
Anatomical landmarks such as the anterior acetabular notch and transverse acetabular notch can be reliably used to achieve accurate acetabular cup positioning within the safe zone in total hip arthroplasty. This simple and cost-effective technique provides reproducible results with good functional outcomes and may serve as a practical substitute for advanced navigation techniques, particularly in resource-limited settings.
Dr. Avik Kumar Naskar, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. E-mail: avik7933@gmail.com
Abstract
Introduction: Accurate orientation of the acetabular component in total hip arthroplasty (THA) is critical for restoration of hip biomechanics and prevention of complications such as instability, impingement, accelerated wear, and early implant failure. While computer-assisted navigation enhances accuracy, its routine use is limited by cost and availability. Anatomical landmarks, including the anterior acetabular notch (AAN) and transverse acetabular notch (TAN), may provide a reliable intraoperative reference for component positioning. This study evaluates the accuracy of acetabular cup placement using these landmarks with post-operative computed tomography (CT)-based assessment.
Materials and Methods: A prospective observational study was conducted on 53 patients undergoing primary total hip replacement at a tertiary care centre. Acetabular component positioning was guided intraoperatively using AAN for anteversion and TAN for abduction. Post-operative CT scans obtained on day 14 were used to measure cup orientation. Target alignment was defined according to Lewinnek’s safe zone (abduction 40° ± 10°, anteversion 15° ± 10°). Functional outcomes were assessed using the Harris Hip Score (HHS), and patients were followed up clinically and radiologically.
Results: The mean post-operative acetabular cup abduction was 40.13° and anteversion was 16.29°, both within the defined safe zones. The mean HHS improved significantly from 37.42 preoperatively to 85.83 postoperatively, indicating substantial functional recovery. The mean error in cup positioning was markedly reduced post-operatively. No cases of dislocation or major complications were observed during the follow-up period.
Conclusion: Simple anatomical landmarks can reliably guide acetabular cup placement in THA, offering a cost-effective alternative to intraoperative technology-assisted guidance methods like navigation, with comparable clinical outcomes.
Keywords: Arthroplasty, replacement, hip, acetabulum, anteversion.
Total hip arthroplasty (THA) is a highly successful surgical procedure for relieving pain and restoring function in patients with various hip pathologies. Despite advancements in implant design and surgical techniques, accurate positioning of the acetabular component remains a critical determinant of long-term outcomes. Malpositioning the acetabular cup can lead to complications such as instability, impingement, increased polyethylene wear, reduced range of motion (ROM), and early implant failure [1,2]. Optimal orientation of the acetabular component is typically described in terms of abduction and anteversion. Lewinnek et al. proposed a “safe zone” of 40° ± 10° for abduction and 15° ± 10° for anteversion to reduce the risk of dislocation [1]. However, achieving this orientation consistently remains a challenge in clinical practice. Murray defined three types of anteversion of the acetabular component (anatomical, operative, and radiographic), each of which is measured on different images (computed tomography [CT], intraoperative assessments, and post-operative plain radiographs) [3]. As the anteversion is measured on different axes, depending on the method used, different values can be obtained. Anteversion values vary significantly in serial cross-table lateral views [4]. Measurement of anteversion from the elliptical projection of the acetabular component on anteroposterior radiographs has been introduced in numerous reports. However, anteversion on CT reflects the actual anatomical anteversion, whereas anteversion on plain radiographs represents only the radiographic anteversion. The assessment of the angle of abduction is done with the CT, measuring the angle subtended by the long axis of the cup to the transverse axis of the body, and the anteversion as a measurement of the angle between the axis of the component and the coronal plane of the patient. There are a variety of methods aiding in the acetabular cup placement intraoperatively, such as
- The referencing of the transverse acetabular ligament
- Intraoperative navigation technology
- The bony landmarks of the anterior acetabular notch (AAN) and transverse acetabular notch (TAN).
Various methods have been employed to improve the accuracy of acetabular cup positioning, including mechanical alignment guides, fluoroscopy, computer-assisted navigation, and robotic-assisted systems. While these techniques enhance precision, they are often associated with increased cost, operative time, and limited availability, particularly in resource-constrained settings. Anatomical landmarks such as AAN and TAN provide a simple and reproducible intraoperative reference for cup positioning. These landmarks are easily identifiable and do not require additional equipment or infrastructure (Fig. 1).
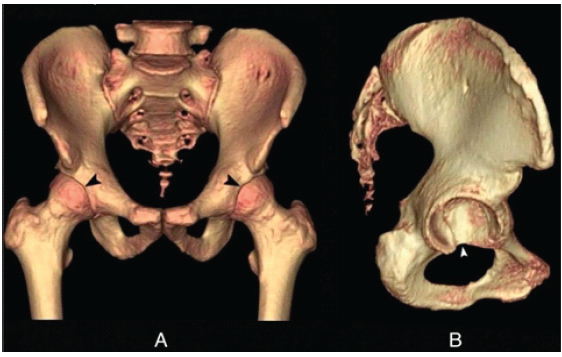
Figure 1: Three-dimensional computed tomographic reconstruction demonstrating key acetabular anatomical landmarks used for cup positioning; (a) Anterior view of the pelvis showing the anterior acetabular notch located at the midpoint of the anterior acetabular rim (black arrowheads). (b) Lateral view of the hemipelvis demonstrating the transverse acetabular notch at the inferior margin of the cotyloid fossa (white arrowhead). These landmarks serve as reliable intraoperative guides for determining acetabular cup orientation in total hip arthroplasty.
While such anatomical landmarks have been widely described for guiding acetabular cup positioning, most studies rely on plain radiographs for assessment, which are limited by projectional errors and variability. To the best of our knowledge, very few prospective studies have evaluated anatomical landmark-based acetabular cup positioning using CT-based three-dimensional validation. This highlights the need for studies that objectively evaluate the accuracy of landmark-based techniques using CT-based measurements. The present study largely addresses this gap in the literature by evaluating the acetabular cup positioning using AAN and TAN as anatomical guides with validation through a postoperative CT scan and assessing the associated functional outcomes.
The study was conducted at the Department of Orthopaedics in a tertiary care facility.
Study population:
A total of 53 male and female patients having avascular necrosis (AVN) of the hip, hip osteoarthritis, fracture of the neck of femur, and non-union of the neck of femur undergoing primary THA between June 2022 and February 2024 were considered eligible and were included in the study.
Study design:
This is a prospective observational study conducted in the Department of Orthopaedics to evaluate the accuracy of acetabular component placement using post-operative CT scan.
Data source:
The study investigated patients who were operated on between June 2022 and February 2024. The Ethics Committee of the Institute approved the study (ethics code: IGGMC/Pharm/BORS/1501–02/2023).
Patient preference:
A convenience sample of 53 patients was included in the study. All patients above the age of 18 years who underwent primary THA between 2022 and 2024 and were willing to participate and provide informed consent were taken into account. Patients with ankylosed hip, developmental dysplasia of the hip, significant acetabular deformity, missed follow-up, and undergoing revision surgery have been excluded from the research.
Data collection:
From the surgical operating data, investigations such as pre- and postoperative imaging and demographic information, including age, gender, body habitus, and prior functional activity, were gathered. A comprehensive clinical examination was done to check for the pre-operative ROM and evaluate the mechanical axis, limb alignment, and neurovascular status of all the patients before consideration for THA. From the CT imaging of the pelvis, AAN was identified at the middle of the anterior rim (in coronal section) and in the vicinity of the anterior pole of the acetabulum (in sagittal view), and TAN was found to be at the lower margin of the cotyloid fossa near the inferior pole (sagittal view) (Fig. 2).
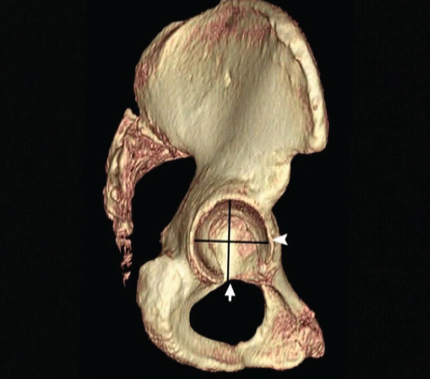
Figure 2: Three-dimensional computed tomographic reconstruction illustrating the spatial relationship of acetabular anatomical landmarks; Lateral view of three-dimensional reconstructed image of the hemipelvis showing the anterior acetabular notch near the anterior pole of the acetabulum (arrowhead) and the transverse acetabular notch near the inferior pole (arrow). These landmarks help define orientation and serve as intraoperative guides for accurate acetabular cup positioning in total hip arthroplasty.
Acetabular abduction was obtained on the mid-coronal image by measuring the angle between a line drawn from the acetabular teardrop to the lateral acetabular margin and the inter-teardrop line. The acetabular anteversion was obtained on the mid-axial image by measuring the angle between a line drawn from the anterior acetabular margin to the posterior acetabular margin and a line perpendicular to the line connecting the centres of both femoral heads (Fig. 3).
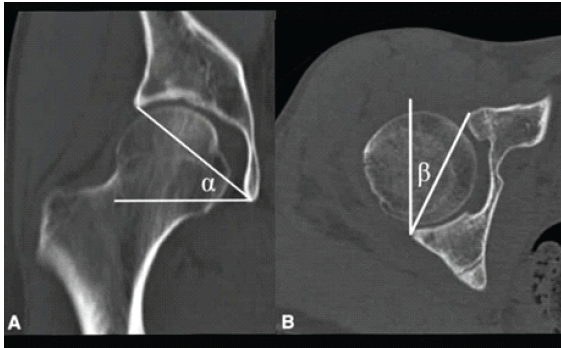
Figure 3: Computed tomography-based measurement of acetabular cup orientation parameters; (a) Mid-coronal computed tomography image demonstrating measurement of acetabular cup abduction (α) using a reference horizontal line. (b) Mid-axial computed tomography image showing measurement of acetabular cup anteversion (β) using standard axial reference lines. These measurements provide an accurate three-dimensional assessment of acetabular component orientation following total hip arthroplasty.
In osteoarthritic hips, the osteophytes are present at the anterior rim of the acetabulum, which obscures the AAN, and the cotyloid fossa is frequently covered by a bony spur, a so-called central osteophyte, which obscures the TAN; hence, the measurement was taken from the true margin of the acetabulum, excluding the osteophytes. The four points to align the cup position at the acetabular rim are the superior and inferior points of 40° abduction and the anterior and posterior points of 15° anteversion. The superior point was the opposite point of the apex of TAN, and the posterior point was the opposite point of the AAN. When the acetabular abduction is >40°, the cup’s inferior point is inside TAN, and when abduction is <40°, it is outside the TAN. When the anteversion is >15°, the cup is aligned with the anterior point outside the AAN, and when the anteversion is <15°, it is inside the AAN. CT scans were obtained again on post-operative day 14 to assess the acetabular component orientation. Cup abduction angle and anteversion angle were noted. Functional outcome was assessed using the Harris Hip score (HHS) preoperatively and at follow-up visits [5].
Surgical technique:
All procedures were performed using the posterior (Moore’s) approach with the patient in the lateral decubitus position [6,7,8]. After exposure, acetabular preparation was carried out using sequential reaming which was directed toward the medial and posterior walls rather than the acetabular roof to avoid translating the centre of rotation superiorly or laterally. Initial reaming was done with a reamer about 9 mm smaller than the templated size. The true floor of the acetabulum was used as the marker for the depth of reaming. Reaming to depth that obliterates this U-shaped portion of the acetabulum (fovea) usually converts the bony acetabulum to a hemisphere. Peripheral reaming was done by larger reamers that were inclined firmly under the superior aspect of the acetabular rim to ream the bone to a hemisphere from its normal sloped anatomy. When reaming the “sloped roof”, the reamer did not engage the superior acetabular rim (because the reamer engaged the more medial roof instead). Once the reamer engaged the superior rim, theoretically, the roof converted into a hemisphere. The reaming was completed when the reamer sat on the superior wall and was stopped 2 mm less than the template size, and then the centre was deepened 2–3 mm so that a larger cup could have a press fit. Trial shells were selected as the same size as the component or that of the reamed size and banged in the direction of the cup placement, and the depth was checked by obliteration of the gap at the slots from the base. Acetabular cup positioning was guided using TAN for abduction and AAN for anteversion with the aim of achieving placement within Lewinnek’s safe zone (Figs. 4 and 5).
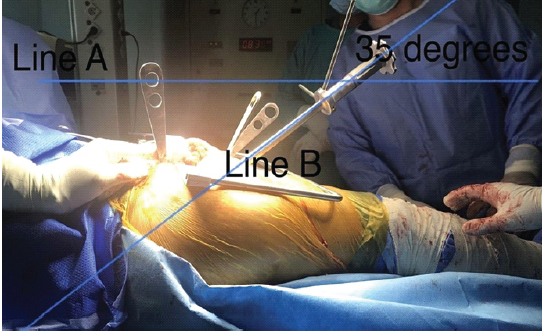
Figure 4: Intraoperative measurement of acetabular cup abduction angle; A horizontal reference line (Line A) is aligned parallel to the floor, while a second line (Line B) is oriented along the acetabular cup insertion handle. The angle formed between Lines A and B represents the acetabular cup abduction angle (35°).
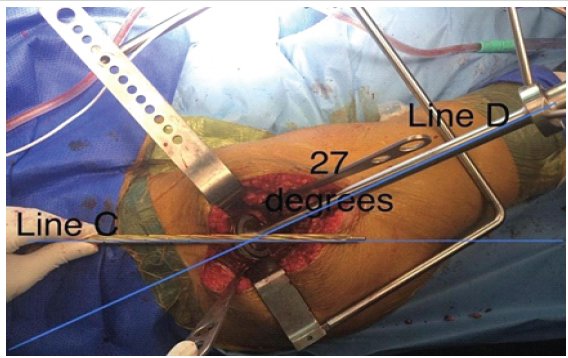
Figure 5: Intraoperative measurement of acetabular cup anteversion angle; The midaxillary line was marked preoperatively on the patient’s torso to represent the coronal plane (Line C) and used as a reference. A second line (Line D) was drawn along the acetabular cup impactor handle. The angle formed between Lines C and D represents the acetabular cup anteversion angle (27°).
Follow-up protocol:
Clinical and radiological follow-ups were done at 6 weeks, 3, 6, 9, and 12 months after surgery and every 6 months thereafter. Cup abduction and anteversion angles were measured using a CT scan after 14 days from surgery (Fig. 6). The functional outcome of the patients was assessed by HHS.
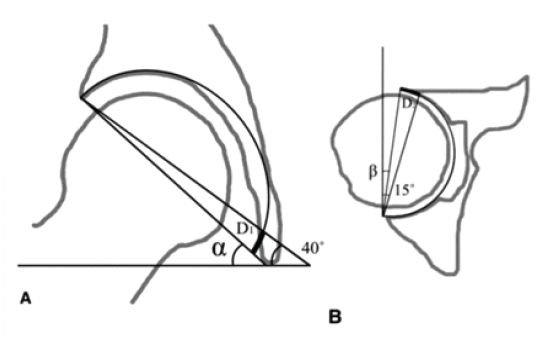
Figure 6: Schematic representation of intraoperative estimation of acetabular cup orientation; (a) Illustration showing calculation of acetabular cup abduction (α) using the transverse acetabular notch as a reference, targeting an inclination of approximately 40°. (b) Illustration demonstrating calculation of acetabular cup anteversion (β) using the anterior acetabular notch as a reference, targeting approximately 15° of anteversion. These reference-based measurements aid in achieving optimal cup orientation within the safe zone during total hip arthroplasty.
Statistical analysis:
Descriptive statistical analysis was performed. Continuous variables were expressed as mean ± standard deviation (SD). Changes in functional scores over time were assessed; however, no comparative statistical inference was intended due to the observational nature of the study.
A total of 53 patients, which included 34 males and 19 females, were included in the study. The mean age of the study population was 45.48 years, with a maximum age of 76 and a minimum age of 22 years. AVN of the hip was the most common indication for surgery.
Radiological outcomes:
The mean post-operative acetabular cup abduction angle was 40.13° (±1.91), and the mean anteversion angle was 16.29° (±2.48). The majority of cases were within the defined safe zone for both parameters. The mean deviation from the target orientation was minimal, indicating a high degree of accuracy in cup placement using anatomical landmarks (Tables 1 and 2).
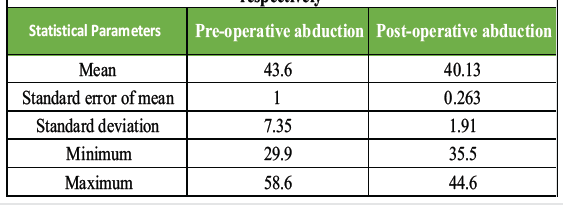
Table 1: Distribution of angle of abduction before and after surgery. The table shows the pre- and post-operative mean angles of abduction along with their standard error, standard deviation, and range (minimum and maximum values). The mean pre- and post-operative angles of abduction were 43.60° and 40.13° respectively
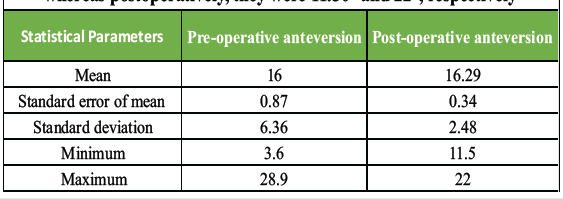
Table 2: Distribution of angle of anteversion before and after surgery; The mean pre-operative anteversion was 16° whereas the mean post-operative anteversion was 16.29°. Preoperatively, the minimum and maximum angles of anteversion were 3.60° and 28.90°, respectively, whereas postoperatively, they were 11.50° and 22°, respectively
Functional outcomes:
The mean pre-operative HHS was 37.42, which improved significantly to 85.83 post-operatively, reflecting substantial functional recovery (Table 3).
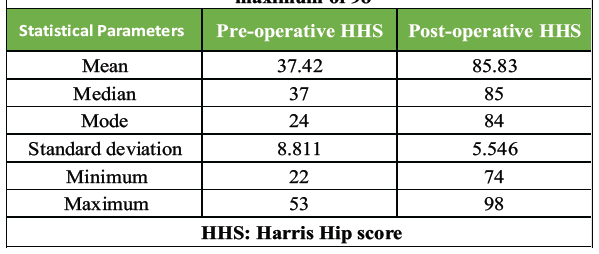
Table 3: Pre-and post-operative distribution of Harris Hip score; The mean pre-operative HHS is 37.42 with the minimum and maximum values being 22 and 53, respectively. Postoperatively, the mean HHS increased to 85.83 with a minimum value of 74 and a maximum of 98
Complications:
No cases of post-operative dislocation or major implant-related complications were observed during the follow-up period.
Among the various techniques for performing THA, the uncemented technique, particularly using the posterior approach, is favoured for its advantages in preserving bone stock, providing better prosthesis fixation through biological ingrowth, and facilitating easier revision surgeries if required [9]. Achieving the correct orientation and alignment of the acetabular component is essential for the longevity of the implant and for minimising post-operative complications. Accurate radiological assessment allows for early detection of potential issues, enabling timely interventions if needed [9]. Studies have shown that optimal placement of the acetabular component is associated with better early functional outcomes, reduced rehabilitation time, and improved overall patient satisfaction [10]. Despite the critical importance of component positioning, there is a lack of comprehensive prospective data that specifically examine the correlation between post-operative radiological findings and early functional outcomes in patients undergoing uncemented THA (Table 4).
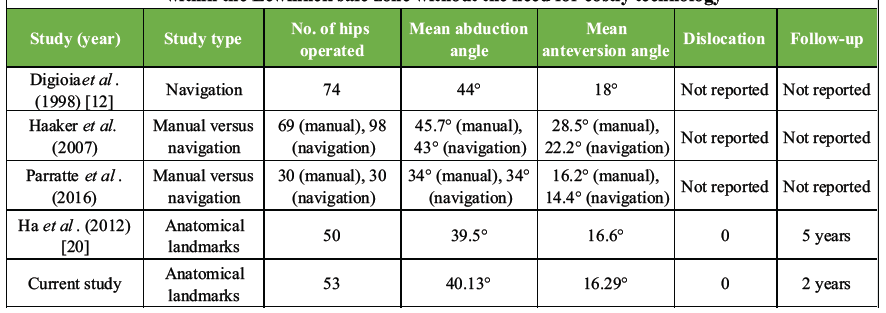
Table 4: Comparison among different studies; The current study was compared with four others in terms of the number of hips operated, mean abduction, and anteversion angles, dislocation rates, and follow-up duration. The outcome was excellent with zero complications and all the acetabular cups were well-aligned within the Lewinnek safe zone without the need for costly technology
This study aims to fill this gap. In this study, the majority of the participants were 40 years old or older, with 73.56% of the sample falling into this category. The mean age of the participants was 45.48 years. The distribution of sex revealed that males constituted a large majority of the sample, accounting for 64.15% of participants, while females represented 35.85%. Saxler et al. in their CT-based study of 105 hips found the mean abduction angle to be 45.8° ± 10.1° and the mean anteversion angle to be 27.3° ± 15° [11]. They only achieved the “safe zone” in 27/105 cups with freehand implantation. The mechanical intraoperative guides used to align the cup with respect to the longitudinal and coronal planes of the patient did not take into account the individual variations in a patient’s anatomy or the change of pelvic orientation during the surgery. Higher rates of inadequate cup orientations outside the desired alignment were observed with mechanical guides. Digioia et al. in their study found that 78% had an unacceptable acetabular alignment and concluded that the mechanical guide was inadequate [12]. This led to various ventures for achieving the optimal anteversion using the anatomical landmarks, among which the study done by Archebold et al. over 1000 hips gave an insight [13]. He proposed a grading system for the transcription activator-like (TAL) and observed that this ligament was identified in only 49% of the hip. The main drawback in this method was that it did not reference the abduction of the cup, so there were chances of the cup being horizontal or vertical, which increased dislocation rates and wear changes. Further, many studies were done supporting the referencing of TAL as a landmark for the acetabular cup position. Pearce et al. concluded that the TAL may be used to align the acetabular cup in THA [14]. Kalteis et al. analysed the acetabular component position relative to TAL using navigation software [15]. Miyoshi et al. also studied the anteversion of the cup relative to TAL [16]. All these studies concluded that the cup anteversion was achieved near the safe zones described, but there was a greater variation in the inclination of the cup. In 2011, Epstein et al. used TAL for cup placement in 64 hips and found that it did not improve on using this ligament as a reference [17]. The first hip navigation system that was developed in 1992 required a pre-operative CT scan and registration of the anatomical and the navigation systems. Extra costs, additional radiation exposure, time-consuming pre-operative planning, and intraoperative matching procedures were a few of its disadvantages. Digioia et al. extensively used image-guided navigation to measure acetabular cup alignment intraoperatively [12]. Leenders et al., in their randomised prospective study, used computer-assisted surgeries to reduce the variability of the cup abduction [18]. With the advent of advancements in technology, the navigation guide was developed, which improved the accuracy of acetabular and femoral component placement and also led to the development of minimally invasive surgeries. However, the navigation technology added to the cost of the surgery and was not feasible in the second and third world countries due to the huge investment involved. This led to the constant search for feasible alternatives as a guide for the cup positioning. Anatomical landmarks were found to be more consistent than the TAL in aiding the cup inclination. Zhang et al., in their 2023 study, determined the orientation of acetabular prostheses in THA by referring to anatomical landmarks of acetabular notches and concluded that those landmarks could help install the cup quickly and safely [19]. Ha et al. in their study of 50 hips found the mean cup abduction to be 39.5° (range 32–47°) and the mean cup anteversion to be 16.6° (range 8–25°) [20]. The mean error of the cup abduction compared with the target abduction of 40° was 1.76° (SD-1.84°; range 0.0–8.4°), and the mean error of the cup anteversion compared with the target anteversion of 15° was 3.47° (SD-2.83°; range 0.1–8.8°). In the scatterplot, cup abduction and anteversion of all 50 hips were within the safe zone with no dislocations. Based on this article, the current study achieved values even closer to the target, signifying the reliability of these anatomical landmarks for acetabular component positioning.
Advantage of the study:
No additional tools like numerical tables or mathematical functions were required, and the study used readily identifiable anatomical landmarks instead of costlier alternatives as an intraoperative guide for cup placement.
Limitations of the study:
The sample size was relatively small, which might limit the generalisability of the findings. The absence of a control group prevents direct comparison with other techniques such as freehand placement or navigation-assisted surgery. The follow-up duration is relatively short, precluding assessment of long-term outcomes such as implant survival and wear.
This prospective observational study highlights the critical relationship between post-operative radiological alignment of the acetabular component and early functional outcomes in patients undergoing uncemented THA. The findings of the study underscore the importance of precise radiological positioning of the acetabular component, particularly regarding cup abduction and anteversion. Proper alignment is crucial for optimising hip biomechanics, ensuring implant stability, and minimising the risk of complications such as dislocation, wear, and loosening. The study demonstrates that accurate positioning of the acetabular component is significantly correlated with improved early functional outcomes, including better pain relief, enhanced hip joint mobility, quicker rehabilitation, and higher levels of patient satisfaction. By providing comprehensive data on the radiological outcomes and their association with early functional recovery, this study contributes valuable insights into the critical factors that influence the success of uncemented THA in a population. The results emphasise the need for meticulous surgical planning, precise intraoperative techniques, and thorough postoperative radiological assessments to achieve the best possible outcomes. Future studies should further explore the long-term impact of component positioning on implant survival and functional performance, as well as the role of advanced imaging techniques and technologies in enhancing the accuracy of component placement. Ultimately, the knowledge gained from this study can help refine surgical practices and improve the overall quality of care for young patients undergoing THA, ensuring better functional outcomes and longer-lasting implants.
Surgeons can achieve safe and consistent acetabular component positioning in routine THA practice by utilising readily identifiable intraoperative acetabular landmarks. CT-based validation supports their accuracy and reliability, making this technique a feasible alternative to costlier technologies like robotics and navigation systems.
References
- 1. Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 1978;60:217-20. [Google Scholar] [PubMed]
- 2. McLaren RH. Prosthetic hip angulation. Radiology 1973;107:705-6. [Google Scholar] [PubMed]
- 3. Murray DW. The definition and measurement of acetabular orientation. J Bone Joint Surg Br 1993;75:228-32. [Google Scholar] [PubMed]
- 4. Nunley RM, Keeney JA, Zhu J, Clohisy JC, Barrack RL. The reliability and variation of acetabular component anteversion measurements from cross-table lateral radiographs. J Arthroplasty 2011;26:84-7. [Google Scholar] [PubMed]
- 5. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. J Bone Joint Surg Am 1969;51:737-55. [Google Scholar] [PubMed]
- 6. Moretti VM, Post ZD. Surgical approaches for total hip arthroplasty. Indian J Orthop 2017;51:368-76. [Google Scholar] [PubMed]
- 7. Von Langenbeck B. On gunshot wounds of the hip joint. Langenbeck’s Archives of Surgery 1874;16:263. [Google Scholar] [PubMed]
- 8. Moore AT. The self-locking metal hip prosthesis. J Bone Joint Surg Am 1957;39-A:811-27. [Google Scholar] [PubMed]
- 9. Widmer KH. A simplified method to determine acetabular cup anteversion from plain radiographs. J Arthroplasty 2004;19:387-90. [Google Scholar] [PubMed]
- 10. Grützner PA, Zheng G, Langlotz U, Von Recum J, Nolte LP, Wentzensen A, et al. C-arm based navigation in total hip arthroplasty-background and clinical experience. Injury 2004;35 Suppl 1:S-A90-5. [Google Scholar] [PubMed]
- 11. Saxler G, Marx A, Vandevelde D, Langlotz U, Tannast M, Wiese M, et al. The accuracy of free-hand cup positioning–a CT based measurement of cup placement in 105 total hip arthroplasties. Int Orthop 2004;28:198-201. [Google Scholar] [PubMed]
- 12. DiGioia AM 3rd., Jaramaz B, Blackwell M, Simon DA, Morgan F, Moody JE, et al. The Otto Aufranc award. Image guided navigation system to measure intraoperatively acetabular implant alignment. Clin Orthop Relat Res 1998;355:8-22. [Google Scholar] [PubMed]
- 13. Archbold HA, Mockford B, Molloy D, McConway J, Ogonda L, Beverland D. The transverse acetabular ligament: An aid to orientation of the acetabular component during primary total hip replacement. J Bone Joint Surg Br 2006;88:883-6. [Google Scholar] [PubMed]
- 14. Pearce CJ, Sexton SA, Davies DC, Khaleel A. The transverse acetabular ligament may be used to align the acetabular cup in total hip arthroplasty. Hip Int 2008;18:7-10. [Google Scholar] [PubMed]
- 15. Kalteis T, Sendtner E, Beverland D, Archbold PA, Hube R, Schuster T, et al. The role of the transverse acetabular ligament for acetabular component orientation in total hip replacement: An analysis of acetabular component position and range of movement using navigation software. J Bone Joint Surg Br 2011;93:1021-6. [Google Scholar] [PubMed]
- 16. Miyoshi H, Mikami H, Oba K. Anteversion of the acetabular component aligned with the transverse acetabular ligament in total hip arthroplasty. J Orthop Sci 2012;17:416-20. [Google Scholar] [PubMed]
- 17. Epstein NJ, Woolson ST. Acetabular component positioning using the transverse acetabular ligament. J Arthroplasty 2011;26:1245-9. [Google Scholar] [PubMed]
- 18. Leenders T, Vandevelde D, Mahieu G, Nuyts R. Reduction in variability of acetabular cup abduction using computer-assisted surgery: A prospective randomized study. J Arthroplasty 2002;17:876-81. [Google Scholar] [PubMed]
- 19. Zhang H, Zhou J, Ling X, Chen H, Du M, Zhao J. Determining the orientation of acetabular prosthesis in total hip arthroplasty by referring to the anatomical landmarks of acetabular notches. Sci Rep 2023;13:6185. [Google Scholar] [PubMed]
- 20. Ha YC, Yoo JJ, Lee YK, Kim JY, Koo KH. Acetabular component positioning using anatomic landmarks of the acetabulum. Clin Orthop Relat Res 2012;470:3515-23. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty July 1, 2025 Metal Mesh Saved The Joint In Primary Hip Arthroplasty In Low Low-Resource Setting
July 1, 2025 Metal Mesh Saved The Joint In Primary Hip Arthroplasty In Low Low-Resource Setting October 1, 2024 Co-existing Ankylosing Spondylitis and Rheumatoid Arthritis in a Patient Undergoing Total Knee Arthroplasty Under Peripheral Nerve Blocks
October 1, 2024 Co-existing Ankylosing Spondylitis and Rheumatoid Arthritis in a Patient Undergoing Total Knee Arthroplasty Under Peripheral Nerve Blocks August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience
August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience