
Fixation of acute osteochondral defects has been shown to yield satisfactory functional outcomes, preserve articular surface congruity, and represent a cost-effective alternative to implant use.
Dr. Jyoti Gupta, Senior Resident, Department of Orthopaedics, Flat number-2 1st Floor, Aashraya Apartment, Green-Woods Society, Katraj, Pune, Maharashtra, India. E-mail: jg97286@gmail.com
Abstract
Introduction: Post-traumatic osteochondral defects can cause chronic pain, reduced range of motion, and early osteoarthritis. Repairing these defects is clinically challenging due to the avascular nature of cartilage and limited self-repair capacity.
Case Report: A 24-year-old male with a large lateral femoral condyle osteochondral defect following trauma presented with knee pain and restricted movement. Diagnostic arthroscopy confirmed the defect along with an intact ligament and meniscus. The osteochondral fragment was preserved and repaired using a novel in situ fixation technique. The fragment was fixed over the defect using Vicryl sutures through medial parapatellar arthrotomy. At 1-year follow-up, stable fixation was confirmed on imaging, and the patient achieved a full range of motion and pain-free daily activities. Post-operative knee injury and osteoarthritis outcome scores and magnetic resonance imaging demonstrated satisfactory healing.
Conclusion: The described suture fixation technique provides a low-cost, effective, and joint-preserving alternative for acute osteochondral defects in young patients, promoting functional recovery without donor-site morbidity.
Keywords: Cartilage preservation, in situ fixation, osteochondral defect, post-traumatic injury, Vicryl suture repair.
Damage to the articular surface frequently results in pain, instability, and functional impairment, often predisposing patients to early degenerative joint disease [1]. These lesions, whether caused by direct trauma, osteochondral fractures, or chronic wear, pose a significant challenge because articular cartilage has an extremely limited capacity for intrinsic repair. Over several decades, orthopaedic surgeons have therefore developed multiple joint-preserving techniques aimed at restoring hyaline or hyaline-like cartilage within articular defects [2]. Such interventions are particularly important in the younger population, as osteochondral defects caused by osteoarthritis or trauma can lead to joint deformity, limited mobility, and pain [3]. Non-operative treatments may provide temporary relief, and symptom control is often achieved using anti-inflammatory medication, viscosupplementation, bracing, orthotic support, and activity adjustments. However, even minor cartilage injuries tend to heal poorly and may progressively lead to degenerative changes over time, especially when left unmanaged [4]. In elderly patients, total joint arthroplasty remains the standard treatment because it reliably restores function in the setting of widespread degeneration. In contrast, for younger individuals or those with focal lesions, preservation of native joint structure and function is crucial to avoid early arthroplasty and its associated long-term complications [3]. Osteochondral fractures of the knee, though relatively common in active individuals, continue to pose diagnostic and therapeutic challenges. Milgram et al. were among the first to describe these injuries, which involve disruption of both the articular cartilage and the underlying subchondral bone [5]. Early identification and appropriate fixation are essential to preserve the viability of the fragment and to restore the joint surface. We present a unique case of repairing the osteochondral fragment found secondary to acute trauma in a young male patient with an excellent 1-year outcome, using a low-cost, technically simple, and biologically favourable suture fixation method that has not been widely described in existing literature.
A 24-year-old male presented with a 2-month history of pain in the right knee and difficulty walking following a twisting injury sustained while descending stairs. Clinical examination revealed lateral joint line tenderness with a painful and restricted range of motion, consistent with mechanical symptoms arising from an intra-articular lesion. McMurray’s test was positive for both medial and lateral menisci, suggesting possible associated meniscal pathology, although ligament laxity tests came out to be negative, indicating preserved ligamentous stability. Initial imaging with a radiograph (Fig. 1) revealed slight blurring of the lateral femoral condyle on the AP view, raising suspicion for a subtle osteochondral lesion.

Figure 1: Pre-operative X-ray.
Further assessment with magnetic resonance imaging (MRI) (sagittal, coronal and axial; Fig. 2) demonstrated thinning and focal cartilage loss over the mid-lateral femoral condyle with mild subchondral marrow oedema. These findings were suggestive of an osteochondral injury.

Figure 2: Pre-operative magnetic resonance imaging sections.
In addition, MRI revealed a Grade II signal in the body and posterior horn of the lateral meniscus with a radial tear, correlating with the clinical findings. Pre-operative Knee Injury and Osteoarthritis Outcome (KOOS) score: 91. 4.
Surgical procedure:
The patient was positioned supine on the operating table following the administration of spinal anaesthesia. Standard sterile preparation and draping were performed. Diagnostic arthroscopy was initiated through the anterolateral and anteromedial portals. Systematic joint inspection revealed an osteochondral defect (Fig. 3) located over the weight-bearing surface of the lateral femoral condyle.

Figure 3: Arthroscopic image of the defect seen on diagnostic arthroscopy.
The articular margins were well defined, and both ligamentous structures and the menisci appeared intact, with no associated chondral flaps or instability. Based on the size of the lesion, the presence of a sizeable osteochondral fragment, and the need for precise anatomical reduction, the surgical team decided to convert to an open approach to ensure optimal visualisation and manipulation of the fragment. A medial parapatellar arthrotomy was performed to allow direct visualisation and manipulation of the lesion (Fig. 4).
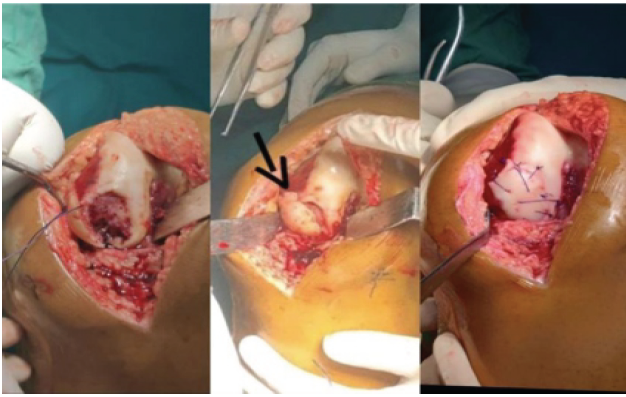
Figure 4: Osteochondral defect over lateral condyle weight bearing area followed by osteochondral fragment extracted from the lateral gutter and final fixation of the osteochondral fragment. The arrow shows the suture passed through the drilled tunnel which helped to secure the fragment over the defect.
Upon entering the joint, the osteochondral fragment (Fig. 5) measuring 2.5 cm × 2.5 cm was identified within the lateral compartment.
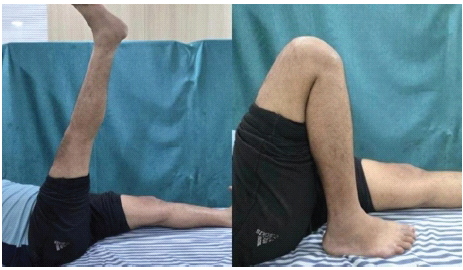
Figure 5: One-year post-operative full knee flexion and extension and quadriceps function.
It was loose but structurally viable, showing preservation of cartilage thickness and subchondral bone integrity. The defect site on the lateral femoral condyle was carefully debrided to remove loose debris and create a clean, stable base for fragment reattachment, taking care not to violate the subchondral bone. The fragment itself was prepared by gentle curettage to remove fibrous tissue and by trimming minimal overhanging or frayed cartilage to restore a congruent margin that would align accurately with the surrounding native cartilage. Two K-wires were inserted to temporarily stabilise the fragment in its anatomical position. Once provisional fixation was confirmed both visually and manually, drill tunnels were created on either side of the femoral condyle extending from the base of the defect toward the periphery. These transcondylar tunnels allowed passage of sutures through robust bone stock while avoiding compromise of the articular surface. The fragment was definitively secured into place using multiple end-to-end, simple, non-continuous 3-0 Vicryl sutures (Fig. 6).
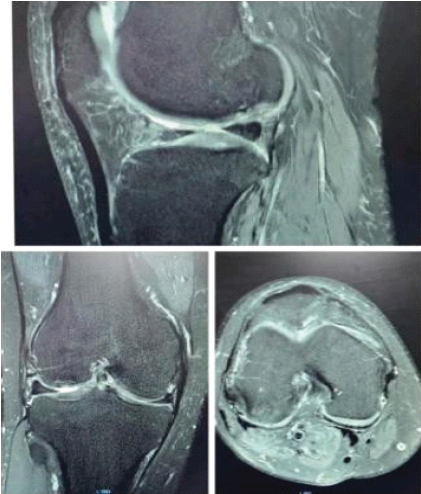
Figure 6: One-year post-operative magnetic resonance imaging sections showing healed cartilage.
Each suture connected the edge of the osteochondral fragment to the adjacent native cartilage, permitting circumferential stabilisation. The use of sutures allowed for controlled apposition of the cartilage margins without hardware prominence, potential implant irritation, or the need for later removal, which is often required with metallic implants. After all sutures were tied and the K-wires removed, the fixation construct was assessed through a gentle range-of-motion examination. The fragment remained stable throughout flexion, extension, and rotational movements, indicating satisfactory mechanical stability. The wound was irrigated thoroughly, the arthrotomy was closed in layers, and sterile dressings were applied. The patient was subsequently shifted to recovery in stable condition.
Rehabilitation process:
Post-operative knee range of motion exercises were started on day one as tolerated to maintain joint mobility and promote early cartilage healing. Non-weight-bearing ambulation with walker support began on day 2, along with static quadriceps and hamstring strengthening exercises, ankle pumps, and active-assisted straight-leg raises. Hip abduction and adduction exercises were introduced after 2 weeks to enhance overall lower-limb strength without compromising fixation. The patient regained a full range of motion (0–140°) (flexion; Fig. 6, extension, and quadriceps function; Fig. 6) and returned to normal daily activities, avoiding high-impact sports per postoperative advice. An MRI (sagittal, coronal, and axial; Fig. 6) at 1-year post-surgery showed a repaired cartilage surface with a wavy contour and areas of hyperintensity consistent with healing. A computed tomography (CT) scan revealed irregularity of the lateral femoral condyle cortex and subarticular cyst formation, correlating with the previous repair site. Post-operative KOOS score: 99.1.
This case illustrates a practical and economical method for stabilising an osteochondral fragment, in which Vicryl sutures are used to secure the fragment to the surrounding cartilage while retaining the native hyaline surface. At the 1-year review, the patient had regained normal knee motion, remained pain-free, and was able to perform routine daily tasks without limitation, except for high-impact activities that were intentionally restricted as part of post-operative guidance. Several other fixation methods, such as headless metallic screws or bioabsorbable devices, are available, but they tend to be more expensive and often require increased procedural complexity. Current evidence supports fixing osteochondral fragments whenever they remain viable, even when presentation is delayed [3]. The technique described in this report maintains joint contour, preserves fragment vitality, and supports reliable functional recovery. Although microfracture is inexpensive and easy to perform, studies frequently report that the tissue formed is fibrocartilage, which does not match the durability of true hyaline cartilage. Some authors have suggested that adding rhBMP-2 may help improve the quality of repair tissue in osteochondral lesions [5]. Despite its accessibility and low cost, microfracture alone may not provide predictable long-term results, especially for medium or larger defects [6]. Mosaicplasty provides native hyaline cartilage for resurfacing and can achieve excellent restoration, but it is technically demanding and can cause pain at the graft harvest site [7]. Success requires precise shaping of the defect, careful selection of a few larger plugs from the contralateral trochlea, and implantation that achieves a flush, radially orientated, press-fit configuration without damaging the cartilage. Any malalignment >5° or instability should be corrected during the same surgical session. Mosaicplasty is generally reserved for smaller defects, approximately 3 cm² or less, due to donor-site limitations [8]. Autologous chondrocyte transplantation offers strong biological potential but is limited by cost, infrastructure needs, and the requirement for two procedures. A small cartilage biopsy is taken arthroscopically and expanded in the laboratory, after which the cultured cells are implanted during a second surgery to form cartilage resembling native hyaline tissue. Although outcomes may be promising, concerns regarding resources, cost, and donor-site morbidity limit its widespread application [9]. Osteochondral autograft transfer is another established method, involving press-fit placement of cylindrical plugs harvested from non-weight-bearing regions into focal full-thickness lesions [10]. This technique provides living hyaline cartilage with its supporting subchondral bone and offers immediate mechanical stability. Many patients return to their previous activity levels sooner than expected; however, a portion may continue to experience pain or recurrent effusions requiring further treatment after resuming sport [11]. In contrast, the method presented in this report provides a single-stage, less complex alternative that avoids donor-site morbidity while delivering stable fixation and reliable functional outcomes.
Osteochondral defects in young adults can be successfully managed using Vicryl sutures for fragment fixation, provided the injury is acute and the fragment is viable. This single-stage approach demonstrates promising functional outcomes, preserves articular congruity, and offers a low-cost alternative to implant-based repairs. Ensuring bone bed vascularity (paprika sign) and fragment stability are critical for success.
Repair of osteochondral defects allows restoration of joint congruence with satisfactory functional results, while serving as an economical alternative to implant-based methods.
References
- 1. Xu D, Cheng G, Dai J, Li Z. Bi-layered composite scaffold for repair of osteochondral defects. Adv Wound Care (New Rochelle) 2021;10:401-14. [Google Scholar] [PubMed]
- 2. Anthonissen J, Rommens PM, Hofmann A. Mosaicplasty for the treatment of a large traumatic osteochondral femoral head lesion: A case report with two-year follow-up and literature review. Arch Orthop Trauma Surg 2016;136:41-6. [Google Scholar] [PubMed]
- 3. Akkaya M, Simsek ME, Caglar C, Nazligul AS, Akcaalan S, Gursoy S. Fixation of neglected subcutaneous osteochondral fragment of large medial femoral condyle defect in adult male: A case report. J ISAKOS 2022;7:39-43. [Google Scholar] [PubMed]
- 4. Simon TM, Jackson DW. Articular cartilage: Injury pathways and treatment options. Sports Med Arthrosc Rev 2018;26:31-9. [Google Scholar] [PubMed]
- 5. Dang LH, Tran NT, Oh JS, Kwon TY, Lee KB. Effect of bone morphogenetic protein-2 combined with microfracture for osteochondral defect of the talus in a rabbit model. Am J Sports Med 2023;51:1560-70. [Google Scholar] [PubMed]
- 6. Gopinatth V, Jackson GR, Touhey DC, Chahla J, Smith MV, Matava MJ, et al. Microfracture for medium size to large knee chondral defects has limited long-term efficacy: A systematic review. J Exp Orthop 2024;114:e70060. [Google Scholar] [PubMed]
- 7. Andrade R, Vasta S, Pereira R, Pereira H, Papalia R, Karahan M. Knee donor-site morbidity after mosaicplasty: A systematic review. J Exp Orthop 2016;3:31. [Google Scholar] [PubMed]
- 8. Robert H. Chondral repair of the knee joint using mosaicplasty. Orthop Traumatol Surg Res 2011;97:418-29. [Google Scholar] [PubMed]
- 9. El Sayed K, Haisch A, John T. Heterotopic autologous chondrocyte transplantation–a realistic approach to support articular cartilage repair? Tissue Eng Part B Rev 2010;16:603-16.Ma HL, Hung SC, Wang ST, Chang MC, Chen TH. Osteochondral autografts transfer for post-traumatic osteochondral defect of the knee-2 to 5 years follow-up. Injury 2004;35:1286-92. [Google Scholar] [PubMed]
- 10. Werner BC, Cosgrove CT, Gilmore CJ, Lyons ML, Miller MD, Brockmeier SF, et al. Accelerated return to sport after osteochondral autograft plug transfer. Orthop J Sports Med 2017;54:2325967117702418. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Single-Stage Treatment of a Patellar Osteochondral Defect in an Adolescent Using Autologous Minced Cartilage – Platelet-Rich Plasma Scaffold Technique: A Case Report and Technical Considerations
March 1, 2026 Single-Stage Treatment of a Patellar Osteochondral Defect in an Adolescent Using Autologous Minced Cartilage – Platelet-Rich Plasma Scaffold Technique: A Case Report and Technical Considerations November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report
November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report October 1, 2025 Hip Arthroscopy and Chondrofiller Application in Isolated Osteochondral Defect of the Femoral Head
October 1, 2025 Hip Arthroscopy and Chondrofiller Application in Isolated Osteochondral Defect of the Femoral Head May 10, 2021 Anchor Site Fracture Following Arthroscopic Rotator Cuff Repair – A Case Report and Review of the Literature
May 10, 2021 Anchor Site Fracture Following Arthroscopic Rotator Cuff Repair – A Case Report and Review of the Literature