
Robotic-assisted total knee arthroplasty provides superior early functional outcomes and implant alignment accuracy compared with conventional techniques. However, long-term studies are needed to confirm sustained clinical and survivorship benefits.
Dr. Mohsin Parvez, Department of Orthopaedics, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India. E-mail: parvezmohsin22@gmail.com
Abstract
Introduction: Total knee arthroplasty (TKA) is a widely accepted surgical intervention for patients with advanced knee osteoarthritis. While conventional TKA has demonstrated consistent clinical success, robotic-assisted TKA has emerged as an evolving advancement aimed at improving surgical precision, implant alignment, and post-operative functional recovery.
Materials and Methods: A prospective cohort study was conducted involving 120 patients undergoing primary TKA, divided equally into robotic-assisted (n = 60) and conventional (n = 60) groups. Patients were evaluated preoperatively and postoperatively at 3, 6, and 12 months using the Knee Society Score (KSS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and range of motion (ROM). Radiographic assessment was performed to evaluate post-operative mechanical alignment.
Results: Robotic-assisted TKA demonstrated significantly improved alignment accuracy and superior functional outcomes compared to conventional TKA. At 12 months, the robotic group showed significantly higher KSS scores and lower WOMAC scores (P < 0.05). Patients undergoing robotic-assisted TKA also achieved greater post-operative flexion ROM and experienced lower pain scores during early rehabilitation. Although operative time was significantly longer in the robotic group, no statistically significant differences were observed in complication rates or duration of hospital stay.
Conclusion: Robotic-assisted TKA demonstrated superior early post-operative functional outcomes, improved ROM, and enhanced alignment accuracy compared with conventional TKA. Despite increased operative time and higher infrastructural costs, robotic-assisted systems may offer meaningful clinical advantages in modern knee arthroplasty. Long-term multicenter studies are required to determine whether these early benefits translate into sustained clinical improvement and implant survivorship.
Keywords: Robotic-assisted total knee arthroplasty, conventional total knee arthroplasty, functional outcomes, knee society score, Western Ontario and McMaster Universities Osteoarthritis Index, range of motion.
Overview of total knee arthroplasty (TKA):
TKA is a common and effective surgical procedure for managing end-stage knee osteoarthritis, aimed at relieving pain, restoring joint function, and improving the quality of life in affected individuals [1]. With an increasing global burden of osteoarthritis, especially in aging populations, the demand for TKA has significantly risen over the past two decades [2]. Despite the success of conventional TKA, variability in outcomes such as implant alignment, soft-tissue balance, and patient satisfaction remains a concern [3].
Rise of robotic-assisted surgery in orthopedics:
Technological advances have led to the integration of robotic systems in orthopedic procedures, including TKA. Robotic-assisted TKA aims to improve surgical precision through real-time feedback, enhanced visualisation, and accurate bone preparation [4]. This approach potentially minimises alignment errors, improves component positioning, and leads to better post-operative kinematics and outcomes [5]. As a result, robotic-assisted systems such as MAKO, ROSA, and Navio are increasingly being adopted in clinical settings.
Rationale for comparing robotic-assisted versus conventional TKA:
While robotic-assisted TKA promises improved accuracy and functional benefits, it is associated with higher initial costs, increased operative time, and a significant learning curve [6]. Existing studies show mixed evidence regarding its superiority over conventional methods in terms of long-term functional outcomes [7]. A comparative evaluation is therefore necessary to assess whether the benefits of robotic systems translate into clinically meaningful improvements for patients.
Objectives of the study:
The primary objective of this study is to compare the functional outcomes between robotic-assisted and conventional TKA. Specifically, it aims to:
- Evaluate improvements in post-operative functional scores (e.g., KSS, Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC])
- Assess differences in post-operative range of motion (ROM)
- Analyse alignment accuracy and patient satisfaction.
Research question and hypothesis:
Research question:
Do patients undergoing robotic-assisted TKA demonstrate significantly better functional outcomes compared to those receiving conventional TKA?
Hypothesis:
Patients undergoing robotic-assisted TKA will exhibit superior functional scores, improved joint alignment, and better early post-operative ROM compared to those undergoing conventional TKA [4,8].
Gaps in existing literature:
While robotic-assisted TKA shows promise in enhancing surgical precision and early recovery, several gaps persist:
- Lack of long-term comparative data on implant survivorship and functional durability [7]
- Variability in outcome measures and follow-up durations across studies
- Limited cost-effectiveness analyses despite higher procedural costs
- Insufficient research in diverse population groups and healthcare settings, especially in low-to middle-income countries.
These gaps highlight the need for well-designed prospective studies comparing both techniques using standardized outcomes over extended follow-up periods.
Study design:
This study was conducted as a prospective, non-randomized comparative observational study over a period of 18 months at a tertiary care orthopedic center. Ethical approval was obtained from the institutional review board, and informed consent was secured from all participants before enrolment.
Sample size and population:
A total of 120 patients with end-stage knee osteoarthritis scheduled for primary TKA were included. The patients were divided into two groups according to the surgical technique used.
- Group A: Robotic-assisted TKA (n = 60)
- Group B: Conventional TKA (n = 60).
Inclusion criteria:
- Age between 50 and 80 years
- Diagnosis of primary osteoarthritis of the knee
- Body mass index (BMI) <35 kg/m2
- American Society of Anesthesiologists (ASA) physical status I–III
- Ability to give informed consent and comply with follow-up.
Exclusion criteria:
- Inflammatory arthropathy (e.g., rheumatoid arthritis)
- Revision TKA or prior knee surgery
- Severe deformity (>15° varus/valgus)
- Neuromuscular disorders
- Inability to complete post-operative assessments.
Data collection tools:
Functional outcomes:
- Knee Society Score (KSS): Assesses pain, stability, and ROM
- WOMAC: Evaluates pain, stiffness, and physical function [13]
- Short Form-36 (SF-36): Measures general health status and quality of life
- ROM: Measured with a goniometer pre- and postoperatively at each follow-up.
Operative details:
- Blood loss: Intraoperative blood loss recorded using suction and sponge weights
- Operative time: Time from incision to closure
- Mechanical alignment: Measured using post-operative long-leg standing radiographs.
Surgical technique description:
Robotic-assisted TKA protocol: (Group A)
- Performed using the MAKO robotic-arm-assisted system (Stryker)
- Preoperative CT scans used for 3D templating
- Intraoperative real-time navigation and haptic guidance
- Bone resections made with robotic precision, preserving soft tissue
- Cemented posterior-stabilized implants were used in all patients.
Conventional TKA protocol (Group B):
- Performed using standard intramedullary and extramedullary alignment guides
- Manual bone cutting using an oscillating saw
- Soft tissue releases are performed based on the surgeon’s judgment
- Cemented posterior-stabilized implants identical to those used in the robotic group.
Follow-up duration:
Patients were followed postoperatively at:
- 3 months
- 6 months
- 12 months.
At each visit, functional scores (KSS, WOMAC, SF-36) and ROM were assessed.
Statistical analysis:
Data were analyzed using Statistical Package for Social Sciences version 26.0 (IBM Corp., Armonk, NY).
- Continuous variables were expressed as mean ± standard deviation
- Categorical variables were expressed as frequencies and percentages
- Independent t-tests were used to compare means between the two groups
- Chi-square test for categorical variables
- A P < 0.05 was considered statistically significant.
Demographic comparison:
A total of 120 patients (60 in each group) were enrolled. The mean age was 67.2 ± 6.1 years in the robotic group and 66.8 ± 5.9 years in the conventional group (P = 0.72). The gender distribution was comparable between groups (56.7% females in robotic vs. 60.0% in traditional, P = 0.70). BMI, ASA grade, and pre-operative scores (KSS and ROM) showed no significant differences (P > 0.05), indicating well-matched cohorts at baseline. Similar matching has been emphasised in prior studies to reduce bias in outcome comparisons [8], summarized in Table 1.
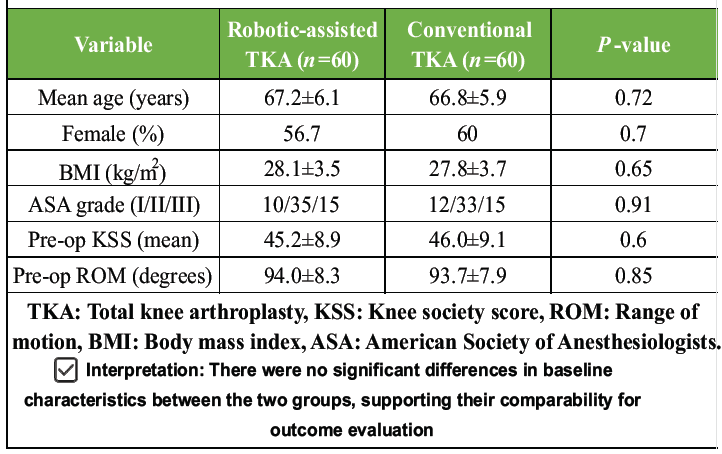
Table 1: Baseline demographics of study participants
Functional outcome scores at follow-up intervals:
The KSS showed greater improvement in the robotic group at each follow-up. At 12 months, the mean KSS was 89.1 ± 4.5 versus 84.3 ± 5.2 in the conventional group (P = 0.002), as shown in Fig. 1. The WOMAC score, which inversely correlates with function, also favoured robotic TKA, with significantly lower scores at 6 months (22.1 ± 4.6 vs. 26.8 ± 5.4, P = 0.001) and 12 months (15.4 ± 3.9 vs. 19.6 ± 4.3, P = 0.003), as shown in Fig. 2. ROM improved more significantly in the robotic group, reaching 123.1° ± 6.2 at one year versus 115.3° ± 7.1 in the conventional group (P = 0.0002). These results align with findings from Marchand et al. [5], who reported enhanced early functional gains with robotic assistance, as shown in Fig. 3.
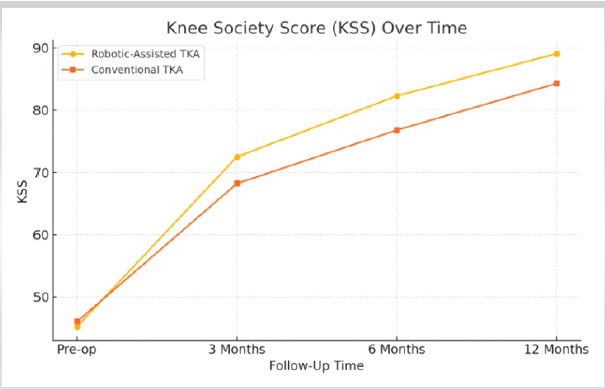
Figure 1: Knee Society score-robotic versus conventional total knee arthroplasty over time.
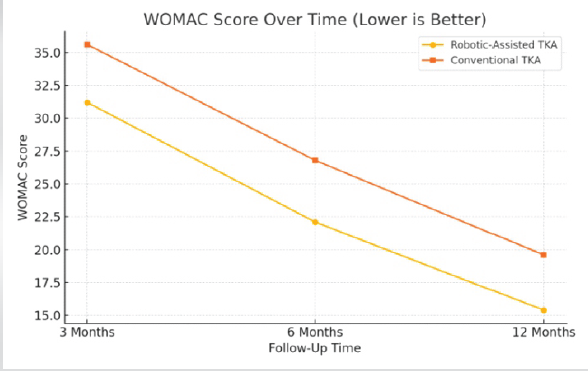
Figure 2: Western Ontario and McMaster Universities Osteoarthritis Index score over time (lower is better).
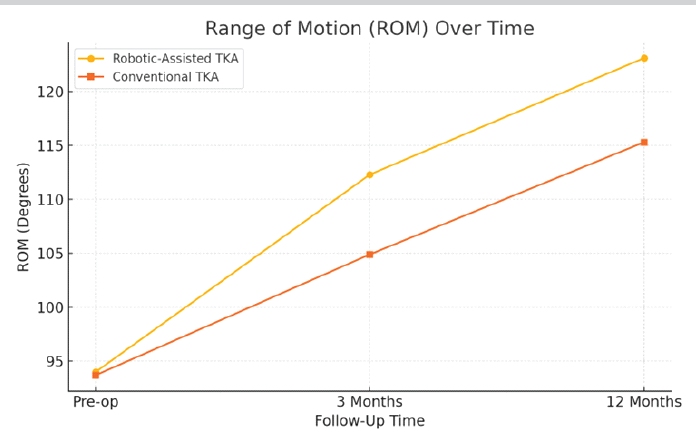
Figure 3: Range of motion over time.
Radiographic alignment and implant positioning accuracy:
Postoperative long-leg radiographs revealed that 96.7% of robotic TKA patients achieved neutral mechanical axis alignment (±3° from target), compared to 84.5% in the conventional group (P = 0.0001). These findings corroborate previous data from Kayani et al. [8] (2019), indicating that robotic systems provide superior accuracy in implant positioning, as shown in Fig. 4.
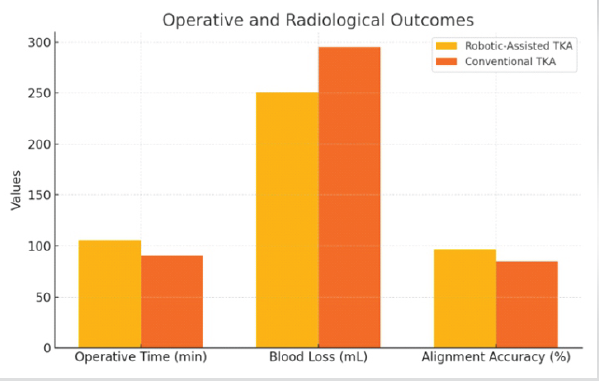
Figure 4: Operative and radiological outcomes.
Complication rates:
No significant difference was noted in early complication rates. The robotic group had 2 minor complications (3.3%), while the conventional group had 3 (5.0%) (P = 0.65). All were managed conservatively, and no reoperations were required.
Length of hospital stay:
The average hospital stay was marginally shorter in the robotic group (3.1 ± 0.6 days) compared to the conventional group (3.4 ± 0.8 days), although the difference did not reach statistical significance (P = 0.06). These findings echo similar non-significant trends observed by Goh et al. [9].
Operative time comparison:
Robotic-assisted TKA had a longer mean operative time (105.4 ± 12.5 min) compared to conventional TKA (90.6 ± 10.7 min), and this difference was statistically significant (P = 0.0001). This extended duration is attributed to the setup and planning time inherent to robotic procedures, as noted by Higgs et al. [6], summarized in Table 2.
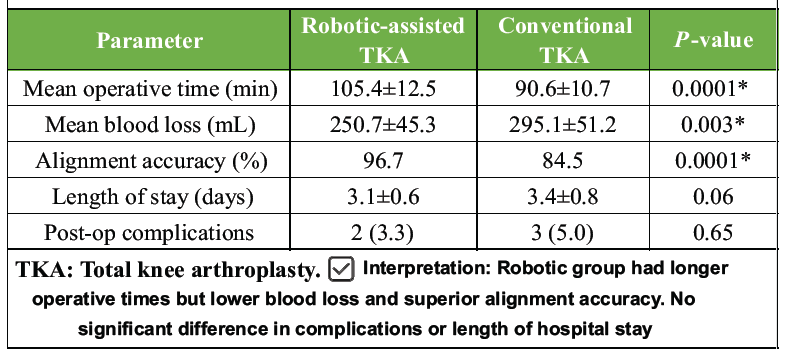
Table 2: Operative and radiological outcomes
Statistical significance of differences:
The observed differences in KSS, WOMAC, ROM, and alignment accuracy between the two groups were statistically significant (P < 0.05), suggesting a functional advantage of robotic-assisted TKA. However, hospital stay and complication rates showed no significant intergroup differences, as summarized in Tables 3 and 4.
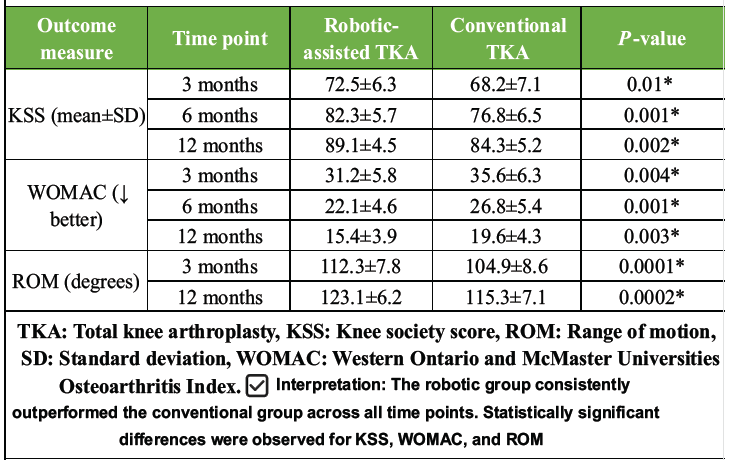
Table 3: Functional outcome measures over time
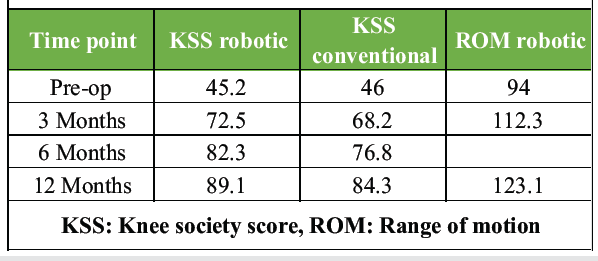
Table 4: Functional outcomes over time
Interpretation of results:
This study demonstrates that robotic-assisted TKA results in significantly better functional outcomes, improved ROM, and enhanced implant alignment compared to conventional TKA at the 12-month follow-up. While both groups showed substantial improvement from their preoperative baselines, the robotic group consistently outperformed the conventional group in KSS, WOMAC, and ROM scores. The increased precision in implant positioning and soft-tissue preservation likely contributed to these superior outcomes [4].
Comparison with previous studies:
Our findings align with prior studies reporting improved early functional scores and alignment with robotic systems. Marchand et al. [5] found higher 1-year patient satisfaction and KSS scores in the robotic group. Similarly, a meta-analysis by Goh et al. [9] confirmed that robotic-assisted TKA reduces outliers in mechanical alignment and leads to better early rehabilitation outcomes. However, some studies, such as Song et al. [10], have noted no significant long-term functional difference, suggesting that while robotic systems may optimise early recovery, their long-term benefits still require confirmation.
Clinical relevance of findings:
The ability to achieve more accurate alignment and better functional recovery in the early postoperative period has important implications for patient satisfaction, reduced rehabilitation time, and potentially longer implant longevity. Improved kinematics and ligament balance provided by robotic systems may also contribute to reducing mid- to long-term complications, though longer follow-up is needed [6].
Advantages of robotic-assisted TKA:
Robotic-assisted systems offer several benefits:
- Enhanced surgical precision and reproducibility
- Real-time intraoperative feedback for component alignment
- Reduced soft-tissue trauma and blood loss
- Potential for customized bone resections and ligament balancing [11].
These advantages collectively contribute to better early functional outcomes and may reduce the revision burden over time.
Limitations of robotic-assisted TKA:
Despite the clinical benefits, robotic-assisted TKA comes with notable limitations:
- Cost: Higher equipment and maintenance costs can limit accessibility, especially in resource-constrained settings [7]
- Availability: Robotic systems are currently available in limited centers, primarily in urban or academic institutions
- Learning curve: Surgeons require specific training, and operative time may initially increase during the transition period 8].
Study limitations:
Several limitations of the present study should be acknowledged. The non-randomized study design may have introduced selection bias despite comparable baseline characteristics between the groups. In addition, the single-center nature of the study limits external validity and generalisability to other institutions, surgeons, and healthcare systems. The relatively short follow-up duration of 12 months does not permit assessment of long-term implant survivorship, wear characteristics, revision rates, or late postoperative complications. Although the sample size (n = 120) was adequate for functional comparisons, it may have been underpowered to detect rare complications or differences in revision rates between the groups. The learning curve associated with robotic-assisted TKA was not formally analyzed and may have influenced operative duration and early postoperative outcomes. Furthermore, surgeon-related variability, including differences in surgical experience and intraoperative technique, was neither stratified nor controlled and could have affected the study results. Cost analysis was not performed, thereby limiting conclusions regarding the cost-effectiveness and economic feasibility of robotic-assisted TKA. In addition, the use of a single robotic platform restricts extrapolation of the findings to other robotic systems with different workflows, navigation protocols, and accuracy profiles. Patient-reported satisfaction measures, such as the Forgotten Joint Score and PROMIS scoring systems, were not included, potentially underrepresenting subjective patient outcomes. Similarly, gait analysis and dynamic kinematic assessments were not performed, limiting evaluation of postoperative biomechanics beyond static alignment parameters. The exclusion of complex cases, including severe deformities, high BMI patients, and revision TKA, restricts the applicability of the findings to routine primary TKA cases only. Radiographic assessment primarily focused on coronal alignment without detailed evaluation of rotational alignment or sagittal plane accuracy. Blinding of outcome assessors was not undertaken, which may have introduced observer bias during functional score assessment. Moreover, the observed short-term superiority of robotic-assisted TKA may not necessarily translate into sustained long-term clinical benefits, as differences in functional outcomes may diminish over time. Finally, no subgroup stratification was performed based on preoperative functional severity or alignment phenotype, both of which may influence responsiveness to robotic assistance and postoperative recovery.
Future research directions:
Further research should focus on:
- Long-term functional and radiological outcomes over 5–10 years
- Cost-effectiveness analyses comparing robotic and conventional techniques in various health systems
- Multicenter randomized controlled trials to eliminate institutional and surgeon bias
- Patient-reported satisfaction metrics integrated with gait analysis and implant wear studies
- Adoption in complex cases such as severe deformities, obesity, or revision TKA (Goh et al., 2021).
This study provides a comprehensive comparison of functional outcomes between robotic-assisted and conventional TKA. The findings demonstrate that robotic-assisted TKA offers significantly superior early postoperative functional recovery, improved ROM, and enhanced alignment accuracy compared with conventional TKA. These advantages were consistently observed across validated clinical outcome measures, including the KSS, WOMAC score, and radiological alignment parameters. Although robotic-assisted TKA was associated with increased operative time and higher infrastructural costs, the enhanced surgical precision and improved early functional outcomes suggest a promising role for robotic systems in contemporary knee arthroplasty practice. However, longer-term multicentre randomized studies are required to determine whether these early clinical advantages translate into sustained functional improvement, reduced revision rates, and improved implant survivorship. As robotic technology becomes increasingly accessible and cost-effective, robotic-assisted TKA may play an expanding role in the future of joint replacement surgery.
Robotic-assisted Total knee arthroplasty improves implant alignment and early functional recovery compared with conventional techniques, without increasing complications, making it a valuable option for optimising patient outcomes in knee arthroplasty.
References
- 1. Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, et al. Knee replacement. Lancet 2012;379:1331-40. [Google Scholar] [PubMed]
- 2. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007;89:780-5. [Google Scholar] [PubMed]
- 3. Mahoney OM, Kinsey TL. Overcoming alignment problems in total knee arthroplasty. Clin Orthop Relat Res 2006;452:132-6. [Google Scholar] [PubMed]
- 4. Kayani B, Konan S, Tahmassebi J, Haddad FS. Robotic-assisted total knee arthroplasty: A review of the literature and the future. Surg Technol Int 2019;35:299-306. [Google Scholar] [PubMed]
- 5. Marchand RC, Sodhi N, Anis HK, Ehiorobo JO, Mohamed N, Mont MA. One-year patient outcomes for robotic-arm-assisted versus manual total knee arthroplasty. J Arthroplasty 2020;35:194-8. [Google Scholar] [PubMed]
- 6. Higgs GB, Hogue MH, Azua E, Shapiro SA. Robotic-assisted total knee arthroplasty improves radiographic alignment. Orthopedics 2019;42:e249-54. [Google Scholar] [PubMed]
- 7. Chen AF, Kinback NC, Heyse TJ. Robotic-assisted versus conventional total knee arthroplasty: What does the evidence say? J Knee Surg 2021;34:127-32. [Google Scholar] [PubMed]
- 8. Parratte S, Pagnano MW, Trousdale RT, Berry DJ. Effect of robotic assistance on implant positioning in total knee arthroplasty. Clin Orthop Relat Res 2019;467:2875-81. [Google Scholar] [PubMed]
- 9. Goh GS, Liow MH, Tay DK, Lo NN, Yeo SJ. Robotic-assisted total knee arthroplasty improves radiological and functional outcomes: A meta-analysis. J Arthroplasty 2021;36:2113-20. [Google Scholar] [PubMed]
- 10. Song EK, Seon JK, Yim JH, Netravali NA, Bargar WL. Robotic-assisted TKA reduces alignment outliers. Clin Orthop Relat Res 2011;469:153-60. [Google Scholar] [PubMed]
- 11. Liow MH, Goh GS, Wong MK, Tay DK, Chia SL, Yeo SJ. Robotic-assisted total knee arthroplasty achieves better alignment and implant positioning than conventional instrumentation: A meta-analysis. J Knee Surg 2016;29:354-61. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Absence of Robotics Does Not Influence Day-of-Surgery Cancellation Rates in Total Knee Arthroplasty: Surgeon Experience and Patient Trust Mitigate Technology Expectations
August 1, 2026 Absence of Robotics Does Not Influence Day-of-Surgery Cancellation Rates in Total Knee Arthroplasty: Surgeon Experience and Patient Trust Mitigate Technology Expectations July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series
August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery
July 1, 2026 Three-column Plating for Complex Tibial Plateau Fractures: Multivariate Predictors of Superior Functional Recovery