 5 weeks. Outcome measures included the numeric pain rating scale (NPRS), goniometric assessment of knee flexion and extension, and the knee injury and osteoarthritis outcome score (KOOS). Assessments were performed at baseline, Day 14, and Day 35. Data were analyzed using repeated-measures analysis of variance with post hoc comparisons.
Results: Both groups demonstrated significant reductions in pain intensity over time (P < 0.001). A significant Time × Group interaction (P = 0.017) indicated statistically faster early pain relief in the MET + TENS group. Knee flexion and extension improved significantly in both groups (P < 0.001), with no significant between-group differences (P = 0.115). KOOS subscale scores (pain, symptoms, activities of daily living, sports/recreation, and quality of life) improved significantly in both groups (P < 0.001), with comparable functional gains (P = 0.091).
Conclusion: This prospective pilot study suggests that both TE combined with TENS and MET combined with TENS are associated with short-term improvements in pain, knee ROM, and functional outcomes following ACL reconstruction.
Keywords: Anterior cruciate ligament reconstruction, muscle energy technique, therapeutic exercise, transcutaneous electrical nerve stimulation, knee function.
Anterior cruciate ligament (ACL) injuries are among the most common musculoskeletal conditions affecting young adults, athletes, and physically active individuals. ACL ruptures constitute a substantial proportion of knee ligament injuries and are frequently associated with pain, joint instability, functional impairment, and reduced quality of life (QOL) [1,2]. Surgical reconstruction is widely regarded as the gold standard for restoring mechanical stability of the knee and minimizing the risk of long-term degenerative changes [3]. However, despite successful surgical intervention, many patients continue to experience persistent deficits in muscle strength, proprioception, joint mobility, and overall knee function, underscoring the critical role of structured post-operative rehabilitation in optimizing recovery outcomes [4].
Post-ACL reconstruction rehabilitation traditionally emphasizes therapeutic exercise (TE) programs aimed at restoring muscle strength, joint range of motion (ROM), neuromuscular control, and functional performance. Substantial evidence supports the effectiveness of TE in reducing post-operative pain, improving mobility, and facilitating return to activity [4]. Muscle energy technique (MET) is a manual therapy approach designed to improve muscle extensibility through therapist-guided isometric muscle contractions followed by passive stretching. MET primarily targets neuromuscular relaxation, reduction of muscle hypertonicity, and enhancement of joint mobility rather than direct strength development [5]. Transcutaneous electrical nerve stimulation (TENS) is frequently incorporated during the early phases of rehabilitation for pain modulation, thereby improving patient comfort and enabling active participation in therapeutic interventions [6].
Although TE, MET, and TENS are widely used in clinical practice, most studies have evaluated these modalities individually rather than in combination. Evidence regarding their combined application as integrated rehabilitation strategies remains limited, and findings are inconsistent as to whether multimodal approaches provide superior functional recovery compared with conventional exercise-based rehabilitation alone [7]. Furthermore, research examining combined rehabilitation protocols within Indian clinical populations is scarce, highlighting the need for context-specific evidence to inform clinical decision-making.
Recent evidence suggests that combining TE or MET with TENS may enhance pain relief, improve knee ROM, and accelerate functional recovery following ACL reconstruction. However, comparative evidence evaluating the relative effectiveness of TE versus MET when combined with TENS remains insufficient. Therefore, the purpose of the present study was to compare the effects of TE combined with TENS and MET combined with TENS on pain intensity, knee ROM, and functional outcomes in patients following ACL reconstruction. By addressing this research gap, the study aims to provide preliminary evidence on differential early recovery patterns associated with distinct multimodal rehabilitation strategies and to support informed, patient-specific post-operative rehabilitation planning.
Study design
This study employed a prospective, non-randomized interventional repeated-measures pilot design to evaluate the effects of TE and MET combined with TENS on recovery following ACL reconstruction. The repeated-measures approach allowed assessment of changes in pain, knee ROM, and functional outcomes at multiple stages of post-operative rehabilitation. Participants were allocated using a convenience-based non-randomized approach due to feasibility constraints of this pilot study. This was a pilot study and was not registered as a clinical trial.
Study setting
The study was carried out in the NIMS Hospital’s Department of Orthopedics, where patients frequently participate in organized post-operative ACL rehabilitation programs.
Participants
Inclusion criteria
- Male and female participants
- Age between 18 and 40 years
- Individuals who had undergone ACL reconstruction
- Medical clearance from the treating physician to participate in rehabilitation exercises
- No history of other knee surgeries within the previous year
- Presence of post-operative pain, reduced knee ROM, or muscle weakness
- Willingness to follow the research procedure and give written informed consent.
Exclusion criteria
- Presence of infection, severe swelling, or open wounds affecting the operated knee
- Combined ligament injuries (posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament injuries)
- Neurological disorders affecting lower limb function (e.g., stroke, peripheral neuropathy)
- Pre-existing severe osteoarthritis or other conditions limiting participation in rehabilitation
- Uncontrolled diabetes mellitus, cardiovascular disease, or severe hypertension
- Any new knee trauma or injury during the study period
- Inability to attend regular physiotherapy sessions or comply with the intervention protocol.
Although both male and female participants were included, the study was not powered to perform sex-specific subgroup analyses.
Sample size and sampling
Forty people in all were recruited based on feasibility and patient availability during the study period. A convenience sampling method was employed. As this was an exploratory pilot study, no a priori sample size or power calculation was performed.
Interventions
All interventions were administered and supervised by qualified physiotherapists to ensure correct technique, safety, and adherence to protocol. A non-randomized assignment method was used to divide the participants into two groups.
- Group A: TE + TENS
- Group B: MET + TENS.
TE protocol
Participants in Group A received a structured TE program divided into three progressive phases:
Phase I (2–7 days post-surgery)
Passive knee extension (over-pressure), ankle pumps, passive and active knee flexion, straight leg raises (flexion, adduction, and abduction), quadriceps isometric exercises, hamstring stretching, multi-angle isometric strengthening, standing hamstring curls, and mini-squats.
Phase II (2–3 weeks)
All Phase I exercises with the addition of leg press, leg extension, half squats, prone hamstring curls, cycling, patellar mobilization, passive ROM exercises, stair climbing, and proprioceptive training.
Phase III (4–5 weeks)
Continuation of previous exercises along with wall squats, calf raises, walking exercises, standing balance training on a tilt board, and isokinetic exercises.
The TE program aimed to restore knee stability, muscle strength, joint mobility, and functional performance.
MET
Participants in Group B received MET. MET targeted muscles commonly affected following ACL reconstruction, including the quadriceps, hamstrings, gastrocnemius, hip flexors, gluteal muscles, and adductors. This intervention aimed to improve muscle extensibility, neuromuscular control, joint mobility, and pain modulation, thereby facilitating active participation in post-operative rehabilitation exercises.
Quadriceps (vastus medialis and vastus lateralis)
- Rationale: Quadriceps inhibition is common after ACL reconstruction, compromising knee extension, patellar tracking, and functional stability
- Protocol: Isometric contraction for 5–7 s followed by gentle passive stretching for 30 s; repeated 3–5 cycles.
Hamstrings
- Rationale: Tight hamstrings can limit knee flexion and functional mobility
- Protocol: Isometric contraction for 5–7 s followed by passive stretching for 30 s; repeated 3–5 times per session.
Gastrocnemius
- Rationale: Gastrocnemius tightness may impede terminal knee extension and alter gait mechanics
- Protocol: Isometric contraction against resistance for 5–7 s followed by passive stretching; 3–5 repetitions.
Hip muscles (gluteus maximus, gluteus medius, and hip flexors)
- Rationale: Weak or imbalanced hip muscles can lead to altered lower-limb kinematics, knee valgus, and reduced functional performance
- Protocol: Short isometric contractions for 5–7 s followed by targeted passive stretching; repeated 3–5 times per muscle group.
Adductors
- Rationale: Tight adductors may contribute to medial knee stress and impaired alignment
- Protocol: Isometric contraction followed by gentle passive stretching; repeated 3–5 times.
TENS
TENS was applied to both groups in conventional mode with the following parameters:
- Frequency: 80–100 Hz
- Pulse width: 50–80 µs
- Duration: 20 min.
TENS was used to reduce post-operative pain and facilitate active participation in rehabilitation sessions. Adherence to home-based exercise programs outside supervised sessions was not formally monitored.
Outcome measures
Numeric pain rating scale (NPRS)
The NPRS (0 = no pain, 10 = worst imaginable pain) was used to assess pain intensity. NPRS demonstrates high test–retest reliability (intraclass correlation coefficient [ICC] = 0.85–0.95) and sensitivity to clinically meaningful changes in pain intensity [8].
Goniometric measurement of knee ROM
A universal goniometer was used to measure knee flexion and extension. The axis was positioned over the lateral femoral epicondyle, with the fixed arm aligned toward the greater trochanter and the movable arm toward the lateral malleolus. This method demonstrates excellent intra-rater reliability (ICC = 0.90–0.98) and strong inter-rater reliability (ICC = 0.80–0.92) [9,10].
Knee injury and osteoarthritis outcome score (KOOS)
The KOOS was used to evaluate functional outcomes across five domains: Pain, symptoms, activities of daily living (ADL), sports and recreation, and QOL. Scores range from 0 to 100, with higher scores indicating better knee function. KOOS demonstrates excellent test–retest reliability and internal consistency [11,12,13].
Data collection procedure
Outcome measures were recorded at three time points: Baseline, Day 14, and Day 35. To reduce inter-observer variability and improve consistency, all assessments were conducted by the same qualified physiotherapist.
Ethical considerations
The study was approved by the Institutional Ethics Committee of NIMS University (IEC No: NIMS/PT/OT/April/2024/46). Written informed consent was obtained from all participants before enrolment. The study was conducted in accordance with the Declaration of Helsinki.
Data analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences software (version 26; IBM Corp., Armonk, NY, USA). Repeated-measures analysis of variance with Greenhouse–Geisser correction and Bonferroni post hoc tests were applied. Statistical significance was set at P < 0.05.
Pain intensity decreased significantly over time in both groups, with a significant Time × Group interaction indicating a difference in the rate of pain reduction (Tables 1, 2, 3).
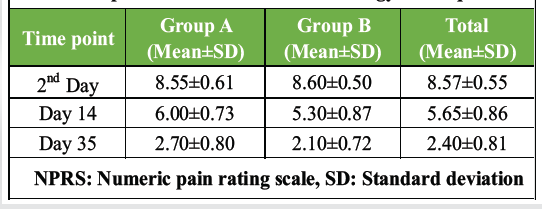
Table 1: Comparative analysis of NPRS scores between
therapeutic exercise and muscle energy technique
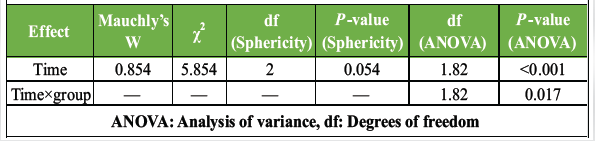
Table 2: Sphericity test and repeated measures ANOVA
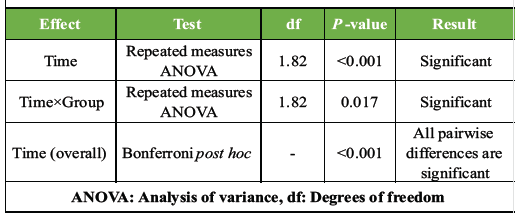
Table 3: Summary of repeated measures ANOVA and post hoc results
Knee ROM, including flexion and extension, improved significantly over the 5-week rehabilitation period in both groups (P < 0.001). However, no significant Time × Group interaction was observed for knee flexion or extension (P = 0.115), indicating comparable improvements between the TE + TENS and MET + TENS groups (Tables 4, 5, 6).
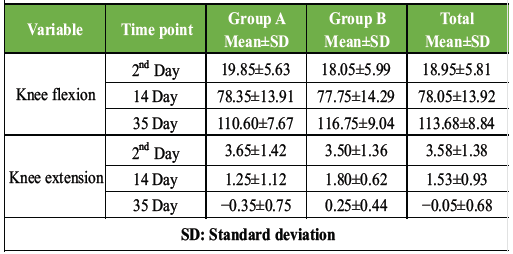
Table 4: Comparative analysis of goniometer (knee flexion and extension) between therapeutic exercise and muscle energy technique
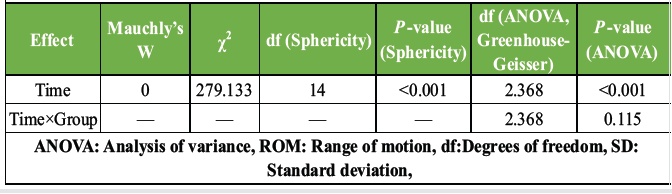
Table 5: Sphericity test and repeated measures ANOVA – knee ROM
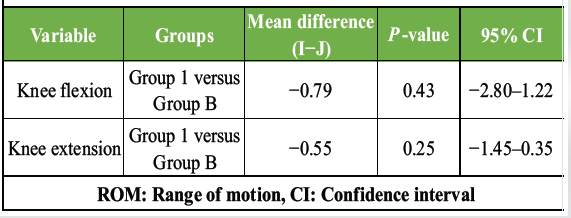
Table 6: Pair-wise comparisons – Knee ROM between groups
All KOOS subscales (pain, symptoms, ADL, sports/recreation, and QOL) showed significant improvements over time in both groups (P < 0.001). No significant Time × Group interaction was observed (P = 0.091), indicating comparable functional recovery between groups (Tables 7, 8, 9).
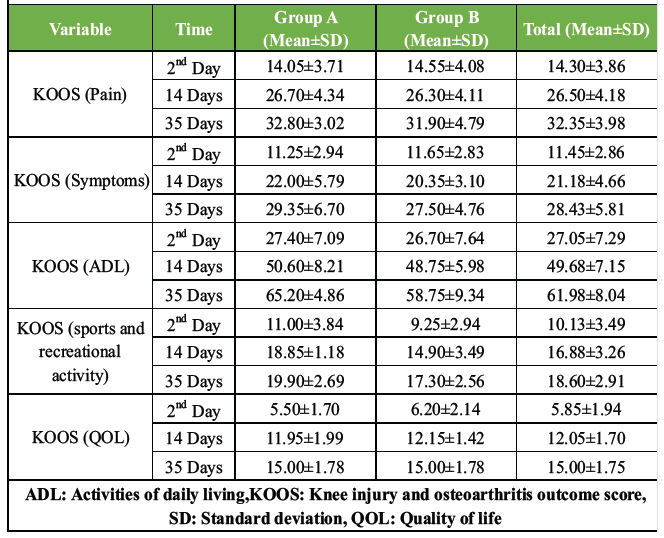
Table 7: Comparative analysis of KOOS between therapeutic exercise and muscle energy technique
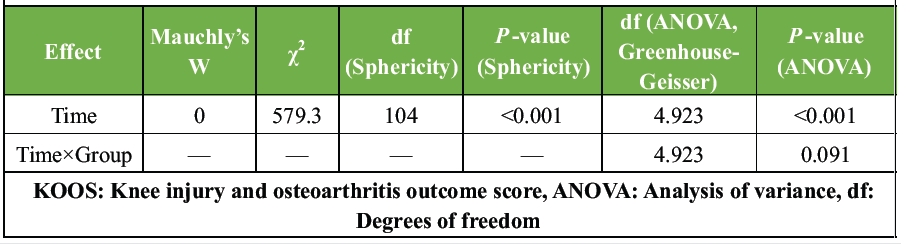
Table 8: Sphericity test and repeated measures ANOVA – KOOS
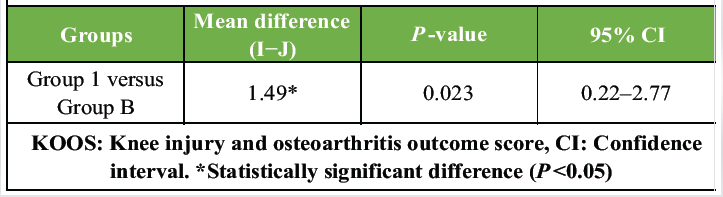
Table 9: Pairwise comparisons – KOOS between groups
The present study compared the effects of TE combined with TENS (TE + TENS) and MET combined with TENS (MET + TENS) on pain intensity, knee ROM, and functional outcomes following ACL reconstruction. The findings suggest that both rehabilitation approaches were effective in improving post-operative outcomes over the 5-week intervention period, with only minor differences observed in early pain reduction patterns.
Pain intensity decreased significantly in both groups, with a statistically significant but modestly faster early pain reduction observed in the MET + TENS group. This finding is consistent with previous evidence indicating that TENS produces analgesic effects through modulation of nociceptive input and activation of endogenous inhibitory mechanisms [6,14]. The additional early pain relief associated with MET may be related to neuromuscular relaxation, reduction of muscle hypertonicity, and improved local circulation, which may be particularly beneficial during the immediate post-operative phase [15,16]. However, the magnitude of the observed difference was small, and its clinical significance remains uncertain. In contrast, TE emphasizes progressive strengthening and neuromuscular re-education, which may contribute to a more gradual trajectory of pain reduction.
Knee flexion and extension improved significantly in both groups, with no significant between-group differences, suggesting that TE + TENS and MET + TENS may be similarly effective in restoring knee ROM during early post-operative rehabilitation. These findings are consistent with previous research demonstrating that both active exercise-based interventions and manual therapy techniques can improve joint mobility through distinct physiological mechanisms [17,18,19].
Functional outcomes, assessed using the KOOS, improved significantly across all domains in both groups, with no significant between-group differences. These results support the use of multimodal rehabilitation approaches integrating exercise or manual therapy with electrotherapy modalities to facilitate functional recovery following ACL reconstruction. However, given the short follow-up duration and pilot nature of the study, these findings should be interpreted cautiously and cannot be extrapolated to long-term functional outcomes.
Clinical implications
The findings of this pilot study have several practical implications for post-operative ACL rehabilitation:
- Multimodal approaches are effective: Both TE + TENS and MET + TENS are effective strategies for early recovery after ACL reconstruction. Clinicians can confidently incorporate either approach based on patient preferences, tolerance, or specific clinical indications
- Pain management: MET combined with TENS may offer faster early-phase pain relief, which could enhance patient comfort and adherence to rehabilitation programs
- Functional recovery: Since both approaches produce comparable improvements in ROM and functional outcomes, rehabilitation programs can be individualized without compromising overall recovery
- Resource optimization: In settings where physiotherapy resources are limited, either method may be employed effectively, while TENS can be integrated as a non-invasive adjunct to facilitate greater exercise tolerance.
Limitations
Non-randomized study design
Participants were allocated using a non-randomized, convenience-based approach; therefore, the possibility of selection bias cannot be excluded. Differences in unmeasured baseline characteristics may have influenced group comparability and outcome responses.
Absence of a true control group
The study did not include a control group receiving standard rehabilitation alone, which limits the ability to determine the independent contribution of TE or MET beyond natural post-operative recovery and the analgesic effects of TENS.
Small sample size and lack of power calculation
As a pilot study with a total sample size of 40 participants, no a priori sample size calculation was performed. Consequently, the study may have been underpowered to detect smaller but clinically meaningful differences between interventions or to conduct subgroup analyses.
Short follow-up duration
Outcomes were assessed over a 5-week period only, which does not capture long-term recovery, graft integrity, neuromuscular control, proprioceptive function, or return-to-sport outcomes.
Single-center study
This study was conducted at a single clinical center, which may limit the generalizability of the findings to other rehabilitation settings or patient populations.
Convenience sampling
Participants were recruited using convenience sampling based on availability, which may not accurately represent the broader population of individuals undergoing ACL reconstruction.
Lack of blinding
Blinding of participants and outcome assessors was not feasible due to the nature of the interventions, which may have introduced performance and measurement bias.
Home exercise program adherence
Adherence to prescribed home-based exercise programs was not formally monitored, which could have influenced individual rehabilitation outcomes.
Therapist-dependent intervention delivery
Although standardized intervention protocols were followed, the effectiveness of the MET may vary depending on therapist skill and experience, potentially affecting reproducibility across different clinical settings.
Use of tens in both groups
The application of TENS in both intervention groups limits the ability to isolate the independent effects of TE and MET.
Lack of surgical stratification
Surgical variables, such as graft type and reconstruction technique were not stratified or controlled, which may have influenced post-operative recovery patterns.
Limited outcome measures
Objective measures of muscle strength, proprioception, balance, and functional performance were not included, limiting a comprehensive assessment of rehabilitation outcomes.
Future directions
Future research should include larger, randomized controlled trials with longer follow-up periods to evaluate long-term functional outcomes, graft stability, and return-to-sport readiness. Investigating the combination of MET and TE with TENS in a hybrid protocol may also provide insights into whether synergistic effects exist. In addition, monitoring adherence to home-based exercises and including objective measures of muscle strength, proprioception, and balance could enhance the understanding of the mechanisms underlying recovery.
This prospective pilot study suggests that both TE combined with TENS and MET combined with TENS are associated with short-term improvements in pain, knee ROM, and functional outcomes following ACL reconstruction. Although MET combined with TENS demonstrated a modest advantage in early pain reduction, both interventions yielded comparable improvements in ROM and functional outcomes. These results support individualized rehabilitation planning based on patient tolerance, clinical presentation, and therapist expertise. However, these findings are preliminary and should be confirmed in larger randomized controlled trials with longer follow-up durations to establish long-term effectiveness and clinical significance.
Both TE + TENS and MET + TENS can be safely used after ACL reconstruction, allowing clinicians to individualize rehabilitation based on patient pain tolerance and early recovery goals.
References
- 1. Van Grinsven S, Van Cingel RE, Holla CJ, Van Loon CJ. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2010;18:1128-44. [Google Scholar] [PubMed]
- 2. Spindler KP, Wright RW. Clinical practice. Anterior cruciate ligament tear. N Engl J Med 2008;359:2135-42. [Google Scholar] [PubMed]
- 3. Adams D, Logerstedt DS, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current concepts for anterior cruciate ligament reconstruction: A criterion-based rehabilitation progression. J Orthop Sports Phys Ther 2012;42:601-14. [Google Scholar] [PubMed]
- 4. Scranton PE. Rehabilitation following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 2009;39:234-9. [Google Scholar] [PubMed]
- 5. Fryer G. Muscle energy technique: An evidence-informed approach. Int J Osteopath Med 2011;14:3-9. [Google Scholar] [PubMed]
- 6. Johnson M. Transcutaneous electrical nerve stimulation: Mechanisms, clinical application and evidence. Rev Pain 2007;1:7-11. [Google Scholar] [PubMed]
- 7. Wang Y, Zhang H, Liu X, Chen J. Multimodal rehabilitation strategies following anterior cruciate ligament reconstruction: A comparative analysis. J Sports Rehabil 2025;34:145-54. [Google Scholar] [PubMed]
- 8. Williamson A, Hoggart B. Pain: A review of three commonly used pain rating scales. J Clin Nurs 2005;14:798-804. [Google Scholar] [PubMed]
- 9. Norkin CC, White DJ. Measurement of Joint Motion: A Guide to Goniometry. 5th ed. Philadelphia, PA: FA Davis; 2016. [Google Scholar] [PubMed]
- 10. Clarkson HM. Musculoskeletal Assessment: Joint Range of Motion and Manual Muscle Strength. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2013. [Google Scholar] [PubMed]
- 11. Roos EM, Lohmander LS. The knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual Life Outcomes 2003;1:64. [Google Scholar] [PubMed]
- 12. Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 2006;34:156-64. [Google Scholar] [PubMed]
- 13. Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International knee documentation committee (IKDC) subjective knee evaluation form, knee injury and osteoarthritis outcome score (KOOS), knee injury and osteoarthritis outcome score physical function short form (KOOS-PS), knee outcome survey activities of daily living scale (KOS-ADL), lysholm knee scoring scale, oxford knee score (OKS), western Ontario and Mcmaster universities osteoarthritis index (WOMAC), activity rating scale (ARS), and Tegner activity score (TAS). Arthritis Care Res (Hoboken) 2011;63:S208-28. [Google Scholar] [PubMed]
- 14. Sluka KA, Walsh D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J Pain 2003;4:109-21. [Google Scholar] [PubMed]
- 15. Chaitow L. Muscle Energy Techniques. 3rd ed. Edinburgh: Churchill Livingstone; 2006. [Google Scholar] [PubMed]
- 16. Liu L, Huang QM, Liu QG, Thitham N, Li P, Ma YT. Effectiveness of muscle energy technique on pain and disability in patients with musculoskeletal disorders: A systematic review. Phys Ther Sport 2024;57:12-20. [Google Scholar] [PubMed]
- 17. Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR. Recent advances in the rehabilitation of anterior cruciate ligament injuries. J Orthop Sports Phys Ther 2012;42:153-71. [Google Scholar] [PubMed]
- 18. Danishta, Meena NK, Saharan AK, Kumar M. Efficacy of therapeutic exercise versus muscle energy technique in rehabilitation following anterior cruciate ligament reconstruction of the knee: A pilot study. Innovations 2024;77:2285-301. [Google Scholar] [PubMed]
- 19. Chen Y, Li J, Xu W. Multimodal physiotherapy approaches in postoperative knee rehabilitation: Clinical outcomes and patient satisfaction. Physiother Theory Pract 2023;39:987-95. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction
June 1, 2026 Role of Prehabilitation in Improving Outcomes after Anterior Cruciate Ligament Reconstruction July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide