
Tuberculosis is endemic in India, and osteoarticular TB can have a varied presentation. It is therefore essential to consider it in the differential diagnosis while evaluating a lytic bone lesion. Where possible, all patients should have a biopsy of the lesion and provide a specimen for GeneXpert MTB/RIF to confirm the diagnosis and drug susceptibility testing.
Dr Syeda Saba Khaleel, Department of Orthopaedics, Apollo Institute of Medical Sciences, Hyderabad, Telangana, India. E-mail: sy.saba03@gmail.com
Abstract
Introduction: Tuberculosis (TB) is a major health issue in both developing and developed countries.
Case Report: We present a case of a 37-year-old female who presented to the OP with complaints of pain and swelling in the right forearm for 1 year after sustaining trauma.
Conclusion: TB of the ulna shaft is a rare but significant form of skeletal TB, often overlooked due to its non-specific symptoms and resemblance to other bone infections or tumours.
Keywords: Lytic bone lesion, skeletal tuberculosis, ulna diaphysis.
Tuberculosis (TB) of the bones is a rare and significant form of extrapulmonary TB [1,2], accounting for approximately 1–3% of all TB cases. Among skeletal TB cases, spinal TB is the most common, whereas TB of the ulna shaft is extremely rare [3]. Due to its insidious onset and non-specific clinical presentation, ulna TB is often misdiagnosed as chronic osteomyelitis, bone tumours, or pyogenic infections, leading to delayed treatment and increased morbidity. Minimal initial symptoms, rarity of the lesion, and the ability to mimic more common pathologies account for the delay in diagnosis [4,5].
This is a Caucasian female patient who presented to the orthopaedics outpatient with insidious pain in the right forearm for 1 year. There was a history of trauma 1 year ago. The patient had a history of TB 5 years ago, for which she was treated with anti-tubercular therapy (ATT). There was no history of fever or any other constitutional symptoms.
Findings:
She had swelling of her forearm and was tender over the distal 1/3rd shaft of the ulna. An X-ray (Fig. 1) of the forearm showed a lytic lesion on the distal 1/3 of the ulna. Magnetic resonance imaging of the forearm was done (Figs. 2 & 3), which showed linear T2-weighted short-tau inversion recovery hyperintensity and a T1-weighted isointense lesion measuring 4.5 cm in length noted in the medulla of the distal 1/3 of the ulna, causing a breach in the posterolateral and anteromedial cortex of the ulna and extending into surrounding muscles and soft tissue, showing peripheral enhancement on post-contrast study, suggestive of osteomyelitis.

Figure 1: X-ray forearm showing lytic lesion of the ulna.

Figure 2: Coronal MRI showing a linear hyperintense intramedullary lesion involving Ulna
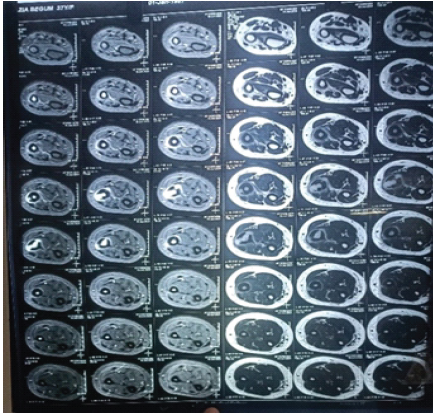
Figure 3: Axial MRI cuts showing cortical disruption and surrounding soft tissue involvement
Procedure:
Aspiration of the cyst produced a small amount of haemorrhagic pus. She was admitted for incision and drainage of the abscess. Incision was given over the dorsal aspect of the swelling. Through the dorso-lateral cortex, debridement (Fig. 4) of the lesion was done till fresh bleeding was seen. Bone graft substitutes (Fig. 5) were used to fill the defect, and plate fixation was done in Stage 2. (Figs 6&7). After confirmation with the patient, The patient was started on ATT based on Mycobacterium tuberculosis culture sensitivity for 9 months (Fig. 6) The latest follow-up was conducted after 1 year; the patient did not exhibit any symptoms of lung disease. There was no apparent pain or discomfort in the limbs, and the swelling of the forearm had disappeared, returning to its normal appearance. X-ray examination revealed a gradual improvement in the ulna (Fig. 8), ultimately returning to its normal long, tubular bone shape without any signs of bone destruction.
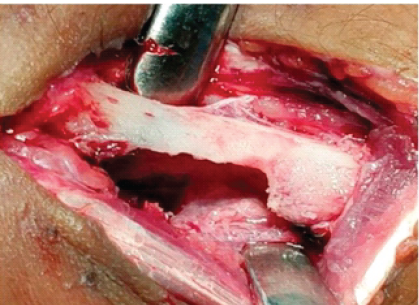
Figure 4: Intraoperative images showing debridement of the lesion.
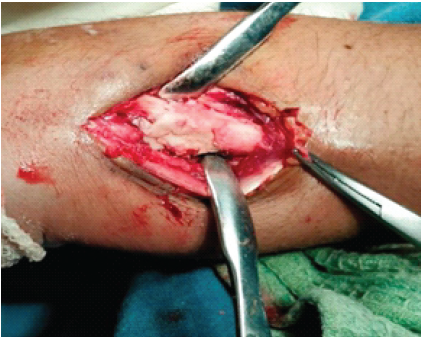
Figure 5: Bone defect filled with polymethyl methacrylate cement.
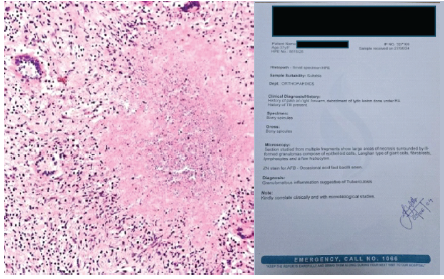
Figure 6: Histopathology findings.

Figure 7: Second stage plate fixation and bone grafting.

Figure 8: Follow-up X-ray at 14 weeks.
TB of the ulna shaft is a rare manifestation of skeletal TB, which itself accounts for only 1–3% of all TB cases. Unlike spinal TB, tubercular osteomyelitis of long bones is uncommon, leading to diagnostic delays due to its non-specific symptoms and radiological findings [6].
Pathophysiology:
TB of the ulna shaft results from haematogenous dissemination from a primary focus, often from pulmonary TB. The slow-growing M. tuberculosis causes granulomatous inflammation, leading to cortical bone destruction, periosteal reaction, and sequestration. This results in progressive pain, swelling, and, in advanced cases, pathological fractures. Patients with ulna TB commonly present with
- Localized swelling and dull pain that worsens over time
- Restricted forearm movement, particularly in advanced cases
- Minimal systemic symptoms (fever, weight loss may be absent)
- Cold abscess formation in chronic cases.
Radiologically:
Osteolytic lesions, cortical thinning, and periosteal reaction mimic chronic osteomyelitis, or pyogenic infections [7]. Thus, a high index of suspicion is required, particularly in endemic regions. TB is known to mimic the symptoms of many other diseases, including various cancers and other infections [5,8].
Diagnostic challenges:
TB of the ulna shaft is difficult to diagnose early due to its rarity and radiological overlap with other bone pathologies. Definitive diagnosis relies on:
- Histopathology – Caseating granulomas [9]
- GeneXpert MTB/Rifampicin (RIF) – Rapid detection of TB DNA and RIF resistance [10]
- Culture on Lowenstein–Jensen medium – Gold standard but slow (4–8 weeks).
Delayed diagnosis can lead to progressive bone destruction, joint involvement, and deformity, making early intervention crucial.
Treatment and prognosis:
The primary treatment for ulna TB is ATT, which should be continued for at least 9–12 months based on response. Medical therapy alone is usually effective in early cases. Surgical intervention (debridement, bone grafting, or stabilisation) is needed in cases with severe bone loss, abscess formation, or pathological fractures. With early diagnosis and appropriate ATT, prognosis is generally good, but delays can lead to deformities and functional impairment. Many reports suggest that debridement alone, without bone grafting, yields favourable outcomes.
Ulna shaft TB is rare but treatable. A high index of suspicion, early diagnosis with molecular tests, and prompt ATT and surgical treatment are essential to prevent complications. In regions where TB is endemic, clinicians should consider skeletal TB in cases of chronic osteolytic lesions to avoid unnecessary delays in treatment.
Always obtain tissue samples for GeneXpert MTB/RIF and culture on Lowenstein–Jensen medium to confirm diagnosis and guide therapy.
References
- 1. Davidson PT, Horowitz I. Skeletal tuberculosis. A review with patient presentations and discussion. Am J Med 1970;48:77-84. [Google Scholar] [PubMed]
- 2. Westall J. Tuberculosis levelling off worldwide. BMJ 1997;314:921. [Google Scholar] [PubMed]
- 3. Burnwal R, Neogi DS, D Ortho SS. Tubercular osteomyelitis of distal ulna presenting as epiphyseal injury. Maedica (Bucur) 2012;7:247-50. [Google Scholar] [PubMed]
- 4. Gyawali B, Sharma BD, Kayastha N, Joshi A. Tuberculosis mimicking a bone tumour. Med J Shree Birendra Hosp 2012;11:49-51. [Google Scholar] [PubMed]
- 5. Sbai MA, Benzarti S, Bouzaidi K, Sbei F, Maalla R. A rare localisation of tuberculosis of the wrist: the scapholunate joint. Int J Mycobacteriol 2015;4:161-4. [Google Scholar] [PubMed]
- 6. Kao HK, Yang WE, Shih HN, Chang CH. Physeal change after tuberculous osteomyelitis of the long bone in children. Chang Gung Med J 2010;33:453-60. [Google Scholar] [PubMed]
- 7. Desimpel J, Posadzy M, Vanhoenacker F. The many faces of osteomyelitis: A pictorial review. J Belgian Soc Radiol 2017;101:24. [Google Scholar] [PubMed]
- 8. Wiratnaya IG, Susila IW, Sindhughosa DA. Tuberculous osteomyelitis mimicking a lytic bone tumor: Report of two cases and literature review. Rev Bras Ortop (Sao Paulo) 2019;54:731-5. [Google Scholar] [PubMed]
- 9. Bickels J, Jelinek JS, Shmookler BM, Neff RS, Malawer MM. Biopsy of musculoskeletal tumours. Current concepts. Clin Orthop Relat Res 1999;368:212-9. [Google Scholar] [PubMed]
- 10. Negi SS, Khan SF, Gupta S, Pasha ST, Khare S, Lal S. Comparison of the conventional diagnostic modalities, bactec culture and polymerase chain reaction test for diagnosis of tuberculosis. Indian J Med Microbiol 2005;23:29-33. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Brown Tumors of Hyperparathyroidism: A 13-Year Retrospective Case Series from a Tertiary Center in South India
April 1, 2026 Brown Tumors of Hyperparathyroidism: A 13-Year Retrospective Case Series from a Tertiary Center in South India March 10, 2024 Unifocal Tubercular Osteomyelitis of Ulna Diaphysis in a Child: A Case Report
March 10, 2024 Unifocal Tubercular Osteomyelitis of Ulna Diaphysis in a Child: A Case Report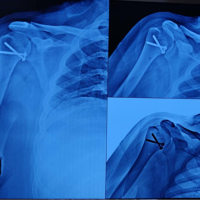 December 10, 2021 Lesser Tuberosity Avulsion Fracture: A Rare Case Report
December 10, 2021 Lesser Tuberosity Avulsion Fracture: A Rare Case Report July 10, 2020 Total Elbow Arthroplasty as Treatment of Non-union with Bone Loss of Distal Humerus – A Case Report
July 10, 2020 Total Elbow Arthroplasty as Treatment of Non-union with Bone Loss of Distal Humerus – A Case Report