
Oestrogen deficiency after menopause contributes to accelerated degeneration of intervertebral discs and spinal structures. Early menopause and prolonged postmenopausal duration should be considered important biological risk factors in lumbar degenerative disease progression.
Dr. Cheemullu Shivashankar Shreyas, Department of Spine, Indian Spinal Injuries Centre, New Delhi, India. E-mail: shreyascheemullu@gmail.com
Abstract
Introduction: Lumbar degenerative disease (LDD) is one of the significant causes of chronic low back pain and disability in postmenopausal women. Although age-related degeneration has been well studied, little has been done to establish how the onset of menopause and duration since menopause affect the rate of lumbar degeneration. Menopause-induced oestrogen deficiency is thought to increase the rate of degenerative alteration in intervertebral discs and vertebral structures that could affect the severity of the disease and clinical outcome.
Purposes: The purpose of the study was to determine the effect of age at menopause and years since menopause on the intensity of LDD and to determine the relationship between clinical manifestations and radiographical evidence in postmenopausal females.
Materials and Methods: The study was a tertiary care center-based, observational cross-sectional study which lasted 12 months at this hospital. There was a total of 50 postmenopausal women aged 45 years or older who presented with persistent low back pain. The participants were divided into the early (<45 years), normal (45–50 years), and late (>50 years) menopause. Clinical evaluation involved the severity of pain based on the Visual Analog Scale and functional limitation. The lumbar spine assessment was conducted and assessed using the standard imaging on radiological assessment, and graded on the degenerative severity. Descriptive and comparative statistical data analysis was done to analyse the data.
Findings: The lumbar degeneration was moderate to severe in 74% of the respondents. The highest level of severe degeneration was observed among the early menopause group (50%), the normal group (23.8%), and the late menopause group (20%). The highest pain scores were seen in women who were early menopausal (6.8 ± 1.4) and progressively with radiological severity. The trend of an increase in degenerative severity was noted with the length of time which passed after menopause. The clinical-radiological correlation was positive, and the higher scores on pain were associated with more advanced degenerative grades.
Conclusion: Earlier menopause and longer postmenopausal years were both positively related to the severity of LDD, the level of pain, and functional impairment. The onset of menopause seems to be a significant biological factor in the development of lumbar degeneration, which is the reason why the history of menopause should be included in the clinical assessment and prevention instead of preventive measures.
Keywords: Disk degeneration, estrogen deficiency, lumbar degenerative disease, low back pain, menopause.
Lumbar degenerative disease (LDD) is the most common cause of chronic low back pain and functional disability, which includes the middle and elderly age groups all over the globe, causing a high burden on quality of life and health care (HDB) [1]. Lumbar degenerative cascade is a multifactorial process that consists of progressive dehydration of the interspinal disc, facet joint arthropathy, hypertrophy of the ligamentum flavum, and osteophyte development, which eventually cause instability of the spine and neural compression [2]. Age is taken to be the most unchanging risk factor in lumbar degeneration, and recently, it has been shaped by growing evidence that biological sex and hormonal conditions are the key factors in regulating the initiation and further developmental degeneration in the spinal changes [3]. Among the women, menopause is a significant physiological shift characterised by a dramatic drop in oestrogen, which has been linked to increased musculoskeletal degeneration (e.g., osteoporosis, sarcopenia, degenerative joint disease) [4]. Oestrogen has been reported to have protective effects on bone metabolism, cartilage integrity, and extracellular matrix homeostasis by regulating collagen synthesis, proteoglycan synthesis, and expression of inflammatory cytokine [5]. As a result of this, postmenopausal oestrogen deficiency could be a predisposing factor of LDD onset and progression in women relative to age-matched premenopausal women and men [6]. A number of studies based on imaging have shown that lumbar disc degeneration, facet joint osteoarthritis, as well as vertebral endplate alterations are more prevalent and severe in postmenopausal women and especially those with early menopause [7]. The intervertebral disc has oestrogen receptors, and experimental studies indicate that a deficiency of oestrogen hastens the apoptosis of disc cells, decreases matrix production, and enhances the disc’s mechanical stress susceptibility, thus enhancing disc degeneration [8]. Furthermore, loss of bone mineral density (BMD) during menopause also changes the microarchitecture of vertebral bodies, and this can influence the transfer of load across the motion segment of the spine and cause even greater degenerative alterations [9]. Natural early menopause or surgical early menopause has been linked with a higher risk of musculoskeletal disorders, and therefore, the time of estrogen deficiency and not the age is the possible reason to determine the extent of degenerative diseases [10]. Regardless of these observations, clinical correlation between age of menopause onset and severity of LDD has not been well investigated, especially in terms of symptom severity, functional disability, as well as radiological grading [11]. The bulk of literature is either heat age spinal degeneration or postmenopausal osteoporosis, and little effort on integrating hormone factor in degenerative spine research is done [12]. Moreover, individual differences in the age of menopause in populations based on genetic, nutritional, and socioeconomic factors might lead to individual differences in lumbar degeneration patterns, which are not entirely portrayed in the existing literature [13]. The role of menopause onset in LDD is of special significance to developing nations where there is poor access to preventive musculoskeletal treatment and delayed diagnosis [14]. To determine the clinical relationship between menopausal status, the length of menopause, and lumbar degenerative changes could assist in the determination of high-risk populations and inform early intervention plans such as hormonal, lifestyle, and rehabilitative interventions. Thus, the study will determine the effect of the menopause onset on the development of LDD in relation to clinical and radiological correlation, to be included in a deeper understanding of the sex-specific and hormonal factors in the spinal degeneration.
Study design:
This study was conducted as a multicentric, hospital-based, observational, cross-sectional clinical correlation study across the Departments of Orthopaedics in collaboration with the Departments of Radiodiagnosis at multiple tertiary care teaching hospitals equipped with advanced imaging facilities. The study protocol was approved by the Institutional Ethics Committees of all participating centres, and written informed consent was obtained from all patients before inclusion in the study.
Study duration:
The study was conducted over a period of 12 months. This duration included patient recruitment, clinical evaluation, radiological assessment, data collection, and statistical analysis.
Participants:
Postmenopausal women presenting with symptoms suggestive of LDD were considered for inclusion in the study.
Inclusion criteria:
- Women with a documented history of natural menopause were included in the study
- Participants were categorized based on age at menopause into three groups: Early menopause (<45 years), normal menopause (45–50 years), and late menopause (>50 years)
- History of chronic low back pain for more than 3 months
- Radiological evidence of lumbar degenerative changes on imaging
- Willingness to participate and provide written informed consent.
Exclusion criteria:
- History of surgical menopause (hysterectomy with bilateral oophorectomy)
- Known inflammatory spinal disorders, such as ankylosing spondylitis
- History of spinal trauma, infection, or malignancy
- Congenital spinal deformities
- Long-term steroid therapy or known metabolic bone disorders other than age-related osteoporosis
- Previous lumbar spine surgery.
Study sampling:
A purposive sampling method was used. All eligible patients meeting the inclusion criteria and attending the outpatient department during the study period were consecutively enrolled until the desired sample size was achieved. This method ensured adequate representation of postmenopausal women with varying ages of menopause onset.
Study sample size:
The sample size was calculated using prevalence-based estimation for observational studies, considering a 95% confidence interval and allowable error within the feasible recruitment period. Based on the expected patient inflow and eligibility criteria, a final sample size of 50 participants was included to assess the association between menopause onset and LDD severity.
Study parameters:
The following parameters were assessed:
- Demographic variables: Age, body mass index, occupation
- Menopausal variables: Age at menopause, duration since menopause
- Clinical parameters: Severity of low back pain using visual analogue scale (VAS), duration of symptoms, presence of radicular pain, functional limitation
- Radiological parameters: Degree of lumbar disc degeneration, disc space narrowing, osteophyte formation, facet joint arthropathy, and overall lumbar degenerative grading.
Study procedure:
The eligible patients were determined in the course of the normal outpatient visits. A comprehensive history was obtained with particular attention paid to menopausal history and menopause duration after the informed consent was obtained. Clinical evaluation of the lumbar spine was carried out a clinical observation of spinal tenderness, range of motion, neurological condition, and evidence of nerve root affection. Radiological examination was performed with the help of plain radiographs of the lumbosacral spine in the anteroposterior and lateral position. The magnetic resonance imaging (MRI) results were checked to determine the degeneration of the disk and the compression of the neural, as shown when it was available and clinically necessary. The assessment of radiological findings was based on standard degenerative scoring systems.
Study data collection:
Data were collected using a predesigned and pretested structured pro forma. Clinical findings, menopausal details, pain scores, and radiological grades were systematically recorded. All data were anonymized to maintain confidentiality. Radiological assessments were independently reviewed to minimise observer bias.
Data analysis:
The data collected were put in a Microsoft Excel spreadsheet and calculated with the help of the right statistical software. Continuous variables were represented by a mean and standard deviation, and the categorical variables were represented by frequencies and percentages. The entries were compared to each other using the right statistical tests (Chi-square test, used with categorical variables, analysis of variance or t-test, used with continuous variables). P < 0.05 was regarded to be statistically significant. Association between menopause onset, duration since menopause, and severity of LDD was further analyzed using odds ratio (OR) with 95% confidence intervals. Adjusted ORs were calculated using multivariable logistic regression analysis after controlling for potential confounding variables such as age and body mass index.
Ethical considerations:
The study was conducted after obtaining approval from the Institutional Ethics Committee. Written informed consent was obtained from all participants before enrollment. Confidentiality of patient information was strictly maintained throughout the study. No additional financial burden or risk was imposed on participants, and the study adhered to the ethical principles outlined in the Declaration of Helsinki.
Demographic and menopausal characteristics of study participants:
Among the 50 study participants, the majority belonged to the 50–54 years age group (36%), followed by 55–59 years (28%), while 20% were aged 45–49 years and 16% were aged 60 years or above. Regarding menopausal status, normal menopause (45–50 years) was the most commonly observed category, accounting for 42% of participants, followed by late menopause (>50 years) in 30% and early menopause (<45 years) in 28% of cases. With respect to duration since menopause, 40% of women had been postmenopausal for 5–10 years, 36% for more than 10 years, and 24% for <5 years.
Clinical and radiological severity of LDD:
Assessment of clinical severity showed that moderate pain intensity based on the VAS was the most common presentation, observed in 48% of participants, while severe pain was noted in 34% and mild pain in 18% of cases. Radiological evaluation demonstrated moderate lumbar degenerative changes in 44% of women, followed by severe degeneration in 30% and mild degeneration in 26% of participants. Similarly, functional limitation was predominantly moderate in severity, affecting 42% of patients, whereas 30% had mild limitation and 28% experienced severe functional impairment. These findings indicate that the majority of postmenopausal women in the study had moderate to severe clinical and radiological manifestations of LDD.
Age at menopause versus radiological severity of lumbar degeneration:
Women with early menopause had the highest proportion of severe lumbar degeneration (50%), indicating a strong association between earlier oestrogen deficiency and accelerated spinal degeneration compared with normal and late menopause groups (Table 1 and Fig. 1). Women with early menopause demonstrated higher odds of severe lumbar degeneration compared to women with normal/late menopause. After adjustment for confounding variables, early menopause remained independently associated with severe degenerative changes.
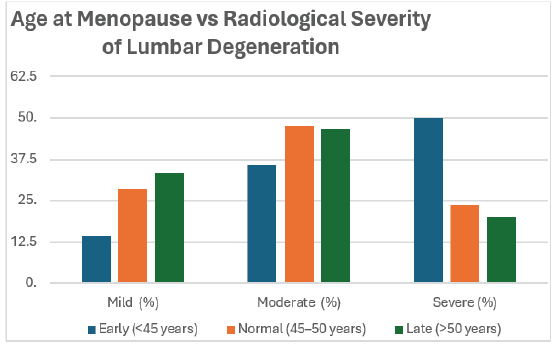
Figure 1: Age at menopause versus radiological severity of lumbar degeneration.
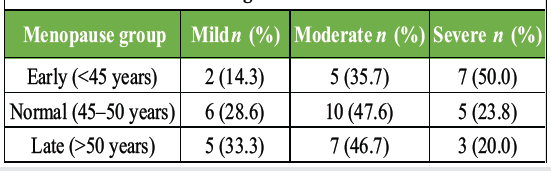
Table 1: Age at menopause versus radiological severity of lumbar degeneration
Duration since menopause versus radiological severity:
An increasing trend of moderate and severe degeneration was observed with longer duration since menopause, suggesting the cumulative impact of prolonged estrogen deficiency on spinal structural degeneration (Table 2 and Fig. 2).
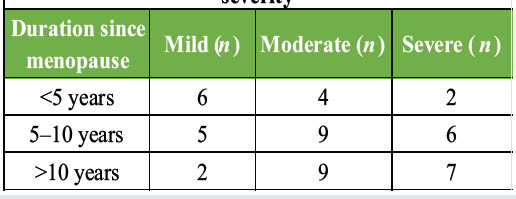
Table 2: Duration since menopause versus radiological severity
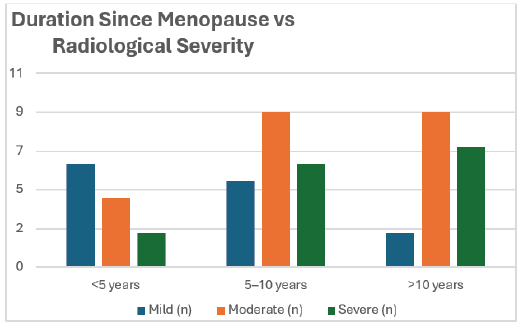
Figure 2: Duration since menopause versus radiological severity.
The current clinical correlation study has assessed the effect of onset of menopause on the LDD progression and has shown that earlier onset of menopause and longer postmenopause period were correlated with higher radiological severity, higher pain scale, and higher functional limitation, and indicated the similar effect of hormonal factors with chronological aging. In the study population of 50 postmenopausal women, early menopause was noted in 28% of the population, and this cohort had the highest percentage of severe degeneration of the lumbar joints (50%), in comparison to 23.8% in the normal menopause cohort and 20% in the late menopause cohort, which indicated a clear gradient of degeneration severity with the age of attaining menopause. These results were also in line with the large MRI-based study of Lou et al. [15]; postmenopausal status was linked to earlier degeneration of lumbar discs even after having age, height, weight, and postmenopausal status as independent variables (P < 0.0001), which was retrospectively examined on 846 postmenopausal women. Lou et al. [15] also demonstrated that there was a significant positive relationship between the years since menopause (YSM) and the extent of degeneration across all lumbar levels with correlation coefficients between r = 0.137 at L5/S1 and r = 0.259 across all lumbar disks, which further supports the current study, that at 2 cases of degeneration was observed in women with <5 YSM, and in women with over 10 YSM, there were 7 cases of degeneration. Notably, Lou et al. reported that this relationship was the highest during the first 15 years of menopause and declined after this, which agrees with the current study that the severity of degenerative changes increased with an increased duration of menopause, indicating that the estrogen deficiency has a greater degenerative effect during the early postmenopausal period. In the present study, there was a high association between pain severity and the onset of menopause and the severity of radiological grade, with the highest VAS scores in the early menopause group (6.8 ± 1.4), followed by a progressive increment in the severity of the degenerated disease (7.1 ± 1.3) as the radiological grade changes. Though the study conducted by Lou et al. [15] was mainly on radiological outcomes and not pain assessment, the structural deterioration they reported is a biological explanation of the increased pain and functional limitation they found in women who had earlier menopause in the present study. The results obtained from Wang et al. [13], who assessed lumbar disc degeneration in elderly men and women, also supported the observed sex- and hormone-related differences in spinal degeneration by showing that the female participants exhibited more severe degeneration of the disc compared to males, even though the ages were evenly distributed. Ageing Wang et al. discovered that lumbar spine BMD and the severity of disc degeneration had a significant association with each other in women but not men, indicating that female-specific factors (e.g., hormonal changes) may alter the disc-to-bone interaction. This finding was an addition to the current study, which showed that women with early menopause were more degenerated and scored higher in pain, which supports the idea that estrogen deficiency is a factor that leads to faster degenerative events. Potential confounding conditions affecting bone metabolism and spinal degeneration were minimised through strict exclusion criteria and detailed clinical history assessment. The influence of the skeletal changes occurring in menopause was further put into context by the landmark study of Elders et al. [16], which showed a significant acceleration of lumbar bone loss over the perimenopausal period and the first 2 postmenopausal years with mean bone loss rates of 6.4% during the perimenopausal period and 5.1% per annum in the first 2 postmenopausal years. Though the study under consideration did not directly estimate the BMD, the radiological severity that was growing with a longer period after menopause among this cohort could partially be explained by the structural effects of such a fast early postmenopausal bone loss, which causes the shift of load transmission through the spinal section of motion and can predispose degeneration of the disc and facet arthropathy. The interplay between disc degeneration and bone metabolism was also explained by Ichchou et al. [17], who stated that the increasing severity of the disc space narrowing in postmenopausal women was correlated with greater spinal BMD and decreased bone resorption, as a negative correlation between C-terminal telopeptide levels and the disc space narrowing was observed, which was adjusted with age and body mass index. These results indicated that degenerative disc disease and osteoporosis can be comorbid with complicated and even contradictory processes. The more prevalent nature of moderate and severe degeneration (74% combined) and the large degree of functional limitation found (70% moderate to severe limitation) in the context of the current study highlighted the clinical relevance of the degenerative changes being experienced, regardless of the underlying bone density changes. In addition, the correlation of the menopause to degenerative alterations in other joints also enhanced the biological likelihood of the current results. It was demonstrated by Lou et al. [18] that the severity of cartilage degeneration in the knee was significantly higher in postmenopausal women compared to pre- and perimenopausal women after the adjustment of age, height, and weight (P < 0.001), and that the severity of cartilage degeneration had a positive association with the number of YSM and the severity of cartilage degeneration across up to 25 years. Although this research centred on the knee joint, nonetheless it provided strong evidence that oestrogen deficiency is involved in the growth of generalised cartilage degeneration in weight-bearing joints, which confirms the current study finding of gradual degeneration of the lumbar joint with the development of menopause. Combined, the similarity in results of the current clinical trial and these large imaging- and BMD-based studies indicated that the effect of menopause and the age of the period of oestrogen deficiency were key factors influencing degenerative musculoskeletal alterations. The increased pain score, radiological severity, and functional impairment in women with early menopause in the current study demonstrated the importance of the issue of menopausal history as a constituent element of clinical evaluation in postmenopausal women presenting with chronic low back pain. The present study specifically evaluated the relationship between menopause onset, duration since menopause, and LDD using combined clinical and radiological assessment, which adds important evidence regarding hormonal influence on spinal degeneration. Inclusion of symptomatic postmenopausal women with categorised menopausal age groups improved clinical relevance. However, the study had certain limitations. The sample size was relatively small, and the cross-sectional design limited the ability to establish causal relationships. BMD, serum oestrogen levels, and detailed biochemical markers were not assessed. In addition, MRI evaluation was not uniformly available for all participants, and residual confounding due to lifestyle or nutritional factors could not be completely excluded.
This paper has reached the conclusion that the initiation and the number of YSM are also important factors in the development of the LDD in postmenopausal women. Early menopause was also accompanied with more radiological severity of lumbar degeneration, more pain, and more functional limitation than normal and late menopause. Over time since menopause, the degenerative changes and the severity of the symptoms were found to increase in a progressive manner, which demonstrates the additive effect of the estrogen deficiency on the spinal structures. The clinical symptoms and radiological findings positive correlation supported the applicability of structural degeneration in the determination of disease burden. This evidence brings out the significance of the inclusion of menopausal history in the clinical evaluation of women with chronic low back pain and the necessity of early intervention and specific preventive measures to reduce the degenerative disease of the lumbar degenerative in high-risk postmenopausal women.
Early onset of menopause and longer duration since menopause are significantly associated with increased severity of LDD in postmenopausal women. Incorporating menopausal history into clinical evaluation may help identify high-risk individuals for early preventive interventions.
References
- 1. Baron YM, Brincat MP, Galea R, Calleja N. Intervertebral disc height in treated and untreated overweight post-menopausal women. Hum Reprod 2005;20:3566-70. [Google Scholar] [PubMed]
- 2. Wang T, Zhang L, Huang C, Cheng AG, Dang GT. Relationship between osteopenia and lumbar intervertebral disc degeneration in ovariectomized rats. Calcified Tissue Int 2004;75:205-13. [Google Scholar] [PubMed]
- 3. Gambacciani M, Pepe A, Cappagli B, Palmieri E, Genazzani AR. The relative contributions of menopause and aging to postmenopausal reduction in intervertebral disk height. Climacteric 2007;10:298-305. [Google Scholar] [PubMed]
- 4. Miyakoshi N, Hongo M, Mizutani Y, Shimada Y. Prevalence of sarcopenia in Japanese women with osteopenia and osteoporosis. J Bone Miner Metab 2013;31:556-61. [Google Scholar] [PubMed]
- 5. Wang YX, Griffith JF, Zeng XJ, Deng M, Kwok AW, Leung JC, et al. Prevalence and sex difference of lumbar disc space narrowing in elderly Chinese men and women: Osteoporotic fractures in men (Hong Kong) and osteoporotic fractures in women (Hong Kong) studies. Arthritis Rheum 2013;65:1004-10. [Google Scholar] [PubMed]
- 6. Kim JY, Chae SU, Kim GD, Cha MS. Changes of paraspinal muscles in postmenopausal osteoporotic spinal compression fractures: Magnetic resonance imaging study. J Bone Metab 2013;20:75-81. [Google Scholar] [PubMed]
- 7. Wang YX, Zhao F, Griffith JF, Mok GS, Leung JC, Ahuja AT, et al. T1rho and T2 relaxation times for lumbar disc degeneration: An in vivo comparative study at 3.0-Tesla MRI. Eur Radiol 2013;23:228-34. [Google Scholar] [PubMed]
- 8. Takatalo J, Karppinen J, Taimela S, Niinimäki J, Laitinen J, Sequeiros RB, et al. Association of abdominal obesity with lumbar disc degeneration–a magnetic resonance imaging study. PLoS One 2013;8:e56244. [Google Scholar] [PubMed]
- 9. Griffith JF, Wang YX, Antonio GE, Choi KC, Yu A, Ahuja AT, et al. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2007;32:E708-12. [Google Scholar] [PubMed]
- 10. Richelson LS, Wahner HW, Melton LJ 3rd., Riggs BL. Relative contributions of aging and estrogen deficiency to postmenopausal bone loss. N Engl J Med 1984;311:1273-5. [Google Scholar] [PubMed]
- 11. Wallace JM, Erickson B, Les CM, Orr BG, Banaszak Holl MM. Distribution of type I collagen morphologies in bone: Relation to estrogen depletion. Bone 2010;46:1349-54. [Google Scholar] [PubMed]
- 12. Imada K, Matsui H, Tsuji H. Oophorectomy predisposes to degenerative spondylolisthesis. J Bone Joint Surg Br 1995;77:126-30. [Google Scholar] [PubMed]
- 13. Wang YX, Griffith JF, Ma HT, Kwok AW, Leung JC, Yeung DK, et al. Relationship between gender, bone mineral density, and disc degeneration in the lumbar spine: A study in elderly subjects using an eight-level MRI-based disc degeneration grading system. Osteoporos Int 2011;22:91-6. [Google Scholar] [PubMed]
- 14. Gruber HE, Yamaguchi D, Ingram J, Leslie K, Huang W, Miller TA, et al. Expression and localization of estrogen receptor-beta in annulus cells of the human intervertebral disc and the mitogenic effect of 17-beta-estradiol in vitro. BMC Musculoskelet Disord 2002;3:4. [Google Scholar] [PubMed]
- 15. Lou C, Chen HL, Feng XZ, Xiang GH, Zhu SP, Tian NF, et al. Menopause is associated with lumbar disc degeneration: A review of 4230 intervertebral discs. Climacteric 2014;17:700-4. [Google Scholar] [PubMed]
- 16. Elders PJ, Netelenbos JC, Lips P, Van Ginkel FC, Van Der Stelt PF. Accelerated vertebral bone loss in relation to the menopause: A cross-sectional study on lumbar bone density in 286 women of 46 to 55 years of age. Bone Miner 1988;5:11-9. [Google Scholar] [PubMed]
- 17. Ichchou L, Allali F, Rostom S, Bennani L, Hmamouchi I, Abourazzak FZ, et al. Relationship between spine osteoarthritis, bone mineral density and bone turn over markers in post menopausal women. BMC Women’s Health 2010;10:25. [Google Scholar] [PubMed]
- 18. Lou C, Xiang G, Weng Q, Chen Z, Chen D, Wang Q, et al. Menopause is associated with articular cartilage degeneration: A clinical study of knee joint in 860 women. Menopause 2016;23:1239-46. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Thoracolumbar Fascial Defect in Persistent Low Back Pain After Lumbar Surgery: Ultrasound Findings and Response to Fascial Plane Injection
August 1, 2026 Thoracolumbar Fascial Defect in Persistent Low Back Pain After Lumbar Surgery: Ultrasound Findings and Response to Fascial Plane Injection March 1, 2026 Assessment of Lumbar Foraminal Stenosis: Diagnostic Value and Clinical Correlation: A Systematic Review
March 1, 2026 Assessment of Lumbar Foraminal Stenosis: Diagnostic Value and Clinical Correlation: A Systematic Review January 1, 2026 Surgical Experience in Symptomatic Bertolotti Syndrome: Clinical Follow-up of Three Patients Refractory to Conservative Management
January 1, 2026 Surgical Experience in Symptomatic Bertolotti Syndrome: Clinical Follow-up of Three Patients Refractory to Conservative Management November 1, 2025 Correlation between Radiographic Parameters and Lordosis in Patients with Chronic Low Back Pain
November 1, 2025 Correlation between Radiographic Parameters and Lordosis in Patients with Chronic Low Back Pain