
The reconstruction of dorsal shear injuries of the hand and wrist presents significant challenges that require a comprehensive understanding and careful multidisciplinary team planning, with the main goal of reconstructing and preserving the prehension and pinch of the hand.
Omar O Al-Hayek, Department of Orthopedic and Spine Surgery, Dr. Soliman Fakeeh Hospital, Fakeeh Care Group, Jeddah, Saudi Arabia. E-mail: hayekou1@yahoo.com
Abstract
Introduction: Dorsal hand shear injuries present complex challenges for surgeons in addressing soft tissue coverage, extensor tendon injuries, and bone loss. This case study examines the inherent challenges associated with the treatment of a severe injury to the dorsum of the hand, as well as the selected treatment approach.
Case Report: A 41-year-old male experienced a severe injury to the dorsum of his left hand following a road traffic accident. The injury involved skin loss from the wrist to the metacarpophalangeal joints, complete loss of the extensor digitorum communis tendons and extensor indicis proprius, significant bone loss in all metacarpal and carpal bones, and instability in the distal radioulnar joint. Multiple debridement and reconstruction surgeries were performed, leading to a satisfactory functional outcome.
Conclusion: There are very few publications addressing complex dorsal hand injuries with follow-up lasting more than 10 years. This article addresses a complex dorsal hand injury and describes steps taken for management with long-term follow-up and acceptable functional outcomes and patient satisfaction. A comprehensive understanding of the pathology and extent of the injury is crucial in developing an effective treatment plan for dorsal hand and wrist shearing injuries. Successful management depends on the knowledge and application of management principles and alternative approaches to address the diverse range of possible injuries involved to restore a functional hand.
Keywords: Dorsal shear, crush hand, hand reconstruction, iliotibial band flap, extensor tendons.
Mangled injury refers to the descriptive characterization of an injury that arises from the act of cutting, tearing, or crushing, leading to the deformation of a limb to the point of being unidentifiable. Typically, a mangled extremity is a consequence of severe trauma and frequently encompasses substantial damage to three or four tissue categories, including bone, skin, artery, and nerve [1]. Of particular significance are traumatic dorsal shearing injuries affecting the hand and wrist, as they present challenges in the context of reconstructing the complex soft tissue and bony structures involved [2]. The detrimental impact of dorsal shearing injuries on hand function is substantial, as they result in extensive damage to the soft tissue envelope, extensor tendon, and underlying bony framework of the hand and wrist. Furthermore, these injuries present distinctive and complex challenges for surgeons responsible for addressing and restoring these impairments. In this case report, we will elucidate a sequential methodology employed for the management of a similar injury, which ultimately yielded a satisfactory long-term functional outcome. We will deliberate upon the inherent challenges associated with treatment, as well as the treatment approach we selected, while also exploring alternative options that were available. Our intention is for this case report to provide valuable guidance for the management of analogous injuries, considering the scarcity of comprehensive literature available to direct the management of intricate dorsal hand and wrist injuries.
A 41-year-old medically free male electrical engineer was referred to our hospital a few days after sustaining a left-hand crush injury. The injury occurred as a result of a motor vehicle accident, whereby the car flipped, and the patient’s left hand became entrapped between the car and the floor. Before being referred from another hospital, the patient had undergone surgical debridement and had two K-wires inserted. At the presentation to our hospital 1 week later, a proper history and examination were done. During the examination, there were evident signs of dorsal shearing injury, as demonstrated in Fig. 1.
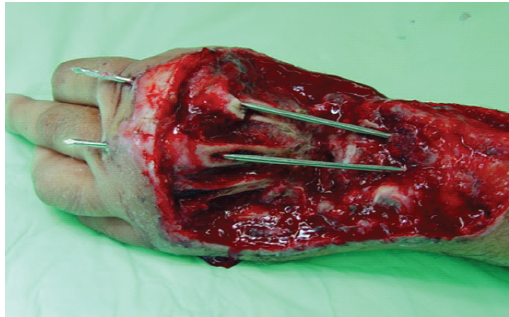 Figure 1: The image illustrates the patient’s initial presentation to our facility following debridement and alignment stabilization using two K-wires. It demonstrates a dorsal shear injury accompanied by skin loss and substantial bone loss.
Figure 1: The image illustrates the patient’s initial presentation to our facility following debridement and alignment stabilization using two K-wires. It demonstrates a dorsal shear injury accompanied by skin loss and substantial bone loss.
The patient exhibited extensive loss of dorsal skin, soft tissue, extensor tendons, muscles, and the dorsal cortex of the carpal and metacarpal bones. Moreover, the injury involved the distal radius and resulted in a significant injury to the distal radioulnar joint. Notably, there were no signs of vascular compromise in the fingers. The patient underwent two instances of local debridement 5 days apart, accompanied by the utilisation of an external fixator to stabilise the affected area and preserve alignment while preserving the length. Fig. 2 exhibits intraoperative and radiographic results following initial surgical interventions.
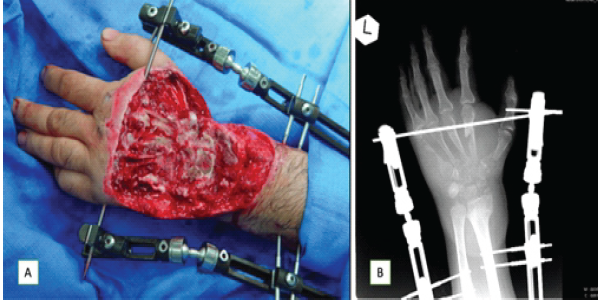
Figure 2: (a) Intraoperative image after debridement showcasing the utilization of external fixation for treatment. (b) Post-operative radiograph demonstrating the condition after the implementation of external fixation, emphasizing the magnitude of bone injuries affecting the metacarpals, carpal bones, ulnar styloid, radial styloid, and distal radioulnar joint.
Subsequent to these surgical procedures, the patient exhibited no signs of either local or systemic infection. After a comprehensive discussion of the patient’s case with the plastic surgery team, a pedicled groin flap procedure was performed. This is illustrated in Fig. 3.
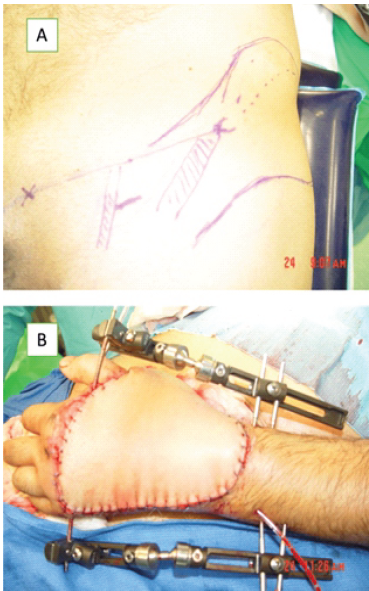
Figure 3: (a) The image depicts the marking performed before the application of a left groin flap. (b) The image illustrates the utilization of a groin flap to provide coverage for the defect.
Following the procedure, a waiting period of 3 months was elected to allow the flap to mature after it was released from the groin. Eventually, the flap has successfully healed. Upon studying the radiographic images from the presentation (Fig. 4), it was observed that there was a complete loss of the carpal bones, as well as the bases and shafts of the metacarpal bones.
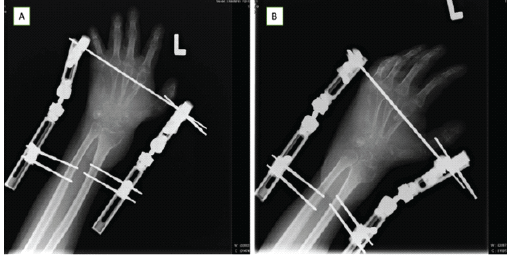
Figure 4: (a) The anteroposterior view captures the assessment of bone defects before the bone reconstruction surgery. Notably, it is observed that the metacarpal heads are preserved, even in the case of complete loss of the fifth metacarpal. (b) Oblique view.
Iliac crest autograft was used as a strut for support as well as to facilitate optimal healing through the presence of cancellous bone. It was harvested as a single piece after removing one cortex. This graft was employed for the reconstruction of the carpal bones and the metacarpals of the three middle fingers. The fixation of the graft in the radius and carpus was achieved using screws. In addition, another piece of the graft was used to reconstruct and bridge the metacarpal of the thumb and was fixed individually with two screws, as depicted in Fig. 5.
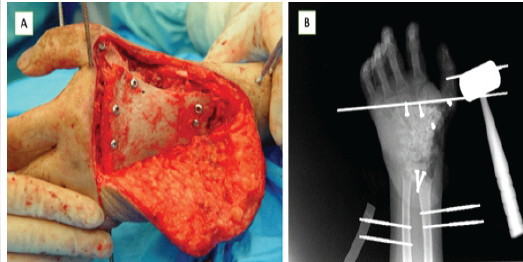
Figure 5: (a) The reconstruction of the carpals and metacarpals involved the utilization of the iliac crest graft, which was securely fixed proximally to the distal radius using screws and distally to the metacarpal head. In addition, a separate piece was employed for the reconstruction of the thumb metacarpal. (b) Following the bone reconstruction procedure, the post-operative radiograph demonstrates the implementation of external fixation to preserve proper alignment while promoting bone healing.
This procedure was done while preserving the initial external fixation in place for extra support and to maintain the wrist in a neutral position. After a period of 3 months, the bone grafts had successfully healed, and the flap remained viable. However, the patient experienced a significant limitation in the functional range of motion manifested mainly as loss of pronation and supination. The subsequent operation involved multiple procedures to address the functional limitations of the wrist and forearm. First, a dorsal corrective osteotomy of the distal radius was performed to establish a functional position for the wrist. This procedure aimed to correct any wrist deformities and align the bones properly. Next, a Sauvé-Kapandji procedure was carried out to improve supination and pronation at the distal forearm. This procedure involved creating a fusion between the distal radius and ulna bones to enhance rotation of the forearm. After that, to reconstruct the fifth metacarpal, a bone graft was taken from the osteotomized ulna. The graft was used to replace the missing bone and restore the stability and structure of the fifth metacarpal. Finally, for the tendon reconstruction, the first stage was done by preparing tunnels for the tendons during this operation. Hemovac tubes were used in place of silastic tubes, which were unavailable at the time. These tunnels were created to guide the tendons during the later stages of tendon reconstruction. Fig. 6 illustrates the post-operative radiographic images.
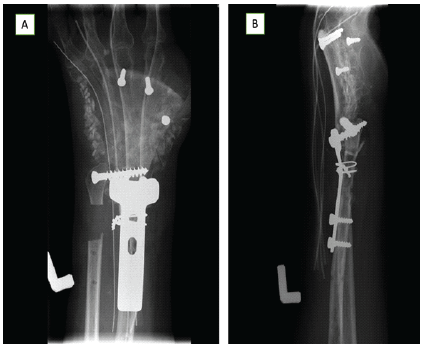
Figure 6: (a) The post-operative anteroposterior view showcases the outcome of a dorsal corrective osteotomy. In addition, a Sauvé-Kapandji procedure was performed. Noteworthy is the utilization of Hemovac tubes during the initial stage of extensor tendon reconstruction. Furthermore, bone chips were employed for the reconstruction of the fifth metacarpal bone. (b) Lateral view.
The subsequent operation involved the second stage of tendon reconstruction, which utilised a tensor fascia lata split graft, and was done 2 months following the first stage. The graft was prepared by dividing it into four bands distally while keeping it as one band proximally. These bands were then fixed through the previously prepared tunnels to complete the tendon reconstruction process. Graft slips were woven distally into the metacarpophalangeal hood or the central extensor tendon distal to the joint. The proximal juncture was carried out using the extensor digitorum communis as a motor. Two months following the successful healing of the tendon and bone grafts, tackling the malalignment of the thumb was warranted. A corrective osteotomy surgery was performed on the thumb metacarpal graft. The objective of this surgery was to reposition the thumb metacarpal graft into an opposition position, enabling improved grip and functionality. The post-operative radiographic images in Fig. 7 display the surgical outcome of the procedure.
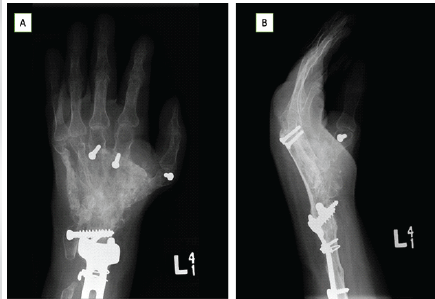
Figure 7: (a) The anteroposterior view captures the outcome following the corrective osteotomy performed on the thumb metacarpal. (b) Lateral view.
The patient demonstrated acceptable long-term functional outcomes after a 1-year follow-up in terms of finger extension and flexion, supination, grip strength, and fine grip, as demonstrated in the findings in Fig. 8.
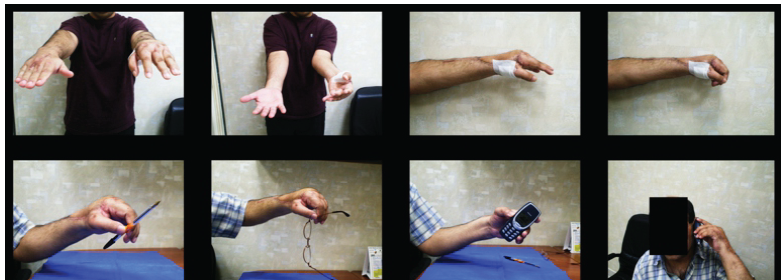
Figure 8: The images depict the functional outcome achieved through the staged reconstruction procedures at 1-year follow-up.
At 20-year follow-up, the patient underwent the Quick Disabilities of Arm, Shoulder, and Hand to assess self-reported functional outcomes. The patient scored 43.42% overall. Fig. 9 shows the results of hand function and range of motion of the patient at 20-year follow-up.

Figure 9: The images depict the functional outcome achieved through the staged reconstruction procedures at 20-year follow-up.
New radiographs shown in Fig. 10 demonstrate bone healing. However, after follow-up, there is still a need for further thumb extension osteotomy.
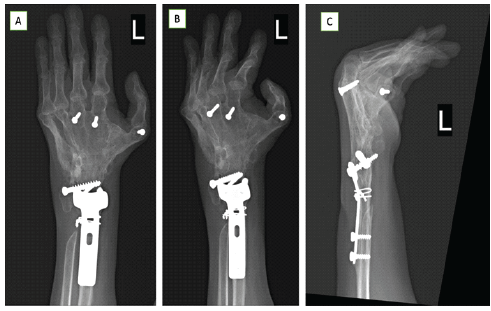
Figure 10: (a) Anteroposterior view 20-year post-operative. (b) Oblique view 20-year post-operative. (c) Lateral view 20-year post-operative.
In our case, the initial step undertaken in the major reconstructive effort was debridement, which is universally recognised as the crucial first step [3]. During each debridement procedure, the surgeon’s primary objective should be the complete removal of all necrotic tissue. It is important to conduct wound debridement and meticulous wound evaluation as soon as possible in the operating room under general anaesthesia. The full extent of the injury zone may not always be apparent during the initial debridement, especially in cases involving degloving, crush, or electrical injuries. The use of larger volumes of irrigation, high-pressure flow, soap solution, and, to a lesser extent, antibiotic solutions, remains critical for effective debridement [4,5,6]. These measures have been shown to effectively remove bacteria, debris, and clots while reducing the risk of wound infection. If complete excision of all necrotic tissue cannot be ensured, it is advisable to postpone reconstruction and plan for a second debridement after 24 h. In our specific case, there was an open fracture with severe comminution and bone loss that precluded internal fixation. The utilisation of external fixation proved to be an excellent method for achieving primary alignment and stability [7]. Care was taken to immobilise only the involved joints while allowing mobilisation of the adjacent joints, resulting in favourable outcomes. In their academic paper, Desai et al. provided a summary of the various approaches for reconstructing complex lesions [8]. They categorised these approaches into three types: Multiple-stage approaches, partially vascularised single-stage approaches, and completely vascularised single-stage approaches. Initially described by Reid in 1974, the multiple-stage approach has traditionally been used to address these injuries, involving the sequential steps of obtaining skin coverage through skin grafts or flaps, performing bony fixation, and subsequently restoring extensor function through tendon grafting or tendon transfer [9]. The latter was the implemented approach in our case. Wound coverage options for the dorsum of the hand and wrist are usually obtained by an immediate local or distant flap for soft tissue reconstruction and summarised by authors Al-Qattan and Sundine and Scheker [10,11]. Local flap options are the distal-based radial or ulnar flap, the reversed posterior interosseous island flap, and the lateral arm flap. Distant flaps include free skin flap, free muscle flap, the temporoprietal free flap, and the pedicled groin flap. In cases requiring both extensor tendon reconstruction and skin coverage in a single stage, composite free flaps provide a favourable vascularised option, with choices including the radial forearm flap (incorporating the palmaris longus or flexor carpi radialis and brachioradialis tendons) [12], the dorsalis pedis flap (incorporating the toe extensors) [13], and thigh flaps (incorporating the fascia lata) [14,15,16]. In cases of multiple-stage reconstruction of the extensor tendon [9] or major defect with the presence of adequate skin and soft tissue coverage [17], the use of silicone rods in tendon graft procedures creates vascularised smooth pseudo-sheaths that facilitate tendon gliding, with the formation of a highly vascularised pseudo-synovial sheath [18]. Hemovac drain tube usage in our case was an alternative. On the second stage, the use of a free tendon graft is commenced and harvested, usually from the palmaris longus, plantaris tendon, or, less commonly, hamstring tendons [19]. Alagoz et al. found in their anatomical study that the plantaris tendon is a preferred choice for longer grafts, whereas the palmaris longus tendon is convenient for thicker grafts, and the tensor fascia lata muscle tendon is suitable when wide or multiple stripes of tendon grafts are desired [20]. Addosooki et al. were the only ones who described the application of a split-free tensor fascia lata graft for the second stage of hand extensor tendon reconstruction [21]. There is a scarcity of documented cases with similar extensive bony and articular injuries as seen in this particular case, which encompassed significant wrist joint instability, loss of carpal bones, and the complete absence of all metacarpals, including the thumb. The management of this case followed certain fundamental principles to achieve the best possible outcome, including ensuring adequate structural support, preserving and maximising the range of motion, and optimising the biological environment. To provide structural support for the wrist and hand, a combination of iliac crest bone reconstruction of the carpal bones and metacarpal bones, along with total wrist arthrodesis, was employed. While the use of a fibular bone graft is more commonly described in the literature for cases involving multiple metacarpal reconstructions, it is typically utilised when the thumb metacarpal and carpal bones remain intact. Preserving the functional position of the wrist and the opposition of the thumb was a priority, achieved by maintaining all metacarpophalangeal joints and enhancing forearm supination and pronation through the addition of the Sauvé-Kapandji procedure. According to Li et al., patients who underwent the Sauvé-Kapandji procedure exhibited improved range of rotation, increased grip power, and fewer degenerative changes compared to those who did not, without risk of wrist instability [22]. To promote healing, autografts were utilised throughout all the procedures, and the preservation of cancellous bone was emphasised. Conversely, the use of allograft reconstruction has been associated with a high incidence of complications, including fractures, non-union, and bony resorption. Allograft fractures are particularly common, with prevalence rates ranging from 5.9% to 26.7% [23]. There are several limitations to our report. First, the extensive number of operations undergone by the patient (11 operations) resulted in increased costs and significant physical strain. It is important to note that many insurance companies may not provide coverage for such procedures. This situation prompts a debate between salvage procedures and amputation, with the latter being the preferred option for the majority of patients. Another limitation is that our report is based on a single case, which restricts generalisability. Therefore, it is recommended to gather more reports and conduct controlled trials to further investigate the reconstruction of complex injuries like this. In addition, biomechanical studies are needed to assess the stability and mobility of using a free split fascia lata graft for multiple extensor tendon reconstruction, as well as the effectiveness of combining the Sauvé-Kapandji procedure with wrist arthrodesis.
The reconstruction of dorsal shear injuries of the hand and wrist presents significant challenges that require a comprehensive understanding and careful planning, particularly when the distal radioulnar joint and the thumb are affected. It is crucial to have a thorough assessment of the current pathology and the extent of the injury to develop an effective treatment plan. The foundation for successful management lies in reconstructing and preserving the prehension and pinch of the hand. Multidisciplinary collaboration is a key factor in achieving successful management outcomes. The combined expertise of multiple disciplines is necessary to address the complexities of these cases. However, it is important to acknowledge that there are certain drawbacks associated with multiple-stage reconstruction, including high costs and prolonged rehabilitation periods.
Dorsal hand shear injuries present complex challenges for surgeons in addressing soft tissue coverage, extensor tendon injuries, and bone loss. A multidisciplinary team approach is necessary to address the complexities of these cases to preserve the prehension and pinch of the hand to achieve acceptable functional outcomes and patient satisfaction.
References
- 1. Gregory RT, Gould RJ, Peclet M, Wagner JS, Gilbert DA, Wheeler JR, et al. The mangled extremity syndrome (M.E.S.): A severity grading system for multisystem injury of the extremity. J Trauma 1985;25:1147-50. [Google Scholar] [PubMed]
- 2. Praveen GM, Adam BS. Microsurgical salvage of complex dorsal shearing injuries of the hand and wrist. Plast Aesthet Res 2020;7:64. [Google Scholar] [PubMed]
- 3. Bakri K, Moran SL. Initial assessment and management of complex forearm defects. Hand Clin 2007;23:255-68. [Google Scholar] [PubMed]
- 4. Anglen JO. Wound irrigation in musculoskeletal injury. J Am Acad Orthop Surg 2001;9:219-26. [Google Scholar] [PubMed]
- 5. Anglen JO. Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds: A prospective, randomized study. J Bone Joint Surg Am 2005;87:1415-22. [Google Scholar] [PubMed]
- 6. Rosenstein BD, Wilson FC, Funderburk CH. The use of bacitracin irrigation to prevent infection in postoperative skeletal wounds. An experimental study. J Bone Joint Surg Am 1989;71:427-30. [Google Scholar] [PubMed]
- 7. Freeland AE. External fixation for skeletal stabilization of severe open fractures of the hand. Clin Orthop Relat Res 1987;214:93-100. [Google Scholar] [PubMed]
- 8. Desai SS, Chuang DC, Levin LS. Microsurgical reconstruction of the extensor system. Hand Clin 1995;11:471-82. [Google Scholar] [PubMed]
- 9. Reid DA. Hand injuries requiring skin replacement and restoration of tendon function. Br J Plast Surg 1974;27:5-18. [Google Scholar] [PubMed]
- 10. Al-Qattan MM. Two-staged extensor tendon reconstruction for zone 6 extensor tendon loss of the fingers: Indications, technique and results. J Hand Surg Eur 2015;40:276-80. [Google Scholar] [PubMed]
- 11. Sundine M, Scheker LR. A comparison of immediate and staged reconstruction of the dorsum of the hand. J Hand Surg Br 1996;21:216-21. [Google Scholar] [PubMed]
- 12. Adani R, Marcoccio I, Tarallo L. Flap coverage of dorsum of hand associated with extensor tendons injuries: A completely vascularized single-stage reconstruction. Microsurgery 2003;23:32-9. [Google Scholar] [PubMed]
- 13. Taylor GI, Townsend P. Composite free flap and tendon transfer: An anatomical study and a clinical technique. Br J Plast Surg 1979;32:170-83. [Google Scholar] [PubMed]
- 14. Talanker MM, Fallah KN, Hartline CA, Freet DJ. One-stage flexor reconstruction with anterolateral thigh and fascia lata rolls after high-voltage trauma: A case report. Eplasty 2023;23:e23. [Google Scholar] [PubMed]
- 15. Suondoh MS, Sulaiman WA, Ismail WF, Saad AZ. One stage microsurgical reconstruction with chimeric flap for salvaging a complex hand injuries. Arch Hand Microsurg 2020;25:156-60. [Google Scholar] [PubMed]
- 16. Sheng H, Tian H, Jing S, Wang Z, Zhang Z, Li D, et al. Clinical application of the free anterolateral thigh myocutaneous flap with the tensor fascia lata for one-stage repair of soft tissues defects at the dorsum of hands (feets). Zhonghua Zheng Xing Wai Ke Za Zhi 2016;32:196-8. [Google Scholar] [PubMed]
- 17. Al-Qattan MM, Al Mohrij SA. A modified technique of two-staged extensor tendon reconstruction in zones 6-8 in a patient with absent palmaris/plantaris tendons: A case report. Int J Surg Case Rep 2019;55:99-102. [Google Scholar] [PubMed]
- 18. Hunter JM, Jaeger SH, Matsui T, Miyaji N. The pseudosynovial sheath–its characteristics in a primate model. J Hand Surg 1983;8:461-70. [Google Scholar] [PubMed]
- 19. Ozbaydar M, Orman O, Ozel O, Altan E. Multiple extensor tendons reconstruction with hamstring tendon grafts and flap coverage for severe dorsal hand injuries. Hand Surg Rehabil 2017;36:410-5. [Google Scholar] [PubMed]
- 20. Alagoz MS, Uysal AC, Tuccar E, Tekdemir I. Morphologic assessment of the tendon graft donor sites: Palmaris longus, plantaris, tensor fascia lata. J Craniofac Surg 2008;19:246-50. [Google Scholar] [PubMed]
- 21. Addosooki A, Said E, Kenawey M, Yousef MA. Reconstruction of complex hand defects using trapezoidal osteocutaneous free fibular flap. Microsurgery 2020;40:306-14. [Google Scholar] [PubMed]
- 22. Li J, Jiao Y, Guo Z, Ji C, Wang Z. Comparison of osteoarticular allograft reconstruction with and without the Sauvé-Kapandji procedure following tumour resection in distal radius. J Plast Reconstr Aesthet Surg 2015;68:995-1002. [Google Scholar] [PubMed]
- 23. Scoccianti G, Campanacci DA, Beltrami G, Caldora P, Capanna R. The use of osteo-articular allografts for reconstruction after resection of the distal radius for tumour. J Bone Joint Surg Br 2010;92-B:1690-4. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2021 Shoulder Lipoblastoma in a 2-Year-Old Boy Case Report and Literature Review
December 10, 2021 Shoulder Lipoblastoma in a 2-Year-Old Boy Case Report and Literature Review May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report
May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report March 10, 2024 Computer Navigation-assisted Bilateral Total Knee Arthroplasty with Osteosynthesis in Single Sitting in Patients Presenting with Distal Femur Fracture with Pre-existing Knee Arthritis: A Case Series
March 10, 2024 Computer Navigation-assisted Bilateral Total Knee Arthroplasty with Osteosynthesis in Single Sitting in Patients Presenting with Distal Femur Fracture with Pre-existing Knee Arthritis: A Case Series May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report
May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report