
In young patients with failed bipolar hemiarthroplasty and acetabular deficiency, structural autologous iliac crest graft reconstruction offers a cost-effective, biologically favourable salvage option with good osteointegration, preserves host bone for possible rerevision, and may avoid the complications and expense of prosthetic augments or wedge implants.
Dr. Muni Srikanth Iytha, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: munisrikanth@aiimsmangalagiri.edu.in
Abstract
Introduction: Developmental dysplasia of the hip imposes significant challenges in hip arthroplasty due to altered hip anatomy, deficient bone stock, and abnormal biomechanics. Bipolar hemiarthroplasty performed in such hips carries a high risk of migration, loosening, or dislocation.
Case Report: We present the case of a 23-year-old female with failed bipolar hemiarthroplasty performed for femoral neck fracture, complicated by unrecognized acetabular dysplasia. She presented with pain, difficulty in ambulation, inability to sit cross-legged or squat, and complete restriction of hip movements. Radiographs showed proximal migration with posterior dislocation of the bipolar prosthesis and acetabular changes. After ruling out infection, she underwent implant removal followed by cemented total hip arthroplasty with acetabular reconstruction using tricortical iliac crest autograft.
Results: At 1-year follow-up, she achieved pain-free ambulation with graft incorporation on radiographs, stable acetabular fixation, and no evidence of infection or loosening.
Conclusion: In young patients with failed hemiarthroplasty and underlying dysplasia, acetabular roof reconstruction with autologous tricortical graft combined with cemented THA provides a cost-effective, biologically favorable, and bone-preserving solution.
Keywords: Developmental dysplasia of the hip, bipolar hemiarthroplasty, acetabular roof reconstruction, total hip arthroplasty, tricortical iliac crest graft.
Developmental dysplasia of the hip (DDH) is a spectrum of disorders characterized by abnormal hip joint development, leading to anatomical and biomechanical alterations with worldwide incidence rates ranging from 1.4% to 35.0% in live births [1].
When DDH is diagnosed and treated during the infant period, conservative management is generally fruitful and leads to good long-term outcomes. On the contrary, diagnosis after the child has begun walking often requires more complex surgical reconstruction and is associated with greater morbidity. In India, the reported incidence varies across the spectrum of hip dysplasia, while true DDH occurs in a much smaller proportion of live births [2].
These include a shallow and steep acetabulum, increased anteversion or retroversion, superior segmental deficiency, excessive femoral anteversion, and narrow femoral canals. Such abnormalities predispose to early degenerative changes and complicate hip reconstruction.
Bipolar hemiarthroplasty in a dysplastic acetabulum is poorly tolerated due to inadequate femoral head coverage, instability, and rapid cartilage wear, often resulting in prosthesis migration and pseudoacetabulum formation. When failure occurs, conversion to total hip arthroplasty (THA) becomes necessary. However, restoring acetabular anatomy, reconstructing deficiencies, and ensuring implant stability are technically demanding.
This report presents the successful management of a young patient with failed bipolar hemiarthroplasty in a dysplastic hip through cemented THA and acetabular reconstruction with an autologous tricortical iliac crest graft, highlighting cost-effectiveness and long-term reconstructive considerations.
A 23-year-old female presented to the outpatient department with complaints of left hip pain, difficulty in ambulation, and inability to sit cross-legged or squat. On examination, she had a surgical scar over the anterolateral aspect of the left hip, limb shortening, and restricted hip movements with no signs of sinus or infection. Neurovascular examination was normal.
She had undergone bipolar hemiarthroplasty for fracture of the neck of the femur 6 years earlier (Fig. 1a, b, c).
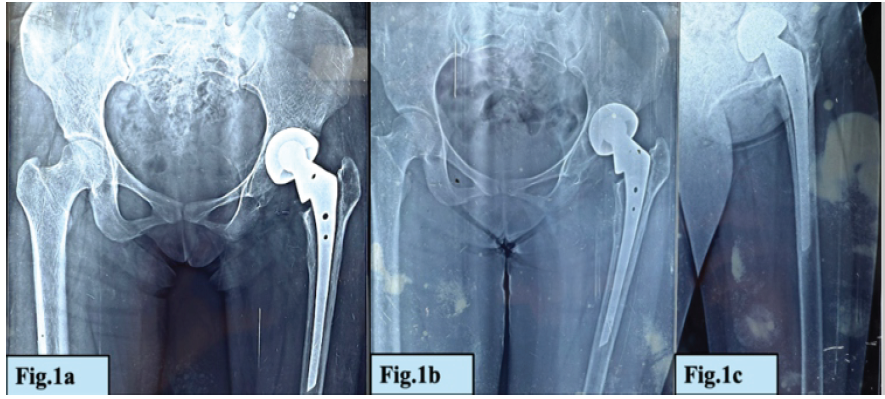
Figure 1: (a-c) X-ray radiographs of in situ bipolar hemiarthroplasty prosthesis.
Current radiographs demonstrated proximal migration of the bipolar cup with acetabular changes and posterior dislocation of the prosthesis (Fig. 2a and b).
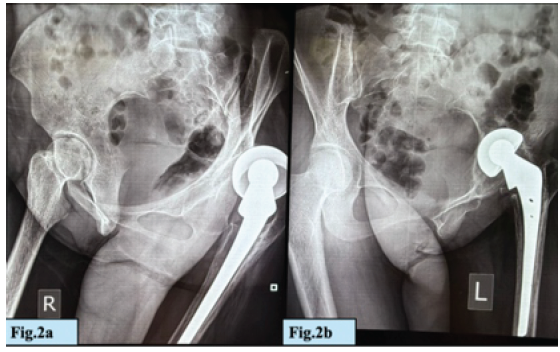
Figure 2: (a and b) Current X-ray radiographs demonstrating proximal migration of the bipolar cup with acetabular changes and posterior dislocation of the prosthesis.
Retrospective evaluation of prior records revealed underlying acetabular dysplasia not addressed during the initial surgery. Routine blood investigations, erythrocyte sedimentation rate, C-reactive protein, and joint aspiration excluded infection. Three-phase bone scan showed no abnormal tracer uptake in the left hip region. Findings were not suggestive of infection (Fig. 3).
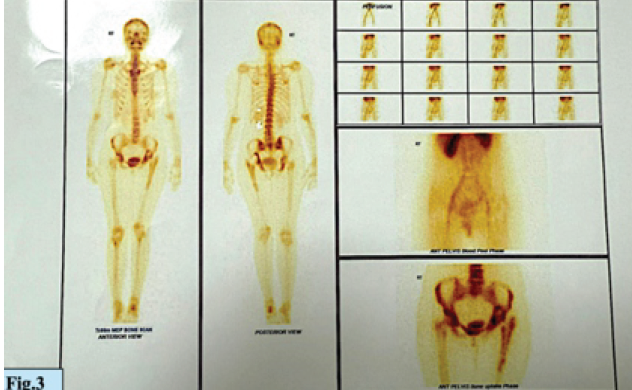
Figure 3: Three phase bone scan showed no abnormal tracer uptake in the left hip region.
A diagnosis of failed bipolar hemiarthroplasty in a dysplastic hip with pseudoacetabulum formation was made, and revision surgery with implant removal and conversion to THA was planned.
Surgical technique
The procedure was performed under regional anesthesia with the patient in the right lateral decubitus position. A posterior approach to the hip was utilized with a curvilinear incision extending from 4 finger breadths below the posterior superior iliac spine, passing over the greater trochanter, and extending distally 10 cm along the femoral shaft.
Fibrotic tissue encasing the prosthesis was excised, sent for histopathological examination and culture, and the implant was removed. A pseudoacetabulum filled with fibrous tissue was identified superior to the native but shallow acetabulum. After complete excision of fibrous tissue, a true acetabulum with a supra-acetabular defect was visualized.
To reconstruct the defect, a tricortical iliac crest autograft was harvested and fixed with cortical screws to act as a structural roof. Acetabular reaming was performed sequentially up to size 46, and a cemented acetabular component was implanted in the native position with correct inclination and anteversion. The remaining superior gap was packed with morselized cancellous bone graft and antibiotic-impregnated calcium sulfate (Stimulan) beads. It helps in new bone formation (osteoconduction). Along with this, it also helps fill the dead space formed by bone loss due to trauma, surgical bone loss, or infectious conditions [3].
The implants used included simplex bone cement, an Exeter femoral stem (cemented, 28 mm head), and an Exeter contemporary flanged acetabular cup (Fig. 4a, b, c).

Figure 4: (a-c) The implants – simplex bone cement, an Exeter femoral stem (cemented, 28 mm head), and an Exeter contemporary flanged acetabular cup.
On the femoral side, canal preparation with sequential broaches was performed, and a cemented polished femoral stem was implanted to allow version control. Trial reduction confirmed stability. Limb length discrepancy was corrected intraoperatively, and combined anteversion was verified using the Ranawat coplanar and Shuck tests. After meticulous hemostasis, closure was done in layers.
The post-operative period was uneventful. The patient was mobilized with partial weight bearing from the 3rd post-operative day and progressed to full weight bearing by 6 weeks. At 1-year follow-up, she reported no pain, was able to walk without support, and regained the ability to sit cross-legged and squat.
X-ray left hip confirmed good graft incorporation and stable implant positioning with no radiolucent lines or signs of acetabular loosening (Fig. 5a, b, c, d).
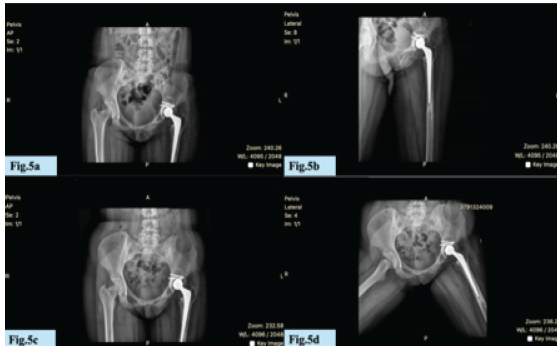
Figure 5: (a-d) X-ray left hip with good graft incorporation and stable implant positioning with no radiolucent lines or signs of acetabular loosening.
Computerized tomography hip preoperatively displayed acetabular roof superior wall defect (Fig.6a) while follow-up showed a well-united bone graft in the posterior superior acetabulum with trabeculated bone bridging between the graft and native bone. No peri-implant lucency was noted. The acetabular and femoral components were well-positioned and stable (Fig. 6b). Functional outcome was rated as excellent according to the Harris Hip Score.
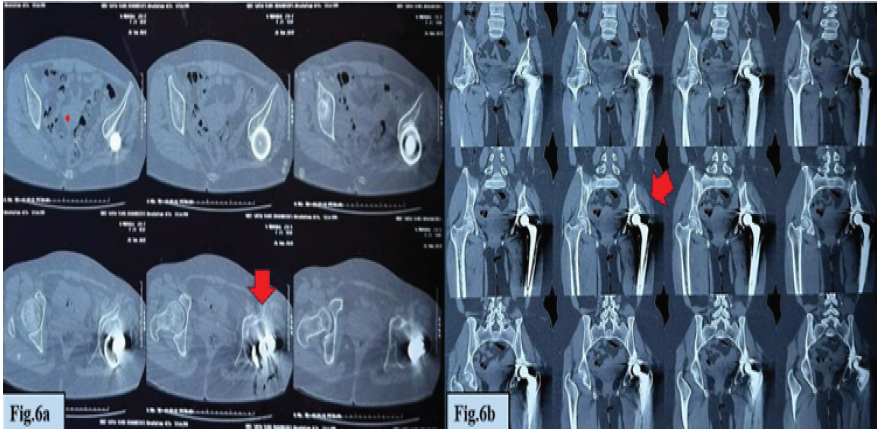
Figure 6: (a) Computed tomography (CT) hip (pre-operative) – showing acetabular roof superior wall defect (red arrow). (b) CT hip (follow-up) showing a well-united bone graft in the posterior superior acetabulum with trabeculated bone bridging between the graft and native bone (red arrow).
THA after failed hemiarthroplasty in dysplastic hips requires consideration of multiple factors, including acetabular reconstruction, implant choice, and bone preservation for future revisions.
Acetabular challenges
The dysplastic acetabulum is deficient in coverage, shallow, and misoriented; superior bone stock is often compromised due to pseudoacetabulum formation, as seen in our case. Unaddressed, these defects lead to superior migration of implants and premature failure [4].
Reconstruction techniques in literature
Various strategies have been described for acetabular reconstruction in DDH:
- Failed hemiarthroplasty revision with total hip replacement has been reported as a challenging but feasible option in dysplastic hips [5]
- Cemented fixation with bone grafts: Bone stock deficiency, particularly in the superolateral region, is a common problem and often results in partial uncovering of the acetabular cup. To ensure primary stability and allow adequate bony ingrowth, at least 70% of the cup must be supported and covered by the native host bone [6]. Roof reconstruction with iliac crest graft provides biological incorporation and long-term stability [7]
- Modular metal augments: Provide mechanical stability while protecting underlying grafts [7]
- Structural acetabular allografts with reconstruction rings: Offer additional support in severe deficiencies [8]
- Beyond defect filling, structural grafting restores bone stock and hip biomechanics, preserving future revision options [9].
- Cotyloplasty (medial protrusion): Creates new acetabular coverage by medializing the hip center but risks fracture and intrapelvic complications [10]
- High cup placement: A technically easier option, though leading to altered biomechanics, increased joint reaction force, and high loosening rates [4].
While metallic augments and custom implants offer excellent outcomes, their availability and cost limit their use in developing healthcare settings. Moreover, biologic options such as autologous grafts remain desirable in younger patients due to their remodeling potential and role in preserving host bone stock [4].
Rationale for our approach
In this young patient, we prioritized biological reconstruction and bone preservation for potential future revisions. The tricortical iliac crest graft provided structural integrity to restore superior coverage, while cement fixation of both acetabular and femoral components ensured stable initial fixation in compromised bone stock [4]. The addition of calcium sulfate beads offered both defect filling and localized antibiotic prophylaxis.
Clinical relevance
Studies have reported satisfactory long-term outcomes with iliac crest grafts in dysplastic hips when rigidly fixed and loaded appropriately [4,7]. Our result aligns with these reports, supporting the practice of autologous graft reconstruction in young resource-limited patients. Although cementless fixation is generally preferred in young patients, cemented fixation was chosen in our case to achieve optimal stability in abnormal bone anatomy and preserve bone for subsequent revision possibilities [5].
This case highlights the complexities of THA in failed hemiarthroplasty associated with dysplastic hips. The use of an autologous tricortical iliac crest graft for acetabular roof reconstruction and cemented THA provided a stable, biological, and cost-effective outcome in a young patient. At 1-year follow-up, the patient achieved pain-free function with successful graft incorporation. The technique remains valuable where advanced reconstructive implants are unavailable or unaffordable, particularly in young patients requiring preservation of host bone for future revision surgery.
Neglected bipolar hemiarthroplasty dislocation associated with acetabular wall defects in young adults can be effectively managed with acetabular reconstruction using autologous iliac crest bone graft and stable fixation, offering a viable salvage option and preserving native hip biomechanics while delaying the need for THA.
References
- 1. Chen X, Liu J, Xue M, Zou C, Lu J, Wang X, et al. Risk factors of developmental dysplasia of the hip in infants: A meta-analysis based on cohort studies. Orthop Traumatol Surg Res 2024;110:103836. [Google Scholar] [PubMed]
- 2. Aroojis A, Anne RP, Li J, Schaeffer E, Ananda Kesavan TM, Shah S, et al. Surveillance for developmental dysplasia of the hip in India: Consensus guidelines from the pediatric orthopaedic society of India, Indian academy of pediatrics, national neonatology forum of India, Indian radiological and imaging association, Indian federation of ultrasound in medicine and biology, federation of obstetric and gynaecological societies of India, and Indian orthopaedic association. Indian Pediatr 2022;59:626-35. [Google Scholar] [PubMed]
- 3. Krishna VJB, Kadur SJM, Kumre RN. Study and analysis of effect of calcium sulphate augmented with antibiotics in orthopaedic practice. Nat J Clin Orthop. 2021;5(4):91-97. [Google Scholar] [PubMed]
- 4. Hartofilakidis G, Karachalios T. Total hip arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 2004;86-B:876-84. [Google Scholar] [PubMed]
- 5. Charnley G, Feagin JA. Failed hemiarthroplasty for femoral neck fracture in dysplastic hips: Revision with total hip replacement. Clin Orthop Relat Res 1992;278:122-9. [Google Scholar] [PubMed]
- 6. Wang Y. Current concepts in developmental dysplasia of the hip and total hip arthroplasty. Arthroplasty 2019;1:2. [Google Scholar] [PubMed]
- 7. Slooff TJ, Schimmel JW, Buma P. Cemented fixation with bone grafts of the acetabulum in revision total hip arthroplasty. Clin Orthop Relat Res 1996;324:98-110. [Google Scholar] [PubMed]
- 8. Gustke KA. Acetabular deficiencies in total hip arthroplasty: Treatment with modular metal augments. J Arthroplasty 2004;19 4 Suppl 1:45-50. [Google Scholar] [PubMed]
- 9. DeBoer DK, Christie MJ, Brinson MF, Morrison JC. Revision hip arthroplasty with use of structural acetabular allograft and reconstruction ring. J Bone Joint Surg Am 1994;76:575-88. [Google Scholar] [PubMed]
- 10. Malizos KN, Karachalios T, Bargiotas K. Hip arthroplasty in high hip dislocation: Techniques and results. Acta Orthop Belg 2007;73:352-60. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem
July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach