
Symptomatic os vesalianum pedis is a rare, painful condition that should be considered in the differential diagnosis of persistent lateral foot pain in adolescents, as recognition can guide appropriate conservative or surgical management.
Dr. Bradley Brickman, Department of Orthopaedic Surgery, The University of Toledo Medical Center, Toledo, Ohio, USA. E-mail: bradley.brickman@utoledo.edu
Abstract
Introduction: Os vesalianum pedis (OV) is a rare accessory ossicle located posterior to the proximal base of the fifth metatarsal, with an estimated prevalence of 0.6%. It results from the failure of fusion between the secondary ossification site and the primary ossification center. Most cases are asymptomatic and identified incidentally, but symptomatic presentations can occur following acute trauma or repetitive stress. Reported adolescent cases are limited, with prior literature documenting ages 13–19. We present the youngest reported case of a skeletally immature symptomatic OV in our findings of the English literature – a 12-year-old female – managed successfully with surgical excision and peroneus brevis tendon repair.
Case Report: A healthy 12-year-old female developed acute lateral left foot pain after striking her foot against a table. Urgent care radiographs suggested a non-displaced pseudo-Jones fracture. She was initially managed conservatively, being placed in a controlled ankle motion boot. At 4 weeks, persistent pain and absent callus formation prompted contralateral foot radiographs, revealing a similar ossicle. Magnetic resonance imaging (MRI) confirmed bilateral OV with peroneus brevis attachment, with the left side symptomatic. After 6 weeks of activity restriction failed to improve symptoms, surgical excision of the ossicle with tendon reattachment was performed. Postoperatively, she progressed from short-leg casting to gradual weight bearing in a boot, then returned to regular footwear. At final follow-up, she had full, pain-free function with normal gait, strength, and range of motion.
Conclusion: This case highlights symptomatic OV as a rare but important differential diagnosis for persistent lateral foot pain in adolescent patients, particularly when presumed fifth metatarsal fractures show no healing by 4–6 weeks. Contralateral radiographs and MRI can help differentiate OV from fractures and guide management. While most cases are treated conservatively, surgical excision with tendon repair can yield excellent short-term outcomes when non-operative measures fail. Given the scarcity of skeletally immature cases and unknown long-term implications for tendon integrity and growth plate behaviour, further study is warranted to inform age-specific treatment guidelines.
Keywords: Os vesalianum pedis, accessory ossicle, fifth metatarsal, adolescent foot pain, peroneus brevis tendon, surgical excision.
With an estimated prevalence of 0.6%, os vesalianum pedis (OV) is a rare developmental variant of the foot that presents as an accessory ossicle located just posterior to the proximal base of the fifth metatarsal [1]. It is thought to result from the failure of the secondary ossification site to fuse with the primary ossification center of the fifth metatarsal during development [2]. Although most cases of OV are asymptomatic and typically identified incidentally on plain radiographs of the fifth metatarsal, OV can rarely present symptomatically, often with lateral foot pain following acute trauma or repetitive stress from overuse [3,4,5,6,7]. Upon failure of conservative care, surgical excision of the ossicle followed by reattachment of the peroneus brevis tendon is a surgical option that has previously been employed with success in adult cases of symptomatic OV. To the best of our knowledge, the age range of previously documented adolescent cases spans from 13 to 19 years of age [6,8,9,10,11]. Thus, with this report, we aim to present the youngest reported case in the English literature of a symptomatic OV in a 12-year-old patient following acute foot trauma, in addition to the outcomes of its surgical management.
A 12-year-old female with a past orthopaedic history of clavicle fracture and mild scoliosis presented with acute left foot pain following a minor traumatic event. She was swinging her leg with sudden excitement and struck it against a table. She initially sought care at an urgent care clinic, where plain radiographs of the foot were interpreted as a non-displaced base of the fifth metatarsal fracture, consistent with a pseudo-Jones fracture (Fig. 1a, b, c).
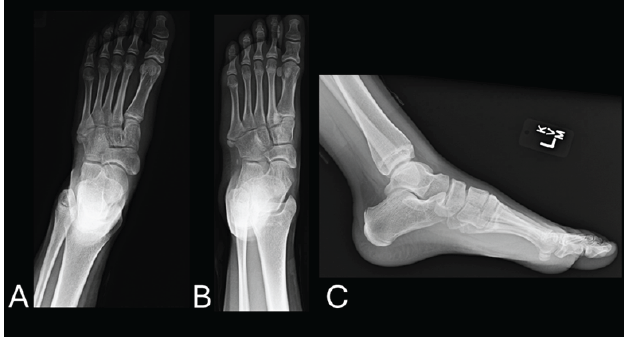
Figure 1: (a, b, c) initial anteroposterior, oblique, and lateral radiographs of the left foot showing an abnormality at the base of the fifth metatarsal.
She was placed in a controlled ankle motion (CAM) boot, made non-weight-bearing (NWB), and advised to follow up with paediatric orthopaedics. At her initial orthopaedic evaluation, 5 days later, she reported sharp localised pain to the lateral aspect of the left foot. On examination, she had point tenderness at the base of the fifth metatarsal, with an otherwise normal musculoskeletal and neurovascular examination. She was placed back into a CAM boot with instructions for weight-bearing as tolerated (WBAT) and scheduled for follow-up. At 4 weeks, the patient reported functional improvement and no longer required analgesics, although she still endorsed pain. Repeat radiographs, however, did not demonstrate expected callus formation (Fig. 2a, b, c).
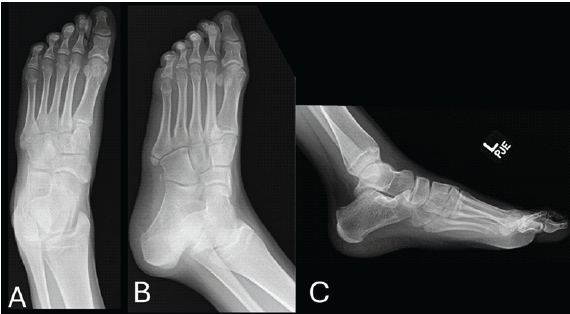
Figure 2: (a, b, c) Left foot anteroposterior, oblique, and lateral radiographs at 4 weeks, without callus formation.
Contralateral foot imaging revealed a similar ossicle, raising suspicion for bilateral OV (Fig. 3a, b, c).

Figure 3: (a, b, c) Contralateral right foot anteroposterior, oblique, and lateral radiographs demonstrating a similar ossicle.
Given persistent symptoms, magnetic resonance imaging (MRI) was obtained, which confirmed the presence of a symptomatic OV with peroneus brevis tendon attachment (Fig. 4a, b, d).
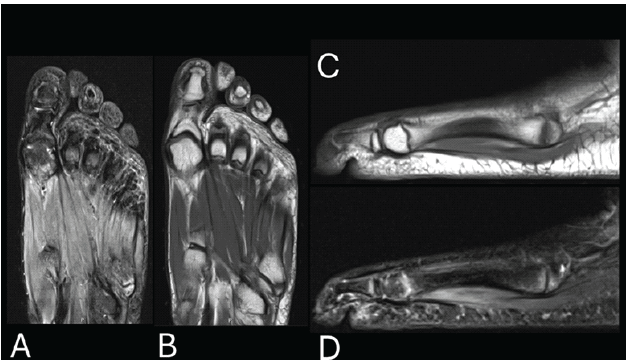
Figure 4: (a and b) Coronal magnetic resonance imaging of the left foot (short tau inversion recovery [STIR], T1) showing increased signal and marrow edema at the fifth metatarsal base. (c and d) Sagittal magnetic resonance imaging (STIR, T1) redemonstrating edema.
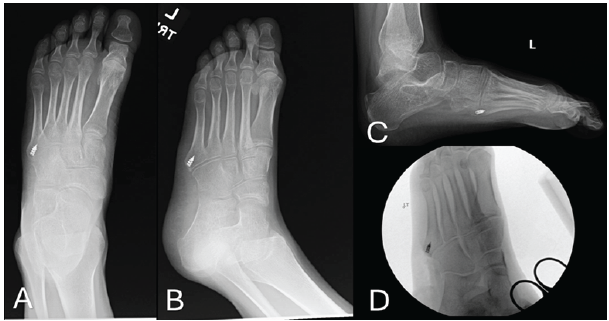
Figure 5: (a, b, c) Left foot anteroposterior, oblique, and lateral radiographs 6 weeks post-excision of os vesalianum pedis with peroneus brevis reattachment. (d) Intraoperative fluoroscopy confirms excision and tendon repair with a suture anchor.
She progressively weaned off crutches and returned to regular footwear. Her recovery was briefly interrupted by two minor injuries: two ankle inversion injuries, one while not wearing the boot, and another misstep leading to transient lateral ankle pain. Neither incident resulted in new radiographic findings. She was managed conservatively with a CAM boot and referred for physical therapy. At her 3-month follow-up, she reported a full return to baseline function without pain, ambulating with a non-antalgic gait and demonstrating full strength and range of motion in the affected extremity (Fig. 6a, b, c). At her final follow-up, 9 months after surgery, she was performing activities as tolerated with no pain, weakness, or other deficits appreciated.

Figure 6: (a, b, c) Left foot anteroposterior, oblique, and lateral radiographs 3 months postoperatively showing interval healing after excision and tendon repair.
In cases of extra accessory ossicles, OV is documented as a relatively rare developmental variant across the United States, Europe, and Asia [1]. While it is common for OV to present asymptomatically, it is hypothesised that trauma may disrupt the synchondrosis of the ossicle and the fifth metatarsal, leading to abnormal motion at this site [2]. This increased mobility could potentially allow the accessory ossicle to act as a fragment next to the insertion of the peroneus brevis tendon. As a result, repetitive contact or mechanical trauma of the tendon can occur, potentially producing inflammation and persistent lateral foot pain. Even in cases where a fracture is absent, this pathophysiological mechanism is hypothesised to be possible, with a common theme being increased mobility of the accessory ossicle that insults the peroneus brevis tendon. While a few cases suggest that symptomatic OV may occur without a clear history of acute trauma, most cases in the literature involve direct injury or repetitive microtrauma, especially in physically active individuals, where chronic stress on the lateral foot is common [12]. The first line of treatment for symptomatic OV is usually conservative; however, upon failure of conservative management, surgical excision of the accessory ossicle and repair of the peroneus brevis tendon are often indicated. Another method with reported good outcomes involves fusion of the ossicle to the fifth metatarsal to stabilise the synchondrosis while preserving the native tendon insertion of the peroneus brevis tendon; however, this approach is less commonly reported compared to excision and tendon repair [11]. In general, the prognosis of symptomatic OV in adults is reported to be good, with some cases resolving with conservative management and others reporting return of function after receiving surgical management [3,4,5,6,7,9,10,12]. Nevertheless, since there appear to be limited adolescent cases of symptomatic OV, coming up with an evidence-based treatment plan currently requires extrapolation from adult case reports. In adolescent patients, there is also a special consideration of whether growth plates surrounding the affected area are still open and how this affects treatment planning in skeletally immature patients, as this mechanism is poorly understood. With respect to diagnosis, it is evident in previous reports that symptomatic OV can disguise itself as other pathologies, such as an unfused apophysis and a pseudo-Jones fracture, the latter of which was the initial diagnosis of this case report [4,7]. Notably, our case suggests that when a suspected pseudo-Jones fracture fails to show callus by 4–6 weeks, contralateral radiographs for comparison and MRI of the affected foot can help prevent the mismanagement of symptoms by clarifying whether symptoms are due to a true fracture, an unfused accessory ossicle, or possible tendon trauma. Overall, this adolescent patient’s quick return to pain-free activity following accessory ossicle removal reinforces the idea that excision and tendon repair are a reasonable option after conservative treatment options have been exhausted. Even though this patient sustained two minor inversion injuries during recovery, neither appeared to impair the healing process. Nevertheless, due to the scarcity of adolescent symptomatic OV reports and this case having less than a year of follow-up care, uncertainty exists in terms of predicting long-term tendon and growth plate behaviour, which outlines the need for further research to help guide the development of age-specific treatment guidelines for this rare condition.
Symptomatic OV is a rare condition with scarce adolescent patient reports, such that the treatment choice and implications on long-term tendon and growth plate behaviour are poorly understood. We report the case of a skeletally immature 12-year-old female patient with symptomatic OV to describe the outcomes of accessory ossicle excision and tendon repair treatment, which appeared to be good in 1 year of follow-up care. In cases of no expected callus formation by 4–6 weeks in a suspected pseudo-Jones fracture of the fifth metatarsal, contralateral radiographs for comparison and MRI of the affected foot could potentially help identify symptomatic OV.
Symptomatic os vesalianum pedis is a rare cause of lateral foot pain associated with an extra accessory ossicle behind the fifth metatarsal, often following the onset of acute or chronic injury. Since it is frequently confused with avulsion fractures of the fifth metatarsal, careful clinical and radiographic evaluation is important. Given the limited number of reported adolescent cases, detailed descriptions of diagnosis and treatment outcomes may help guide management in skeletally immature patients.
References
- 1. Osiowski A, Preinl M, Osiowski M, Baran K, Jasiewicz B, Taterra D. The prevalence and clinical considerations of os vesalianum pedis: A meta-analysis. Foot Ankle Surg 2025;31:612-8. [Google Scholar] [PubMed]
- 2. Sarrafian SK. Osteology. Anatomy of the Foot and Ankle. 2nd ed. Philadelphia, PA: Lippincott; 1993. p. 89-112. [Google Scholar] [PubMed]
- 3. Dorrestijn O, Brouwer RW. Bilateral symptomatic os vesalianum pedis: A case report. J Foot Ankle Surg 2011;50:473-5. [Google Scholar] [PubMed]
- 4. Mathew AJ, Hugh C, Nath S, Pillai MG. Red herring in orthopedics: A case report on painful os vesalianum pedis masquerading as an avulsion fracture of 5th metatarsal and review of literature. J Orthop Case Rep 2023;13:74-8. [Google Scholar] [PubMed]
- 5. Petrera M, Dwyer T, Ogilvie-Harris DJ. A rare cause of foot pain with golf swing: Symptomatic os vesalianum pedis-a case report. Sports Health 2013;5:357-9. [Google Scholar] [PubMed]
- 6. Mousafeiris VK, Papaioannou I, Kalyva N, Arachoviti C, Repantis T. Os vesalianum pedis in a young adult: A case report and literature review. Cureus 2021;13:e14896. [Google Scholar] [PubMed]
- 7. Roy Mohan N, Dominic D. Os vesalianum pedis in a professional badminton player: A case report. Cureus 2024;16:e68411. [Google Scholar] [PubMed]
- 8. Kim MH, Kim WH, Kim CG, Kim DW. Os vesalianum pedis detected with bone SPECT/CT. Clin Nucl Med 2014;39:e190-2. [Google Scholar] [PubMed]
- 9. Aykanat F, Vincenten C, Cankus MC, Kose O, Sindel M. Lateral foot pain due to os vesalianum pedis in a young football player; a case report and review of the current literature. Skeletal Radiol 2019;48:1821-8. [Google Scholar] [PubMed]
- 10. Beil FT, Burghardt RD, Strahl A, Ruether W, Niemeier A. Symptomatic os vesalianum a case report and review of the literature. J Am Podiatr Med Assoc 2017;107:162-5. [Google Scholar] [PubMed]
- 11. Inoue T, Yoshimura I, Ogata K, Emoto G. Os vesalianum as a cause of lateral foot pain: A familial case and its treatment. J Pediatr Orthop B 1999;8:56-8. [Google Scholar] [PubMed]
- 12. De Castro Correia M, Rodrigues Lopes T. Knowing your accessory foot ossicles and avoiding misdiagnoses: A case report of painful os vesalianum pedis. Cureus 2022;14:e27380. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Surgical Management of Painful Os Vesalianum: A Case Report and Literature Review
May 1, 2026 Surgical Management of Painful Os Vesalianum: A Case Report and Literature Review July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report
April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report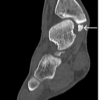 April 1, 2026 Symptomatic Accessory Ossicle Near the Medial Malleolus Simulating Fracture Non-union: A Case Report and Literature Review
April 1, 2026 Symptomatic Accessory Ossicle Near the Medial Malleolus Simulating Fracture Non-union: A Case Report and Literature Review