
Ceramic liner fractures may present with subtle and non-specific symptoms, and a high index of clinical suspicion is required for early diagnosis. Patient education regarding abnormal post-operative symptoms is crucial, as delayed presentation can result in complex revision surgery and compromised outcomes.
Dr. Karthik Sangani, Department of Orthopaedics, Sunshine Bone and Joint Institute, KIMS-Sunshine Hospitals, Hyderabad, India. E-mail: karthiksang2024@gmail.com
Abstract
Introduction: Ceramic-on-ceramic (CoC) bearings are commonly used in total hip arthroplasty (THA) in younger and more active patients because of their excellent wear characteristics and biological inertness. Although advances in ceramic material science have markedly reduced femoral head fracture rates, ceramic liner fractures remain a rare but clinically important complication. Diagnosis may be difficult, as symptoms can be subtle and imaging findings inconclusive, resulting in delayed recognition.
Case Report: A 36-year-old male presented with progressive hip pain, painful squeaking, and grinding sensations 13 months after primary cementless CoC THA. Radiographs and computed tomography demonstrated periarticular radio-opacities suggestive of bearing surface failure. Revision surgery revealed an eccentrically fractured ceramic liner with associated ceramic debris. The acetabular shell and femoral stem were retained, and revision was performed using a highly cross-linked polyethylene liner and a ceramic femoral head following meticulous debridement. The patient experienced complete resolution of symptoms and demonstrated a satisfactory outcome at 1-year follow-up.
Conclusion: Ceramic liner fractures may present with non-specific symptoms and subtle imaging findings. Persistent painful squeaking following CoC THA should prompt early clinical evaluation, as timely diagnosis and appropriate revision are essential to prevent catastrophic failure and complex reconstructive surgery.
Keywords: Ceramic on ceramic, acetabulum liner fracture, bearing surface, total hip arthroplasty.
Total hip arthroplasty (THA) is a reliable and effective procedure for the management of end-stage hip pathology. In younger and more active patients, implant longevity is a key consideration, and bearing surface selection plays a crucial role in long-term outcomes. While metal-on-polyethylene bearings have demonstrated excellent survivorship, concerns regarding wear-related osteolysis have encouraged the use of alternative bearing surfaces with improved tribological properties.
Ceramic-on-ceramic (CoC) bearings were introduced to minimize wear through their high hardness, scratch resistance, and biologically inert wear particles. Advances in ceramic manufacturing have significantly improved fracture toughness, resulting in a substantial reduction in femoral head fractures with modern ceramic materials [1]. Large registry-based analyses have confirmed that contemporary ceramics have markedly lowered the risk of head fracture. However, ceramic liner fractures did not show the same decline in incidence, indicating that liner-specific failure mechanisms persist despite material improvements [1].
Ceramic liner fracture is an uncommon but clinically important complication that may present without a history of trauma. Symptoms are often subtle and include squeaking, grinding sensations, and progressive hip pain. Painful squeaking, in particular, has been identified as a warning sign and may precede liner fracture by several months [2,3]. Diagnosis can be challenging, as undisplaced liner fractures may not be evident on standard radiographs, leading to delayed recognition and underestimation of their true prevalence [2]. We report a case of a fractured ceramic liner with delayed presentation following primary cementless CoC THA, highlighting the diagnostic challenges and management considerations associated with this complication.
A 36-year-old male patient presented with a painful left hip, 13 months after an uncomplicated left THA performed elsewhere for avascular necrosis of the same hip. A cementless CoC prosthesis (DePuy) had been used, consisting of a metallic acetabular cup (52 mm), ceramic liner (32 mm), ceramic femoral head (32 mm, +5 mm offset), and an uncemented Corail femoral stem (size 12). The patient reported that he had audible squeaking from the left hip from within the 1st few months of surgery. Over the preceding several months, he developed persistent left hip pain associated with a grinding sensation and coarse crackles during range of motion, which worsened with walking and physical activity. There was no history of trauma, falls, or other inciting events. The pain severity was rated as 6/10 on a Likert scale.
On physical examination, the patient was 5 feet 7 inches tall and weighed 150 pounds. He also had limb shortening of approximately 1 cm. He had a positive Stinchfield test and pain with the left hip range of motion. Palpable crepitus was noted around the greater trochanteric region during ambulation.
Initial radiographs and computed tomography (CT) imaging (Fig. 1a and b) revealed radio-opacities around the hip joint and along the lateral aspect of the thigh, raising the suspicion of bearing surface fracture.
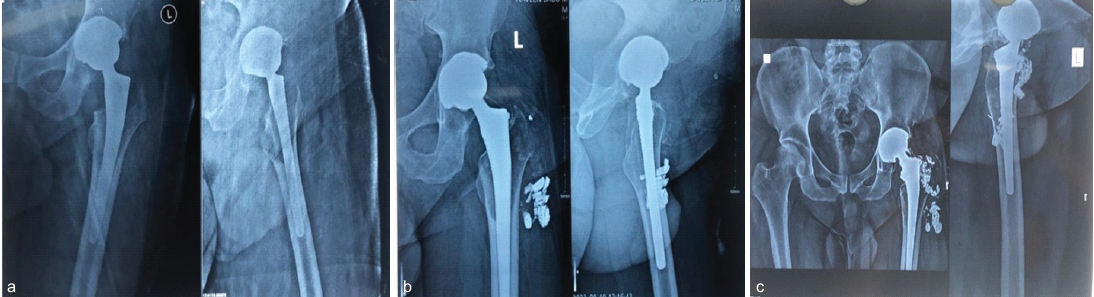
Figure 1: (a) Anteroposterior radiograph of the left hip 1 month after the index total hip arthroplasty. (b) Anteroposterior radiograph of the left hip at 11 months post-operatively, demonstrating radiodense opacities around the hip joint suggestive of bearing surface fracture. (c) Anteroposterior and lateral view radiograph of the left hip at 13 months post-operatively, showing radiodense opacities extending along the lateral aspect of the proximal thigh.
There was no evidence of osteolysis or loosening around the acetabular cup or femoral stem. An infectious workup, including erythrocyte sedimentation rate and C-reactive protein, was negative.
Revision surgery was performed through a posterior approach using the previous surgical scar. Inspection revealed ceramic debris and an eccentrically fractured ceramic liner, accounting for the patient’s symptoms (Fig 2a and b). Thorough debridement of ceramic fragments from the surrounding soft tissues was performed with fluoroscopic assistance.
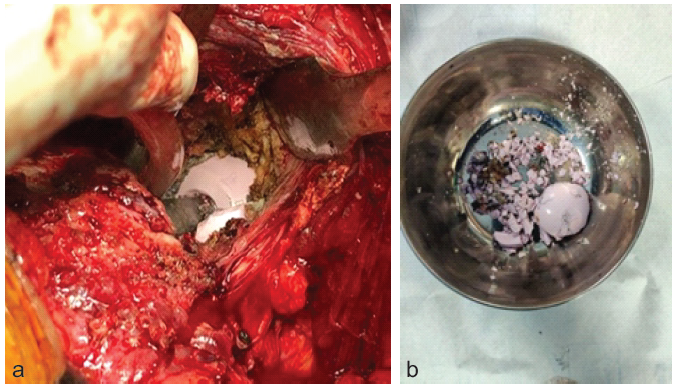
Figure 2: (a) Intraoperative photograph showing an intact ceramic femoral head in situ with surrounding ceramic fragments. (b) Retrieved ceramic liner fragments following revision surgery.
The acetabular shell, femoral stem, and trunnion were intact, stable, and appropriately positioned and were therefore retained. The liner was revised to a highly cross-linked polyethylene liner, and the femoral head, although unfractured, was exchanged for a bigger 36 mm (+12 mm offset) BIOLOX head (DePuy). Stability was confirmed.
Post-operatively, the patient was allowed to bear weight as tolerated with standard hip precautions and a structured rehabilitation protocol. The patient reported complete resolution of pain, squeaking, and crepitus in the post-operative period. 1 year Follow-up radiographs demonstrated a well-aligned and well-fixed implant, with no evidence of osteolysis and no complaints (Fig. 3).
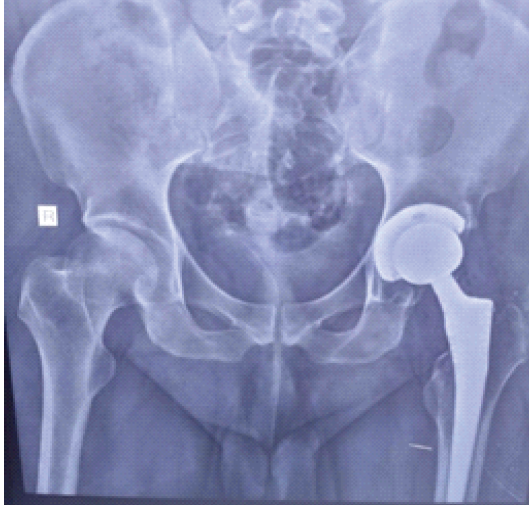
Figure 3: Anteroposterior radiograph of the left hip at 1-year follow-up demonstrating a well-fixed and well-aligned implant.
Despite major advances in ceramic material science, ceramic liner fracture remains a distinct complication of CoC THA. Modern ceramics, particularly zirconia-toughened alumina composites, such as BIOLOX Delta, demonstrate improved fracture toughness, resulting in a dramatic reduction in femoral head fracture rates [1]. Large registry data confirm that head fractures have become exceedingly rare with contemporary ceramics; however, liner fracture rates have not shown a comparable decline, highlighting the importance of mechanical and implant-related factors rather than material properties alone [1].
Ceramic liner fractures are influenced by several patient, implant, and technique-related factors. Malposition of the acetabular component, particularly excessive anteversion or inclination, has been consistently identified as a major risk factor [3]. Traina et al. demonstrated that cups placed outside the optimal anteversion range were significantly more common in patients with liner fractures and that audible noise frequently preceded failure [3]. These findings support the role of neck-cup impingement, microseparation, and edge loading at the liner rim as key mechanisms leading to crack initiation and propagation. Smaller femoral head sizes and higher patient body mass index have also been associated with increased fracture risk, likely due to altered contact mechanics and increased joint reaction forces [1].
Lee et al. recommended the use of acetabular metal shells with an increased inner taper angle of 18°, rather than the conventional 10°, to reduce the risk of ceramic liner malseating [4,5]. They also advocated the use of ceramic femoral heads measuring 32 mm or larger, along with implant neck designs featuring a flatter anteroposterior profile, to minimize impingement and reduce the risk of liner fracture.
The use of metal-backed ceramic liners has been proposed to improve load distribution and protect the ceramic liner during implantation and impingement. However, a metal backing does not eliminate the risk of liner fracture. Case reports have demonstrated that fractures of metal-backed liners may remain non-displaced and radiographically occult, delaying diagnosis while allowing continued generation of ceramic debris [6]. In such cases, the metal shell may temporarily contain ceramic fragments, masking early radiographic signs despite progressive mechanical damage.
Diagnosis of ceramic liner fracture remains challenging. Conventional radiographs may fail to detect non-displaced fractures or small ceramic fragments. CT is valuable for identifying periarticular ceramic debris and subtle liner discontinuity. Toni et al. described an early diagnostic approach incorporating CT evaluation of prosthetic impingement and fluoroscopy-guided joint aspiration for the detection of ceramic particles, allowing diagnosis even when imaging findings are inconclusive [7]. Aspiration with microscopic analysis can confirm the presence of ceramic debris and should be considered when clinical suspicion is high.
Early diagnosis is critical, as delayed recognition of ceramic liner fracture can lead to catastrophic consequences. Continued articulation in the presence of ceramic debris results in severe third-body wear, metallosis, and progressive destruction of surrounding tissues. Reports of delayed diagnosis describe extensive bone loss, pelvic discontinuity, and complex revision surgery with compromised outcomes [8]. These cases emphasize the importance of maintaining a high index of suspicion in patients presenting with new-onset pain, squeaking, or grinding following CoC THA. Equally important is patient education, as persistent or progressive symptoms, such as painful squeaking should not be dismissed or tolerated, and early clinical review may prevent catastrophic failure, as demonstrated in the present case.
The optimal bearing surface at revision following ceramic liner fracture remains debated. Complete removal of ceramic debris is rarely achievable, and retained microscopic fragments pose a risk for accelerated wear. Use of metal-on-polyethylene bearings is generally discouraged due to the susceptibility of metal heads to third-body wear. Ceramic-on-polyethylene and CoC bearings are both considered viable options. Ceramic heads offer superior scratch resistance and reduced vulnerability to ceramic debris, making them preferable when polyethylene liners are selected [4,9,10]. When meticulous debridement is performed, and component positioning is satisfactory, favorable outcomes have been reported with both bearing options.
Ceramic liner fracture remains a rare but clinically significant complication of CoC THA. Although advances in ceramic materials have substantially reduced femoral head fracture rates, liner fractures persist due to mechanical factors, such as component positioning, impingement, and liner seating. Diagnosis is often difficult and may be delayed due to subtle imaging findings and non-specific symptoms. Early recognition and timely revision are essential to prevent catastrophic third-body wear and extensive tissue damage. Careful selection of revision bearing surfaces, with consideration of retained ceramic debris, is critical for achieving favorable outcomes.
Persistent painful squeaking or grinding following ceramic-on-ceramic total hip arthroplasty should raise suspicion for ceramic liner fracture, even in the absence of trauma or obvious radiographic findings. Prompt identification and intervention are essential to prevent catastrophic failure.
References
- 1. Howard DP, Wall PD, Fernandez MA, Parsons H, Howard PW. Ceramic-on-ceramic bearing fractures in total hip arthroplasty: An analysis of data from the national joint registry. Bone Joint J 2017;99-B:1012-9. [Google Scholar] [PubMed]
- 2. Abdel MP, Heyse TJ, Elpers ME, Mayman DJ, Su EP, Pellicci PM, et al. Ceramic liner fractures presenting as squeaking after primary total hip arthroplasty. J Bone Joint Surg Am 2014;96:27-31. [Google Scholar] [PubMed]
- 3. Traina F, De Fine M, Bordini B, Toni A. Risk factors for ceramic liner fracture after total hip arthroplasty. HIP Int 2012;22:607-14. [Google Scholar] [PubMed]
- 4. Lee YK, Lim JY, Ha YC, Kim TY, Jung WH, Koo KH. Preventing ceramic liner fracture after Delta ceramic-on-ceramic total hip arthroplasty. Arch Orthop Trauma Surg 2021;141:1155-62. [Google Scholar] [PubMed]
- 5. Lee YK, Kim KC, Jo WL, Ha YC, Parvizi J, Koo KH. Effect of inner taper angle of acetabular metal shell on the malseating and dissociation force of ceramic liner. J Arthroplasty 2017;32:1360-2. [Google Scholar] [PubMed]
- 6. Diciurcio W, Lutz RW, Smith EB, Deirmengian GK. Fracture of a metal-backed ceramic liner after total hip arthroplasty: A case report. Cureus 2023;15:e41824. [Google Scholar] [PubMed]
- 7. Toni A, Traina F, Stea S, Sudanese A, Visentin M, Bordini B, et al. Early diagnosis of ceramic liner fracture. Guidelines based on a twelve-year clinical experience. J Bone Joint Surg Am 2006;88 Suppl 4:55-63. [Google Scholar] [PubMed]
- 8. Winston BA, Kagan RP, Huff TW. Delayed diagnosis of catastrophic ceramic liner failure with resultant pelvic discontinuity and massive metallosis. Arthroplast Today 2017;3:77-82. [Google Scholar] [PubMed]
- 9. Goretti C, Polidoro F, Paderni S, Belluati A. Ceramic on ceramic total hip arthroplasty and liner fracture. Two case reports and review of literature. Acta Biomed 2019;90 Suppl 12:192-5. [Google Scholar] [PubMed]
- 10. McEntire BJ, Bal BS, Rahaman MN, Chevalier J, Pezzotti G. Ceramics and ceramic coatings in orthopaedics. J European Ceramic Soc2015;35(16):4327-4369. https://doi.org/10.1016/j.jeurceramsoc.2015.07.034 . [Google Scholar] [PubMed] [CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem
July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach