
This article regarding Brown’s tumor underscores the variability in presentation and highlights the importance of multidisciplinary care in optimizing outcomes of treatment.
Dr. Ajith John K, Quarters number 12, Hospital Campus, Amala Hospital, Thrissur, Kerala, India E-mail: ajith.polutan@gmail.com
Abstract
Introduction: Brown tumors are rare, non-neoplastic osteolytic lesions resulting from hyperparathyroidism (HPT), often mimicking bone metastases. Although their incidence has declined in developed nations due to early biochemical screening, they remain clinically relevant in regions with prevalent Vitamin D deficiency. We present a 13-year retrospective analysis of brown tumor cases managed at a tertiary care center in South India.
Material and Methods: Twelve patients diagnosed with brown tumors between 2012 and 2025 were retrospectively reviewed. Clinical presentation, biochemical findings, radiological features, anatomical distribution, management strategies, and outcomes were analyzed. All cases were histologically confirmed and correlated with HPT profiles.
Results: The mean age was 43.3 years (range 25–63), with a female predominance (66.6%). Localized pain was the most common presentation (58.3%), followed by pathological fractures and soft-tissue swellings. Primary HPT accounted for 83.3% of cases, whereas 16.7% were secondary. Sixteen tumors were identified, most frequently affecting the femur and hand. Conservative management was adopted in 7 patients (58.3%), whereas 5 patients (41.7%) underwent surgical intervention, including fixation, curettage, and hemiarthroplasty. Eight patients underwent parathyroidectomy, predominantly for adenomas. Two patients died before surgery due to complications of hypercalcemia. Lesions regressed following parathyroidectomy in most cases, with a mean fracture healing time of 3 months.
Conclusion: Brown tumors, though rare, should be considered in the differential diagnosis of lytic bone lesions in endemic regions. Biochemical testing and timely parathyroidectomy remain central to management. This case series, the first from South India, underscores the variability in presentation and highlights the importance of multidisciplinary care in optimizing outcomes.
Keywords: Brown tumor, hyperparathyroidism, parathyroidectomy, lytic bone lesion, case series.
The parathyroid glands secrete parathyroid hormone (PTH), which affects the kidney, intestine, and bone to control serum calcium levels. The endocrine condition known as hyperparathyroidism (HPT) is characterized by elevated, unbalanced osteoclast activity as a result of PTH secretion [1]. By damaging the bones, HPT can result in non-cancerous osteolytic lesions called brown tumors. Another name for the brown tumor is “osteitis fibrosa cystica” [2]. Non-neoplastic reactive tissue, significant bone resorption, osteoclasts with multinucleated giant cells, vascular and growing fibrous tissue, and bleeding are some of the lesion’s distinguishing characteristics [2]. The term brown tumor is a result of its abundant vascularity, bleeding, and hemosiderin deposits [2]. Primary, secondary, or tertiary HPT (THPT) can result in reactive osteolytic lesions known as brown tumors [2]. The condition known as primary HPT (PHPT) is brought on by the overproduction of PTH. PHPT is most frequently caused by parathyroid adenoma (80%) and parathyroid hyperplasia (10–25%). Rarely, parathyroid carcinoma (<1%) and multiple adenomas (5%) are observed. In PHPT, hyperphosphatemia and hypercalcemia are the most frequent laboratory results [3]. Secondary HPT (SHPT) is a frequent side effect of chronic renal failure. The production of calcitriol, the active form of Vitamin D in late-stage kidney disorders, is compromised, resulting in hypocalcemia. In addition, phosphate excretion is compromised. PTH is released more often when the parathyroid glands are continuously stimulated by low ionized calcium and high phosphate levels [4]. When SHPT lasts for a long time, and the parathyroid glands become overactive on their own, the disease known as THPT develops. Similar to SHPT, THPT is brought on by end-stage renal disease [5]. According to the literature, the incidence of brown tumors is roughly 1.5–2% in SHPT and 3–4.5% in PHPT [6]. Because of better screening methods in recent years, early detection is possible for HPT. Brown tumors, a characteristic sign of HPT, have become less common as a result of early detection and treatment of the condition [7]. Brown tumors appear as distinct, expansile lytic lesions with a thin outer layer of bone on radiographs. Other radiographic findings include osteopenia, subperiosteal bone resorption, and the salt and pepper sign in the skull. That may be present in HPT together with brown malignancies [8]. Brown tumors may appear as a single lesion or as several. On radiological imaging, several bone lesions could be mistakenly identified as bone metastases. PTH measurement and biochemical tests play a significant role in differential diagnosis [9]. The pelvis, ribs, clavicle, mandible, femur, and other long bones are frequently seen to have brown tumors. Numerous clinical indicators and symptoms could be seen based on the lesions’ location and size. One may notice pathologic fractures, generalized skeletal discomfort, or localized bone pain. However, some patients do not exhibit any symptoms and are accidentally diagnosed by radiography [10]. The location and size of the lesions, along with the functional problems they cause, dictate the therapy options for brown tumors. Parathyroidectomy may be enough for certain lesions, and when the unbalanced osteoclastic activity returns, the lesions may regress. However, for certain lesions, conservative treatment is insufficient, and prophylactic fixation is required to improve functional outcomes and reduce the risk of pathological fractures [11]. Although uncommon, any orthopedic surgeon who comes across a lytic lesion in the bone should have a brown tumor in their mind as a differential diagnosis. The purpose of this study was to retrospectively review 13 years of experience with brown tumors and 38 years of orthopedic oncology experience by the senior author in a tertiary care facility in South India. No similar studies have been done in South India, especially in a single institution, which can clearly show the demographics and treatment outcome in brown tumors.
We retrospectively analyzed the records of 12 consecutive patients with brown tumors who had been treated in our institution during the period from May 2012 to 2025. Out of 12 patients, two patients died during the time of treatment, and two patients were treated outside the hospital after initial diagnosis. We examined the files in the hospital archive of all patients who received treatment with the diagnosis of brown tumors within the specified time frame. The consultation notes of endocrinology and endocrine surgeons were evaluated using the hospital archive, and pathology reports were examined, and biochemical results (Ca, PTH) were reviewed. All patients whose diagnosis of brown tumor was histologically confirmed according to the pathology report and whose laboratory results were consistent with HPT were included in the study. The pre-operative radiological images of the patients were examined. Pre-operative plain radiographs of all patients (12 patients) were obtained from hospital records. By evaluating radiological images, data regarding parameters such as the size, number, and location of the lesion were recorded. The patients were classified according to the types of HPT. It was determined which patients underwent parathyroidectomy. The lesions were classified as those undergoing orthopedic surgical procedures or those followed conservatively. Surgical procedures were categorized by examining the operation reports in hospital records. Post-operative complications such as wound problems and implant failure were investigated by examining post-operative radiographic images. Descriptive statistics were used to characterize demographic variables of patients. Mean, median, and standard deviation (SD) values were used to show descriptive statistics. Pearson correlation coefficients for the numerical variables of PTH level, calcium, and age were also assessed.
The study included a total of 12 patients. The mean age of the patients was 43.33 years, with a median of 44 years. The age range was broad, from 25 to 63 years. The patient cohort was predominantly female, comprising 66.66% (n = 8) of the total, whereas males accounted for 33.33% (n = 4). The mean follow-up period was 31.42 months, though this was highly variable, with a large SD of 34.01 and a median of 17 months, ranging from 8 to 120 months. The most common first presenting symptom was localized pain, reported by seven patients. Other symptoms included pathologic fracture, widespread pain, hypercalcemia symptoms, and soft-tissue mass/swelling, each noted in two patients. PHPT was the most frequent diagnosis, affecting 10 out of 12 patients (83.3%). 2 patients (16.7%) had a diagnosis of SHPT. Regarding treatment, conservative management was the primary approach for 7 of the patients (58.33%), whereas a substantial portion of the patients (n = 5, 41.66%) underwent surgical intervention (Table 1).
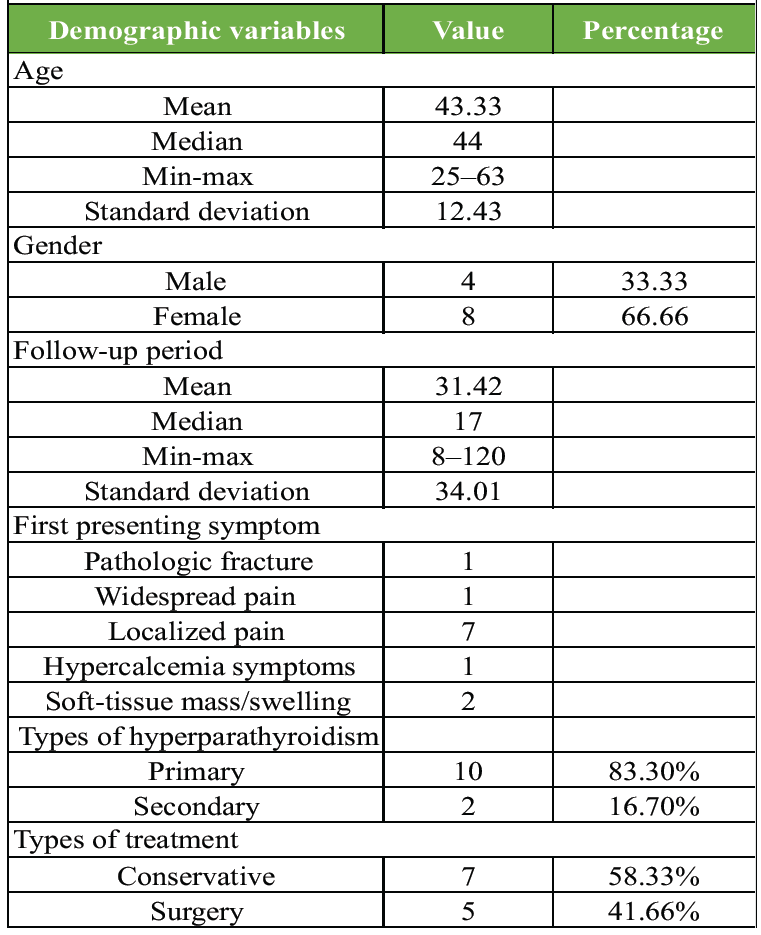
Table 1: Demographic variables of the patients
Out of 12 patients, the cohort’s treatment was divided into two main categories: Conservative management and surgical intervention (parathyroidectomy). Conservative treatment was the most common approach, utilized in 7 patients (58.33%). Surgical intervention was performed on 5 patients (41.67%). This category included a variety of procedures such as nailing for subtrochanteric fractures, curettage of the scapula, soft-tissue excision, nailing of the humerus, and hemiarthroplasty of the femur, with each procedure performed on one patient (Table 2).
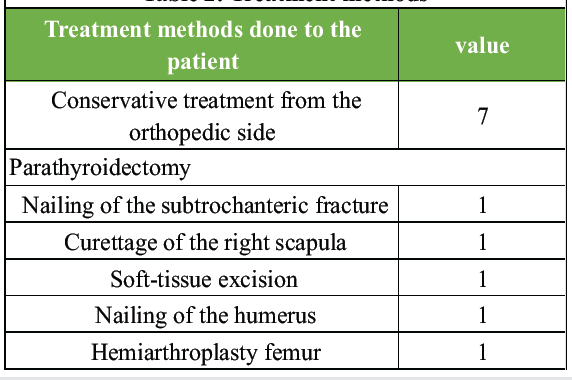
Table 2: Treatment methods
A total of 16 tumors were identified across the 12 patients. The most frequent anatomical locations for the tumors were the neck of the femur/intertrochanteric region and the fingers/hand, each accounting for 3 tumors (18.75%). Shaft of the femur: 2 tumors (12.5%). Scapula, olecranon, distal humerus, distal femur, proximal humerus, ulna, lateral malleolus, and clavicle: each of these locations had one tumor (6.25% each). The findings suggest that while femur and hand tumors are the most prevalent, the disease can affect a wide range of anatomical sites (Table 3).
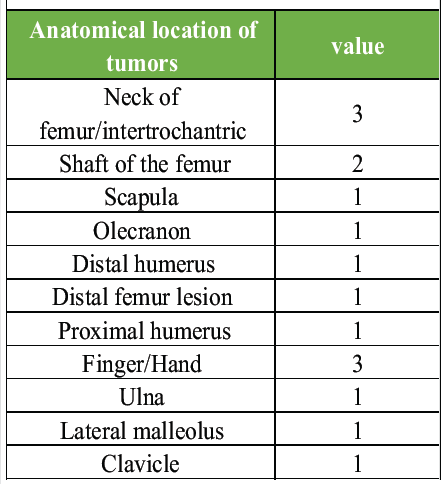
Table 3: Anatomical location of tumors
PTH and calcium
There is a moderate positive correlation (r = 0.407) between PTH and calcium levels. This suggests that as PTH levels increase, calcium levels also tend to increase, which is a classic finding in PHPT. Age and calcium: A weak positive correlation (r = 0.320) exists between age and calcium levels, indicating that older patients in this sample tend to have slightly higher calcium levels. Age and PTH: There is a very weak, almost negligible, negative correlation (r = −0.052) between age and PTH level (Table 4).
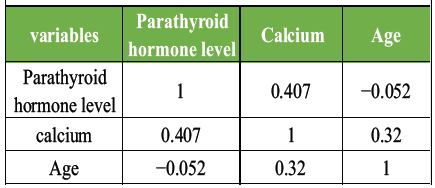
Table 4: The Pearson correlation coefficients for the numerical variables
Analyzing Table 5, a 34-year-old male patient presented to our institution with swelling on the right olecranon clinically similar to olecranon bursae, and a magnetic resonance imaging showed another lesion on the distal humerus, which raised suspicion of HPT. The diagnosis was made and the lesion treated conservatively (Fig. 1).
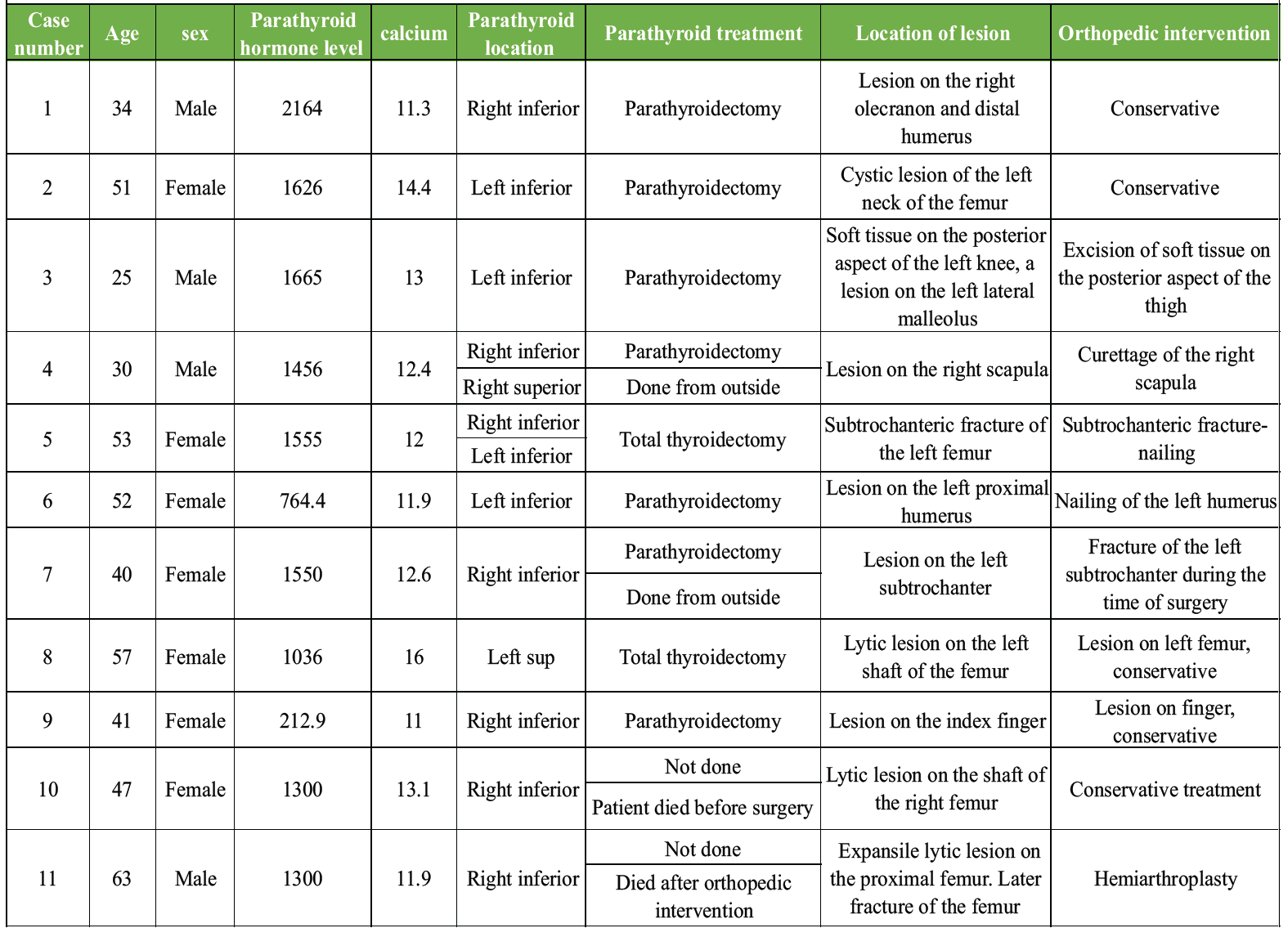
Table 5: Summary of treatment methods

Figure 1: A 34-year-old male patient with swelling on the right olecranon region.
A 51-year-old female patient complained of pain; an X-ray of the left hip showed a lytic lesion on the neck of the femur, and an investigation showed HPT. She was advised to strictly avoid bearing weight for 6 weeks after the parathyroidectomy, and the lesion healed in 3 months (Fig. 2).

Figure 2: A 51-year-old female patient with a lytic lesion on the left trochanteric region.
A 25-year-old male patient came to our outpatient department with swelling on the posterior aspect of the knee. A biopsy showed a giant cell-rich lesion, and after 3 months, the patient presented with pain in the ankle joint, which aroused the suspicion of HPT, and the PTH level was on the higher side. A parathyroidectomy was done, and the lesion subsided.
A 30-year-old male patient with complaints of pain in the right shoulder for 1 year met with a road traffic accident, and an X-ray showed a lytic lesion on the right scapula. Curettage was done outside the hospital, and a biopsy showed chondrosarcoma. An X-ray showed another lytic lesion on the ulna, which aroused the suspicion of HPT, and parathyroidectomy was done, and the lesion healed.
A 53-year-old female patient with complaints of multiple joint pains had a positron emission tomography scan taken from outside, which showed multiple lesions all over the body. In view of this, a diagnosis of metastasis was considered (Fig. 3).

Figure 3: A 53-year-old female patient with complaints of multiple joint pains had a positron emission tomography (PET) scan taken from the outside – PET scan showed multiple bone lesions along the body diagnosis of metastasis was considered, and later on proved to be a case of hyperparathyroidism.
The PTH level was on the higher side, and a diagnosis of HPT was made. The lesion on the trochanteric region was treated conservatively with strict non-weight-bearing. Parathyroidectomy was done for the patient, and post-surgery, the patient incurred a subtrochanteric fracture at home, and nailing was done fracture healed within 3 months.
A 52-year-old patient presented with pain in the left shoulder. X-ray showed a lytic lesion on the humerus, and PTH was on the higher side, so a diagnosis of HPT was made. The patient was not willing to undergo a parathyroidectomy, and nailing was done, but intraoperatively, we were not able to lock the distal screw due to the fragility of the bone, so we put a U slab. A parathyroidectomy was done, and the bone healed within 2 months with a full range of motion.
A 40-year-old female patient with a lytic lesion on the left subtrochanteric region was diagnosed with HPT. A parathyroidectomy was done at an outside institution; during patient positioning, the subtrochanteric fracture was treated conservatively with traction. The fracture has healed, but the limb length discrepancy is still persisting.
A 57-year-old female patient with a lytic lesion on the left shaft of the femur, and the lesion got healed after parathyroidectomy.
A 41-year-old female patient with a history of falls and complaints of pain in her hand. X-ray showed a lesion on the index finger, which healed after parathyroidectomy (Fig. 4).

Figure 4: A 41-year-old female patient with a history of falls and complaints of pain in her hand. X-ray showed a lesion on the index finger, which healed after parathyroidectomy.
A 47-year-old female patient with a lytic lesion on the shaft of the right femur underwent curettage, which was done outside the hospital, and bone cementing and plating were done. Later, the patient presented with hand pain, and a lesion was noted on the p2 of the middle finger. Later, a diagnosis of HPT was made. The patient died before the parathyroidectomy surgery.
A 63-year-old male patient presented with pain in the left hip. An X-ray showed an expansile lytic lesion on the proximal femur, and later on, the neck of the femur fractured, and hemiarthroplasty was done before the parathyroidectomy. The patient died before the parathyroidectomy (Fig. 5).

Figure 5: A 63-year-old male patient presented with pain in the left hip. X-ray showed an expansile lytic lesion on the proximal femur, and later on, the neck of the femur fractured.
A 27-year-old female patient with a history of left clavicle fracture without a trivial fall was treated conservatively and presented to our emergency department with symptoms of hypercalcemia, and was later on diagnosed with HPT, and parathyroidectomy was performed. Following the parathyroidectomy, the patient’s condition was monitored closely for any complications related to hypercalcemia. Out of 12 cases, 8 cases underwent parathyroidectomy at the institution, done by an endocrine surgeon. Two patients had undergone surgery at an outside institution, and two patients died before parathyroidectomy. Two patients underwent total thyroidectomy due to multinodular goitre and papillary carcinoma.
In 1891, Recklinghausen published the first description of osteitis fibrosa cystica [12]. The term “brown tumors” is used in the literature because of its abundant vascularity, which gives it color, and hemosiderin deposits [13]. Brown tumors may result from primary, secondary, or THPT [11]. Over the previous several decades, there have been notable changes in the clinical presentation of PHPT. It is well known that traditional overt complications such as cholelithiasis, nephrolithiasis, and brown tumors are becoming less common. Although the prevalence of brown tumors in PHPT was as high as 58–69% in earlier research, it is currently <5%, particularly in developed nations [11]. In the early 1970s, routine serum calcium screening began to be used in developed nations. In circumstances where there are no symptoms, this circumstance has made it easier to diagnose PHPT early. The extensive use of biochemical screening tests has reduced the incidence of severe forms of PHPT associated with brown tumors. There may be a connection between less severe Vitamin D insufficiency and the lower incidence of brown tumors in Western industrialized nations. It is well known that in nations such as China, India, and Thailand, where there is a major Vitamin D deficiency, severe skeletal symptoms such as brown tumors are still commonly seen [14]. In our nation, Vitamin D insufficiency is also widespread and a significant public health issue [15]. Brown tumors may appear as a single lesion or as several. When diagnosing a single bone lesion of a brown tumor, additional possible explanations include aneurysmal bone cyst, giant cell tumor, giant cell granulomas, single bone cysts, and bone cysts. It may be challenging to distinguish many bone lesions of a brown tumor from leukemia, multiple myeloma, osteolytic metastases, and Langerhans’ cell histiocytosis [11]. Multinucleated large cells, proliferating fibrous tissue, and dark hemosiderin deposits are characteristics of their histology. Since other lesions, such as giant cell tumors, giant cell granulomas, and aneurysmal bone cysts, may have comparable macroscopic and microscopic features, histology by itself cannot make a conclusive diagnosis [16]. In order to establish a conclusive diagnosis, biochemical tests and PTH level assessment are essential [17].
In radiological imaging, several bone lesions from a brown tumor may mimic bone metastases. Measuring PTH levels makes it easy to distinguish between brown tumors and metastases. Malignant hypercalcemias can be seen in metastases; however, PTH increases are nearly never observed. In contrast, brown tumors have higher PTH levels [18]. A study done on 50 958 patients with PHPT median age was 65 years, 74.0% were female, and the median calcium level was 10.9 mg/dL [19]. In our study, the mean age was 43.33, with a female preponderance of 8 out of 12 patients, who were female, and a mean calcium level of 12.71. Localized bone pain is one of the classic symptoms of HPT, and 7 out of 12 patients had this symptom, and the other symptoms, including multiple joint pain and pathological fracture, were seen in the subtrochanteric region [20]. Unusual presentation of HPT is a soft-tissue mass, which was seen in three cases: one on the posterior aspect of the knee, another on the right scapula, and a third on the olecranon region [21]. These findings highlight the diverse manifestations of the disease, emphasizing the need for thorough clinical evaluation in patients presenting with atypical symptoms. Early recognition and intervention can significantly improve patient outcomes and prevent further complications related to bone health. PHPT is the most common type, and in our case series, 10 were primary, and 2 were secondary. The anatomic location is most common on the neck of the femur or the intertrochanteric region in 3 out of 12 cases [19]. In a study done by Yazici et al., 243 patients (a total of 254 adenomas) were operated on for PHPT. The most common adenoma locations were the right inferior gland: 89 cases (37.7%), followed by the left inferior gland with 76 cases (32.1%) [13]. In our study, 7 out of 13 cases were right at an inferior location. These findings underscore the importance of anatomical considerations in surgical planning for patients with PHPT. Further research is needed to explore the correlation between adenoma location and patient outcomes post-surgery. The 2019 Conference of the European Society of Endocrine Surgeons, devoted to “Volumes, Outcomes and Quality Standards in Endocrine Surgery” concluded that parathyroid surgery performed by high-volume, specialized endocrine surgeons (≥40 procedures/year) is associated with higher cure rates, lower complication and recurrence rates, and better cost-effectiveness, especially for complex cases such as non-localizing adenomas or reoperations [22]. 8 out of 12 cases done at our institution are done by an endocrine surgeon, which is the best option in parathyroidectomy since it is a complicated surgery. Two patients have undergone total thyroidectomy due to multinodular goitre, and another one due to papillary carcinoma. During parathyroidectomy, after excision PTH level is sent intraoperatively and checked for a drop in PTH level by 50%, and the surgery will proceed. Christiansen et al. conducted a 3-year follow-up on patients after parathyroidectomy. Bone mineral density (BMD) increased significantly, especially in trabecular-rich sites such as the spine and hip. Most gains occurred within the first 6 months, with continued slower improvement over 2.5 years [23]. In our study mean recovery from fractures was 3 months both clinically and radiologically. Symptoms of hypercalcemia should not be ignored, as two of our patients died before parathyroidectomy due to myocardial infarctions, and calcium levels should be monitored by an endocrine specialist before and after surgery. A limitation of the study is that it is a retrospective study with a small sample size, but considering the rarity of the disease and the study conducted at a tertiary health center in South India is a strong point related to the study. Ideally, follow-up should be done with assessing dual-energy X-ray absorptiometry scan or BMD, which was not done in our study.
Brown’s tumor is one of the conditions that are misdiagnosed and treated by orthopedics due to its variability in clinical presentation. A high index of suspicion and investigation will help in the diagnosis. Early diagnosis through biochemical testing and appropriate surgical management, including parathyroidectomy performed by endocrine surgeons, improves outcomes. Future studies are needed with a larger patient number, and follow-ups are needed in this field, which is lacking right now.
Brown’s tumor is one of the conditions that is misdiagnosed due to its variability in clinical presentation, but it can be diagnosed by a high index of suspicion and biochemical testing.
References
- 1. Rolighed L, Rejnmark L, Christiansen P. Bone involvement in primary hyperparathyroidism and changes after parathyroidectomy. Eur Endocrinol 2014;10:84-7. [Google Scholar] [PubMed]
- 2. Misiorowski W, Bilezikian JP. Osteitis fibrosa cystica. JBMR Plus 2020;4:e10403. [Google Scholar] [PubMed]
- 3. DeLellis RA, Mazzaglia P, Mangray S. Primary hyperparathyroidism: A current perspective. Arch Pathol Lab Med 2008;132:1251-62. [Google Scholar] [PubMed]
- 4. Saliba W, El‑Haddad B. Secondary hyperparathyroidism: Pathophysiology and treatment. J Am Board Fam Med 2009;22:574-81. [Google Scholar] [PubMed]
- 5. Chandran M, Wong J. Secondary and tertiary hyperparathyroidism in chronic kidney disease: An endocrine and renal perspective. Indian J Endocrinol Metab 2019;23:391-9. [Google Scholar] [PubMed]
- 6. Staessen JA, Stijnen T. Brown tumor prevalence in primary and secondary hyperparathyroidism-literature review. J Clin Endocrinol Metab 1998;83:262-6. [Google Scholar] [PubMed]
- 7. Aksoy D, Sertkaya O, Sönmez K, Coşkun A. A reference finding rarely seen in primary hyperparathyroidism: Brown tumor. Arch Med Sci 2013;9:705-9. [Google Scholar] [PubMed]
- 8. Xie C, Tsakok M, Taylor N, Partington K. Imaging of brown tumours: A pictorial review. Insights Imaging 2019;10:75. [Google Scholar] [PubMed]
- 9. Saghafi M, Seif M, Jabbari A, Tabrizi A. Brown tumor of the bone: A case report and review of literature. Iran J Radiol 2018;15:e60882. [Google Scholar] [PubMed]
- 10. Gupta S, Sood S, Singh R. Brown tumor of hyperparathyroidism: A rare presentation. J Orthop Case Rep 2016;6:52-5. [Google Scholar] [PubMed]
- 11. Karaca MO, Özyıldıran M, Savran MD, Başarır K, Yıldız HY. Brown tumors: Retrospective analysis of 26 cases. Arch Orthop Trauma Surg 2024;144:2927-34. [Google Scholar] [PubMed]
- 12. Von Recklinghausen FD. Die fibröse oder deformirende ostitis, die osteomalacie und die osteoplastische carcinose in ihren gegenseitigen beziehungen. In: Festschrift Für Rudolf Virchow Zu Seinem 71. Geburtstage. Berlin: G. Reimer; 1891. [Google Scholar] [PubMed]
- 13. Yazici P, Mihmanli M, Bozdag E, Aygun N, Uludag M. Location of parathyroid adenomas in primary hyperparathyroidism: Where to look? World J Endocrine Surg 2015;7:1-5. [Google Scholar] [PubMed]
- 14. Singh O, Liakopoulos V, Silverberg SJ. Vitamin D in primary hyperparathyroidism: Effects on clinical, biochemical, and densitometric presentation. J Bone Miner Res Suppl 2014;29 Suppl 1:P223-8. [Google Scholar] [PubMed]
- 15. Ritu G, Gupta A. Vitamin D deficiency in India: Prevalence, causalities and interventions. Nutrients 2014;6:729-75. [Google Scholar] [PubMed]
- 16. Sundaram M, McGuire MH. Brown tumor of hyperparathyroidism: Radiologic-pathologic correlation. Radiographics 2001;21:1263-70. [Google Scholar] [PubMed]
- 17. Mishra A, Gupta S. Brown tumor of the jaw: A rare presentation of primary hyperparathyroidism. J Oral Maxillofac Pathol 2012;16:444-8. [Google Scholar] [PubMed]
- 18. Akbar MS, Lennox P. Brown tumors mimicking bone metastases. J Natl Med Assoc 2006;98:1007-10. [Google Scholar] [PubMed]
- 19. Sant VR, ElNakieb Y, Lehmann CU, Rousseau JF, Maalouf NM. Patient characteristics, management, and outcomes in a novel cohort of primary hyperparathyroidism. J Endocr Soc 2024;8:bvae096. [Google Scholar] [PubMed]
- 20. Bandeira F, Cusano NE, Silva BC, Cassibba S, Almeida CB, Machado VC, et al. Bone disease in primary hyperparathyroidism. Arq Bras Endocrinol Metabol 2014;58:553-61. [Google Scholar] [PubMed]
- 21. Irvell L, Werner I, Grimelius L. Soft tissue calcification in hyperparathyroidism. Acta Med Scand 1970;187:145-51. [Google Scholar] [PubMed]
- 22. Iacobone M, Scerrino G, Palazzo FF. Parathyroid surgery: An evidence-based volume‑outcomes analysis: European society of endocrine surgeons (ESES) positional statement. Langenbecks Arch Surg 2019;404:919-27. [Google Scholar] [PubMed]
- 23. Christiansen P, Steiniche T, Brixen K, Hessov I, Melsen F, Heickendorff L, et al. Primary hyperparathyroidism: Effect of parathyroidectomy on regional bone mineral density in Danish patients: A three-year follow-up study. Bone 1999;25:589-59. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Unveiling the Uncommon – A Rare Skeletal Encounter of Tuberculosis of the Ulna Diaphysis in an Adult Female Patient
July 1, 2026 Unveiling the Uncommon – A Rare Skeletal Encounter of Tuberculosis of the Ulna Diaphysis in an Adult Female Patient July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall
July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series
July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series February 1, 2026 Does Adding Lateral Extra-Articular Tenodesis Improve Outcomes After Arthroscopic Anterior Cruciate Ligament Reconstruction? A Longitudinal Comparative Study
February 1, 2026 Does Adding Lateral Extra-Articular Tenodesis Improve Outcomes After Arthroscopic Anterior Cruciate Ligament Reconstruction? A Longitudinal Comparative Study