
Extradigital glomus tumours of the knee can mimic degenerative joint disease, particularly when radiographic osteoarthritis is present. Focal, exquisite, cold-sensitive pain localised to a superficial nodule and disproportionate to radiographic findings should prompt orthopaedic clinicians to consider extra-articular soft-tissue pathology and obtain magnetic resonance imaging for further evaluation.
Hiram E. Luigi Martinez, Department of Orthopaedic Surgery, Ponce Health Sciences University School of Medicine, Ponce, Puerto Rico, USA. E-mail: hluigi25@stu.psm.edu
Abstract
Introduction: Glomus tumours are rare benign vascular neoplasms that usually arise in the subungual region. Around the knee, they remain exceptional and may be mistaken for degenerative or cystic pathology. This case highlights that, in patients with focal, exquisitely tender, cold-sensitive pain that is disproportionate to radiographic osteoarthritis, orthopaedic clinicians should broaden the differential diagnosis to include soft tissue pathology and consider magnetic resonance imaging (MRI) to facilitate timely and accurate diagnosis.
Case Report: A 78-year-old Hispanic male presented with a 15-year history of medial left knee pain. Conservative treatment for presumed osteoarthritis provided partial symptomatic relief during the first 7 years; however, during the subsequent 8 years before presentation to our facility, the pain became progressively refractory to conservative measures and increasingly localised to a small palpable, discoloured, superficial medial parapatellar nodule. Radiographs demonstrated mild-to-moderate osteoarthritic changes and a discrete medial soft-tissue radiodensity. Upon evaluation at our clinic, the above history, together with persistent focal tenderness to light touch and cold hypersensitivity, prompted MRI, which demonstrated a 1.3 cm well-circumscribed subcutaneous nodule in the upper medial parapatellar soft tissues, hypointense on T1-weighted images and hyperintense on T2-weighted images, without intra-articular extension or osseous involvement. Complete local excision was performed with a 2 cm gross soft-tissue cuff to the retinacular level, followed by layered closure. Histopathologic examination demonstrated uniform glomus cells arranged around dilated vascular channels. Immunohistochemical staining was positive for muscle actin and alpha-smooth muscle actin and negative for epithelial membrane antigen, S100, cluster of differentiation 34 (CD34), and desmin, confirming a glomus tumour. Margins were free of tumours. The patient experienced immediate complete pain relief and remained symptom-free without recurrence at 12-month follow-up.
Conclusion: A small extradigital glomus tumour can masquerade as osteoarthritic knee pain. When tenderness is focal, exquisite, cold-sensitive, and not explained by radiographs, orthopaedic evaluation should extend beyond arthritis. The clinician should consider MRI and biopsy with histopathologic confirmation to prevent prolonged ineffective treatment.
Keywords: Glomus tumor, extradigital glomus tumor, knee pain, osteoarthritis, soft tissue neoplasm, case report, surgical excision.
Glomus tumours are uncommon benign mesenchymal neoplasms arising from the glomus body, a specialised arteriovenous structure involved in thermoregulation. They account for less than 2% of soft-tissue tumours and classically occur in the subungual region [1,2]. Around the knee, glomus tumours are distinctly rare. Wang et al. reviewed 30 published reports containing 36 cases through December 2020, and subsequent case series and individual reports have expanded the number only modestly [3,4,5]. This limited literature makes each well-documented knee case valuable, especially when it illustrates an orthopaedic diagnostic pitfall rather than only pathologic confirmation. The classic clinical triad includes paroxysmal pain, pinpoint tenderness, and cold hypersensitivity [2,6]. Extradigital tumours may show an incomplete triad and are often delayed or misdiagnosed as osteoarthritis, meniscal pathology, cystic disease, soft-tissue injury, vascular lesions, or neurogenic tumours [2,3,6]. In the knee, the diagnostic challenge is magnified because mild degenerative radiographic findings are common and can distract attention from a small extra-articular pain generator. We report a superficial upper medial parapatellar glomus tumour in a 78-year-old male with a 15-year history of left knee pain initially managed as a degenerative disease. Conservative treatment provided symptom relief during the first 7 years but became ineffective after the pain localised to a palpable, cold-sensitive medial parapatellar nodule 8 years before presentation. The teaching point is that when knee pain is focal, exquisite, cold-sensitive, and not explained by radiographs, orthopaedic evaluation should extend beyond arthritis. Clinicians should consider magnetic resonance imaging (MRI) and biopsy or excision with histopathologic confirmation to prevent prolonged ineffective treatment.
A 78-year-old Hispanic male with hypertension and gastro-oesophageal reflux disease presented for evaluation of a 15-year history of left knee pain. During the first 7 years after symptom onset, the pain was treated as osteoarthritis-related and responded partially to conservative measures. Eight years before presentation to our facility, the patient noticed that the pain became more focal along the medial parapatellar region and was associated with a small palpable superficial nodule. Since that time, the nodule gradually enlarged and became discoloured, and the pain progressively worsened despite continued non-operative management. At presentation, the pain was constant, severe with light touch over the lesion, and exacerbated by cold exposure. The symptoms limited the activities of daily living and made contact with clothing uncomfortable. Physical examination demonstrated a round, superficial soft-tissue mass over the upper medial parapatellar region. The most reproducible pain was elicited by gentle palpation of the mass rather than by joint-line loading or knee range of motion. The overlying skin was glossy and violaceous without breakdown. Initial radiographs demonstrated mild-to-moderate degenerative changes (Fig. 1).
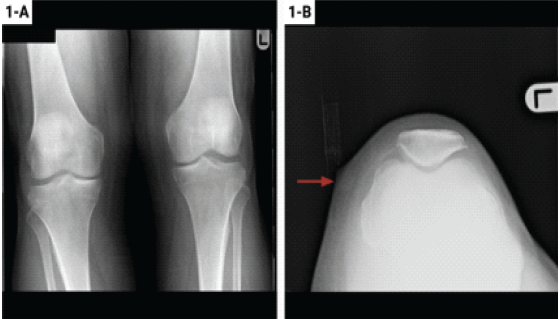
Figure 1: Initial radiographs of the knees: Anteroposterior radiograph of both knees and sunrise view of the left knee. The radiographs demonstrate mild-to-moderate degenerative change consistent with Kellgren-Lawrence grade I-II arthrosis, including subchondral sclerosis and mild joint-space narrowing. The left knee sunrise view shows a discrete, round, superficial medial soft-tissue mass measuring approximately 1.2 × 1.2 cm with cutaneous apex.
Before presentation to our facility, the patient had been treated for presumed degenerative knee disease because radiographs demonstrated osteoarthritic changes, and the superficial lesion had a non-specific appearance. The lesion had also been considered a possible synovial or degenerative cyst. During the initial 7 years after symptom onset, oral analgesics, topical non-steroidal anti-inflammatory gel, and physical therapy provided partial symptom relief. During the subsequent 8 years before presentation, these measures no longer provided meaningful relief. An intra-articular corticosteroid injection was also performed during this refractory period but did not improve the localised pain. Upon presentation, the lack of response to standard osteoarthritis-directed treatment, together with focal cold-sensitive tenderness, prompted reconsideration of the diagnosis. An MRI of the left knee showed a 1.3 cm sharply marginated subcutaneous nodule in the upper medial parapatellar soft tissues, anterior to the joint capsule and medial to the patella. The lesion was hypointense on T1-weighted sequences and hyperintense on T2-weighted sequences, without intra-articular extension, osseous involvement, cortical erosion, or visible continuity with a major neurovascular structure (Fig. 2).
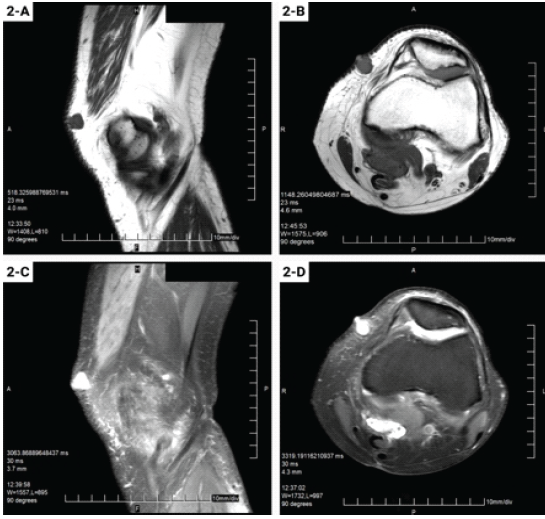
Figure 2: Magnetic resonance images of the left knee: T1-weighted sagittal and axial images and T2-weighted sagittal and axial images of the left knee. The symptomatic lesion measures 1.3 cm and is located in the superficial upper medial parapatellar soft tissues, anterior to the joint capsule and medial to the patella. The nodule is well-demarcated, hypointense on T1-weighted images, hyperintense on T2-weighted images, and shows no intra-articular extension, osseous involvement, or cortical erosion.
These imaging findings were not diagnostic by themselves; however, in the setting of disproportionate focal tenderness and cold sensitivity, they favoured a small benign vascular or neurovascular lesion over primary degenerative knee pain. Given persistent symptoms and failure of conservative care, complete local excision of the symptomatic superficial mass was performed (Fig. 3).
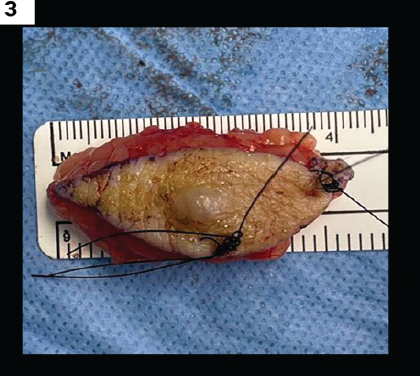
Figure 3: Gross specimen after local excision: Intraoperative gross image of the excised left knee lesion. The specimen is a firm tan-pink nodule with a smooth external surface and surrounding soft tissue. The specimen measures 2.0 cm medial to lateral, 4.5 cm proximal to distal, and 1.5 cm anterior to posterior. The single stitch identifies the proximal margin, and the double stitch identifies the lateral margin.
A complete local excision with an approximately 2 cm gross soft-tissue cuff around the palpable lesion was performed, carried to the retinacular level, rather than a wide oncologic resection. No visible nerve or vascular pedicle was identified. The wound was closed in layers. Gross examination demonstrated a well-circumscribed tan-pink subcutaneous nodule with a smooth surface and punctate whitish foci. Histopathologic examination demonstrated uniform round glomus cells arranged around dilated vascular channels, with margins free of tumour (Fig. 4).
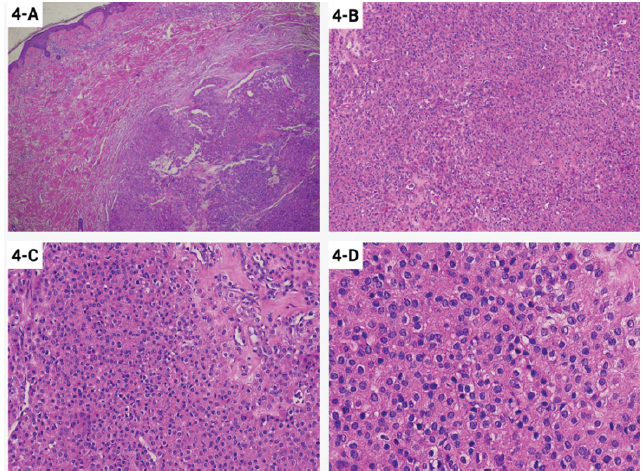
Figure 4: Hematoxylin and eosin-stained sections of the lesion: Representative histologic sections at ×4, ×10, ×20, and ×40 magnification. Low-power images show a well-circumscribed dermal and subcutaneous proliferation. Higher magnification demonstrates uniform round to oval glomus cells with centrally placed nuclei and pale eosinophilic cytoplasm, arranged around dilated vascular channels within focally hyalinized to myxoid stroma.
Immunohistochemical staining showed positivity for muscle actin and alpha-smooth muscle actin (α-SMA). The lesion was negative for epithelial membrane antigen (EMA), S100, cluster of differentiation 34 (CD34), and desmin (Fig. 5).
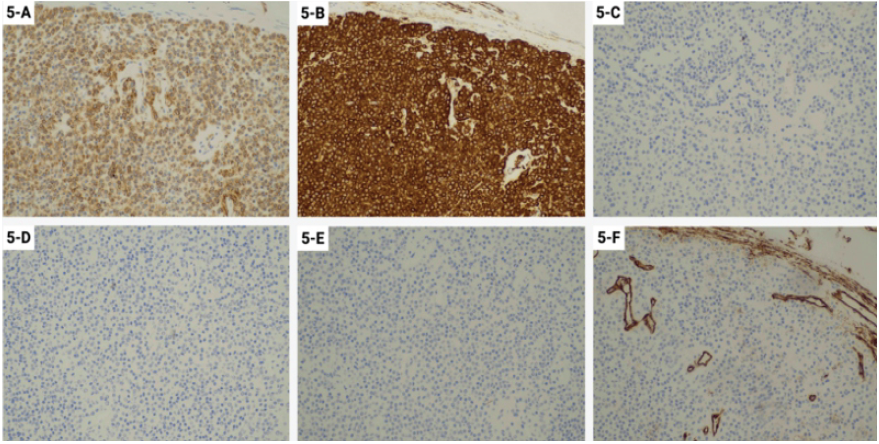
Figure 5: Immunohistochemical staining of the lesion: Immunohistochemical profile at ×20 magnification. The neoplastic cells are positive for muscle actin and alpha smooth muscle actin, supporting smooth muscle differentiation. The lesion is negative for S100 protein, epithelial membrane antigen, desmin, and Cluster of differentiation 34.
These findings confirmed the diagnosis of a glomus tumour. Post-operatively, the patient reported immediate, complete resolution of his characteristic pre-operative pain. At 1 month, the incision was healed, knee motion was unrestricted, ambulation was independent, and he was able to wear regular clothing without discomfort. At 12-month follow-up, he remained symptom-free with no clinical evidence of recurrence.
This case highlights the orthopaedic diagnostic challenge created by a rare extra-articular tumour in the setting of common degenerative disease. Mild-to-moderate osteoarthritis was visible on radiographs and initially supported arthritis-directed treatment, which provided partial relief early in the clinical course. However, the later development of a localised superficial nodule, exquisite focal tenderness, cold sensitivity, and progressive failure of conservative treatment were not compatible with osteoarthritis alone. The diagnostic turning point was recognition of these localised features and the acquisition of MRI. Knee-region glomus tumours are uncommon, but published reports show recurring patterns that are relevant to orthopaedic practice. Wang et al. found 36 cases in 30 reports through December 2020, with locations including soft tissue, popliteal fossa, patellar tendon, iliotibial band, Hoffa’s fat pad, distal femur, and proximal tibia [3]. A later case series found five anterior knee glomus tumours, all in men aged 30 years or older, most with several years of pain before diagnosis [4]. Additional recent reports, including patellar tendon and anterior knee cases, confirm that the number of knee cases remains small and that diagnostic delay is common [5,7,8]. Our patient contributes an elderly presentation with concomitant osteoarthritis, which is a realistic confounder in orthopaedic clinics. The classic triad of paroxysmal pain, pinpoint tenderness, and cold hypersensitivity is helpful but not always complete in extradigital locations [2,6]. Our patient demonstrated two of the three features, namely, pinpoint tenderness and cold hypersensitivity. His pain was constant rather than paroxysmal, and the early partial response to conservative treatment for presumed osteoarthritis further obscured the diagnosis. Nevertheless, the later pain pattern was focal and exquisite, and it was out of proportion to both the size of the lesion and the radiographic arthrosis. MRI is useful for diagnosis, localisation and surgical planning. Typical glomus tumours are well-circumscribed and show low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, often with enhancement when contrast is used [3,9,10,11]. The lesion in this case matched the expected T1 and T2 pattern and was clearly superficial and extra-articular. These details strengthened the decision to treat the superficial mass rather than continue injections or therapy for presumed osteoarthritis. The differential diagnosis for a small painful medial knee mass includes ganglion or synovial cyst, haemangioma, epidermal inclusion cyst, schwannoma, leiomyoma, pigmented lesion, giant cell tumour of tendon sheath, and other benign or malignant soft-tissue tumours [3,12,13,14,15,16,17]. Imaging can narrow this differential, but it cannot reliably confirm a glomus tumour. Histopathology and immunohistochemistry are essential for definitive diagnosis. Histologically, glomus tumours consist of uniform glomus cells arranged around vascular channels, with variable smooth muscle and vascular components [1,18]. Immunohistochemical positivity for muscle actin and α-SMA supports myoid differentiation, while negative S100, EMA, CD34, and desmin help exclude common neural, epithelial, endothelial, and muscular lesions. In this case, the pathologic profile matched a benign glomus tumour. Complete excision is both diagnostic and therapeutic. In knee cases, pain relief is often immediate after removal, and recurrence is uncommon when excision is complete [3,14,19,20]. Our patient’s immediate and durable 12-month relief after local excision, despite persistent radiographic osteoarthritic changes, reinforces that a small superficial tumour can be the primary pain generator. For orthopaedic surgeons, the key is to pause when symptoms are focal, exquisite, cold-sensitive, and disproportionate to the radiographic explanation.
Glomus tumours around the knee are rare but important because they are curable and can mimic common orthopaedic conditions. This case demonstrates how radiographic osteoarthritis can coexist with and distract from a small extra-articular source of pain. In this patient, a 15-year pain history became clinically suspicious after an 8-year period of focal, cold-sensitive, refractory pain associated with a palpable medial parapatellar nodule. MRI defined the lesion, but definitive diagnosis required histopathology and immunohistochemistry. Complete local excision with clear margins produced immediate and durable pain relief.
In patients with presumed osteoarthritic knee pain, symptoms that are focal, exquisitely tender, cold-sensitive, and refractory to standard conservative management should prompt reconsideration of the diagnosis. Orthopaedic clinicians should broaden the differential diagnosis to include extra-articular soft tissue lesions, obtain magnetic resonance imaging to localise and characterise the abnormality, and proceed with biopsy or complete excision when indicated for definitive histopathologic diagnosis and treatment.
References
- 1. Gombos Z, Zhang PJ. Glomus tumor. Arch Pathol Lab Med 2008;132:1448-52. [Google Scholar] [PubMed]
- 2. Schiefer TK, Parker WL, Anakwenze OA, Amadio PC, Inwards CY, Spinner RJ. Extradigital glomus tumors: A 20-year experience. Mayo Clin Proc 2006;81:1337-44. [Google Scholar] [PubMed]
- 3. Wang Y, Li T, Lv Z, Bian Y, Feng B, Liu Y, et al. Glomus tumors around or in the knee: A case report and literature review. BMC Surg 2022;22:97. [Google Scholar] [PubMed]
- 4. Stacy GS, Cipriani NA. Glomus tumours of the knee: A case series. Clin Radiol 2023;78:e123-30. [Google Scholar] [PubMed]
- 5. Daher M, Aouad D, Saade J, Wehbe J. Glomus tumor of the patellar tendon: A case report and review of the literature. J Med Case Rep 2025;19:129. [Google Scholar] [PubMed]
- 6. Lee DW, Yang JH, Chang S, Won CH, Lee MW, Choi JH, et al. Clinical and pathological characteristics of extradigital and digital glomus tumours: A retrospective comparative study. J Eur Acad Dermatol Venereol 2011;25:1392-7. [Google Scholar] [PubMed]
- 7. Villescas VV, Wasserman PL, Cunningham JC, Siddiqi AM. Brace yourself: An unusual case of knee pain, an extradigital glomangioma of the knee. Radiol Case Rep 2017;12:357-60. [Google Scholar] [PubMed]
- 8. Clark ML, O’Hara C, Dobson PJ, Smith AL. Glomus tumor and knee pain: A report of four cases. Knee 2009;16:231-4. [Google Scholar] [PubMed]
- 9. Puchala M, Kruczynski J, Szukalski J, Lianeri M. Glomangioma as a rare cause of knee pain. A report of two cases. J Bone Joint Surg Am 2008;90:2505-8. [Google Scholar] [PubMed]
- 10. Glazebrook KN, Laundre BJ, Schiefer TK, Inwards CY. Imaging features of glomus tumors. Skeletal Radiol 2011;40:855-62. [Google Scholar] [PubMed]
- 11. Christian BP. Extradigital glomus tumor of the anterior knee. Case Rep Plast Surg Hand Surg 2020;7:105-7. [Google Scholar] [PubMed]
- 12. Maxey ML, Houghton CC, Mastriani KS, Bell RM, Navarro FA, Afshari A. Large prepatellar glomangioma: A case report. Int J Surg Case Rep 2015;14:80-4. [Google Scholar] [PubMed]
- 13. Goncalves R, Lopes A, Julio C, Durao C, De Mello RA. Knee glomangioma: A rare location for a glomus tumor. Rare Tumors 2014;6:5588. [Google Scholar] [PubMed]
- 14. Akgun RC, Guler UO, Onay U. A glomus tumor anterior to the patellar tendon: A case report. Acta Orthop Traumatol Turc 2010;44:250-3. [Google Scholar] [PubMed]
- 15. El Hyaoui H, Messoudi A, Rafai M, Garch A. Unusual localization of glomus tumor of the knee. Joint Bone Spine 2016;83:213-5. [Google Scholar] [PubMed]
- 16. Souza BC, Luce MC, Sittart JA, Valente NY. Extradigital glomus tumor mimicking osteomuscular disease. An Bras Dermatol 2018;93:472-3. [Google Scholar] [PubMed]
- 17. Frumuseanu B, Balanescu R, Ulici A, Golumbeanu M, Barbu M, Orita V, et al. A new case of lower extremity glomus tumor up-to-date review and case report. J Med Life 2012;5:211-4. [Google Scholar] [PubMed]
- 18. Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW. Atypical and malignant glomus tumors: Analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am J Surg Pathol 2001;25:1-12. [Google Scholar] [PubMed]
- 19. So SY, Kim BM, Lee SY, Ko YK, Shin YS, Lee WH. Glomus tumor causing anterior thigh pain: A case report. Korean J Pain 2014;27:174-7. [Google Scholar] [PubMed]
- 20. Suprakasan A, Sudhir NU, Kudva R. A knee pain referred to a dermatologist. Clin Dermatol Rev 2024;8:154-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Congenital Absence of Bilateral Patella in an Active Military Personnel Case Report
September 1, 2025 Congenital Absence of Bilateral Patella in an Active Military Personnel Case Report August 1, 2025 Don’t Dismiss the Swelling: A Rare Case of Tenosynovial Giant Cell Tumor in a Young Woman’s Finger – A Case Report
August 1, 2025 Don’t Dismiss the Swelling: A Rare Case of Tenosynovial Giant Cell Tumor in a Young Woman’s Finger – A Case Report July 10, 2022 Rare Occurrence of Extradigital Glomangioma in the Prepatellar Bursa of a 40-Year-Old: A Case Study
July 10, 2022 Rare Occurrence of Extradigital Glomangioma in the Prepatellar Bursa of a 40-Year-Old: A Case Study July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report