
Concurrent involvement of the distal fibular epiphysis, talus, and sinus tarsi is a rare presentation of dysplasia epiphysealis hemimelica; careful clinicoradiological evaluation and complete surgical excision can result in excellent functional outcomes.
Dr. Amir Suhail, Department of Orthopaedics, All India Institute of Medical Sciences, Marudhar Industrial Area, 2nd Phase, M.I.A. 1st Phase, Basni, Jodhpur - 342 005, Rajasthan, India. E-mail: suhail.amir22@gmail.com
Abstract
Introduction: Dysplasia epiphysealis hemimelica (DEH), also known as Trevor’s disease, is a rare developmental disorder characterised by asymmetric osteochondral overgrowth arising from the epiphysis. It commonly involves the lower limb, particularly the ankle and knee, and may mimic osteochondroma both clinically and histologically.
Case Report: We report an unusual case of an 8-year-old boy presenting with pain, swelling, and progressive restriction of ankle motion. Imaging revealed osteochondral lesions arising from the distal fibular epiphysis and the inferolateral aspect of the talus extending into the sinus tarsi. Surgical excision of both lesions was performed through an anterolateral approach. Histopathological examination showed features of a benign osteochondral lesion consistent with DEH. At 12-month follow-up, the patient demonstrated near-full ankle range of motion, no recurrence, and satisfactory functional recovery.
Conclusion: Concurrent involvement of the distal fibula, talus, and sinus tarsi represents an unusual presentation of DEH. Comprehensive imaging evaluation and complete surgical excision can provide favourable functional outcomes.
Keywords: Dysplasia epiphysealis hemimelica, Trevor’s disease, ankle, sinus tarsi, osteochondral lesion, pediatric.
Dysplasia epiphysealis hemimelica (DEH), also known as Trevor’s disease, is a rare, non-hereditary developmental disorder of the epiphysis characterised by asymmetric osteochondral proliferation, typically confined to one side of an epiphysis or a comparable structure [1,2,3]. Its prevalence is estimated at approximately 1 in 1,000,000, with a male predominance of about 3:1, and most cases are identified in early childhood, usually before the age of eight, when swelling, pain, or deformity prompts clinical evaluation [4,5,6]. Fairbank introduced the currently accepted name, DEH, in 1956 [3]. The abnormal cartilage forms an irregular nodular mass located on either the medial or lateral part of the bone, with the medial side more frequently affected [5,6]. DEH may involve a single epiphysis (localised form), multiple epiphyses in one limb (classical form), or an entire limb (generalised form), most often the lower extremity from the pelvis to the foot [5,6]. Approximately two-thirds of affected children present with multiple lesions. Clinically, DEH appears as a nodular bony mass that can cause deformity, restricted motion, or recurrent sprains [6]. Histologically, the lesion resembles an osteochondroma, making radiological correlation critical for diagnosis [4,5,6]. We report an unusual case of DEH involving both the distal fibula and talus, with an outgrowth into the sinus tarsi region, highlighting the diagnostic challenges and emphasising the importance of individualised surgical management [5,7,8].
An 8-year-old boy presented to the orthopaedic clinic with a 1.5-year history of pain and swelling in the right ankle associated with progressive difficulty in walking. There was no history of trauma, fever, weight loss, or family history of joint or bone disorders. On physical examination, a firm, non-tender bony swelling was palpable anterior to the lateral malleolus. The overlying skin was normal, and there were no inflammatory signs (Fig. 1). Range of motion at the ankle and subtalar joints was restricted, and gait was limited due to discomfort. Radiographs (Fig. 2) and computed tomography (Fig. 3) of the right ankle and lower leg showed a well-defined osseous overgrowth arising from the distal fibular epiphysis, projecting anterolaterally, along with an additional irregular bony prominence arising from the inferior surface of the talus in the sinus tarsi region.

Figure 1: Pre-operative clinical photographs showing a visible bony swelling over the anterolateral aspect of the ankle (a and b). Intraoperative image demonstrating exposure of the osteochondral mass arising from the distal fibula and talus within the sinus tarsi region (c).
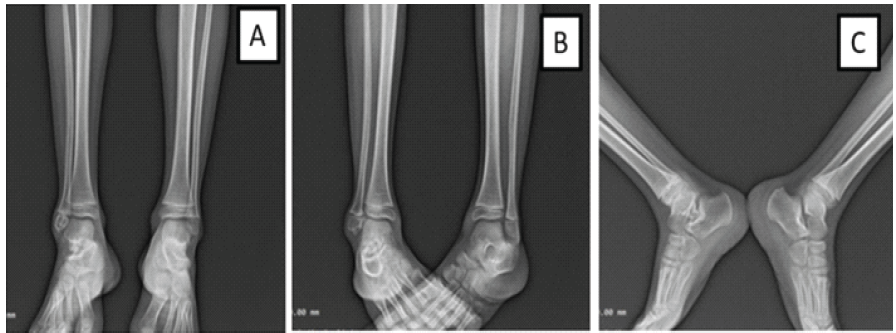
Figure 2: Pre-operative radiographs of the right ankle – Anteroposterior view showing osseous overgrowth from the distal fibular epiphysis (a), Oblique view demonstrating the extent of the lesion (b), Lateral view showing an osteochondral prominence from the talus extending into the sinus tarsi (c).
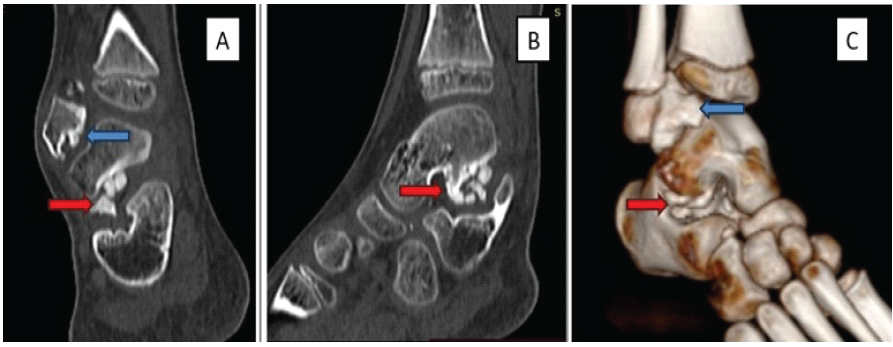
Figure 3: Computed tomography images of the right ankle – coronal (a), sagittal (b), and 3D reconstruction (c) – demonstrating irregular osteochondral overgrowth arising from the distal fibular epiphysis (blue arrow) and the inferolateral aspect of the talus projecting into the sinus tarsi (red arrows).
Magnetic resonance imaging (MRI) demonstrated lobulated osseous masses arising from the distal fibular epiphysis and from the inferolateral aspect of the talus, forming a sessile growth in the sinus tarsi region measuring approximately 1 cm in thickness and <1.5 cm in height and width. Both lesions showed cortical and medullary continuity with their parent bones. There was no cortical destruction, marrow oedema, soft-tissue invasion, or joint effusion, although the subtalar joint space was reduced (Fig. 4).
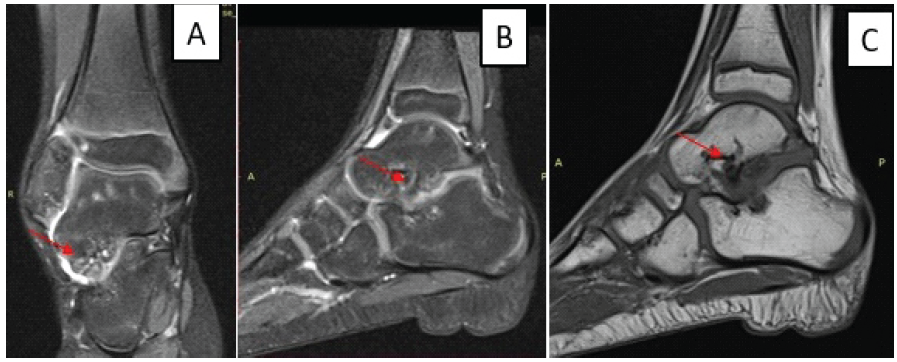
Figure 4: Magnetic resonance imaging of the right ankle. Coronal T2-weighted (a), sagittal T2-weighted (b), and sagittal T1-weighted (c) images showing a lobulated epiphyseal lesion with cartilage signal intensity.
Differential diagnoses included osteochondroma, synovial chondromatosis, intra-articular loose bodies, and epiphyseal dysplasia. The epiphyseal origin of the lesion with intra-articular extension and cortical-medullary continuity on imaging favoured the diagnosis of DEH. The patient was positioned supine under general anaesthesia with a pneumatic tourniquet applied to the thigh. Through an anterolateral approach, both lesions were exposed. Intraoperative fluoroscopy was used to localise the lesions and confirm complete excision. Careful dissection was performed to identify and protect the superficial peroneal nerve. The subtalar joint was inspected intraoperatively, and the articular cartilage was preserved as much as possible while excising the osteochondral masses. Both lesions were excised en bloc, and the raw surfaces were curetted to normal cancellous bone. Histopathological examination (Fig. 5) demonstrated mature cartilage and trabecular bone without cellular atypia. A
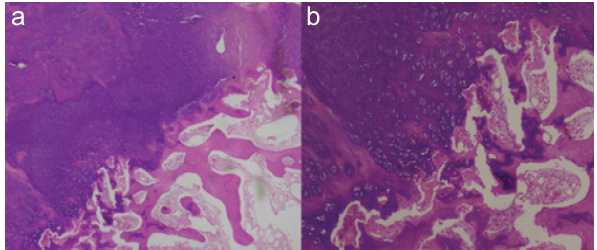
Figure 5: Histopathological examination. (a) Scanner view showing an osteochondral lesion with a cartilaginous cap overlying mature bony trabeculae (Hematoxylin and Eosin [H&E], ×40). (b) Low-power view demonstrating orderly distribution of bland chondrocytes without atypia (H&E, ×100).
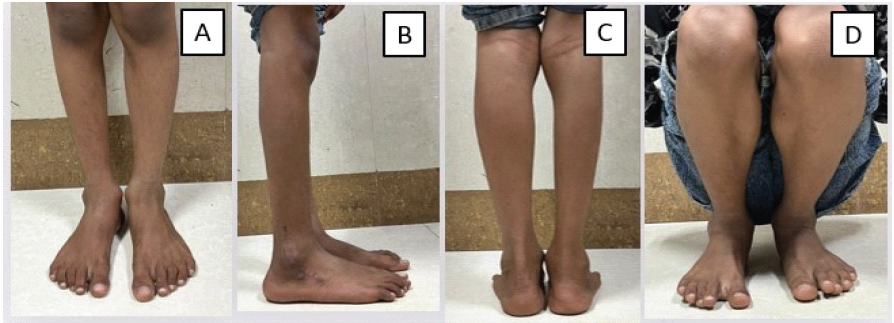
Figure 6: Post-operative clinical photographs of the ankle and foot – anterior (a), lateral (b), posterior (c), and squatting position (d) – demonstrating good functional recovery and maintained hindfoot alignment.
The American Orthopaedic Foot and Ankle Society ankle-hindfoot score was 92/100, with a Visual Analogue Scale pain score of 1/10. No limb-length discrepancy, angular deformity, progression of hindfoot malalignment, or evidence of physeal disturbance was observed during follow-up. Recurrence assessment during follow-up was performed clinically and with serial radiographs; post-operative MRI was not considered necessary because the patient remained asymptomatic with no radiographic evidence of recurrence.
DEH is an uncommon developmental disorder of the epiphysis with heterogeneous clinical presentations. Although the exact aetiology remains unclear, proposed mechanisms include abnormalities in epiphyseal cartilage proliferation during skeletal development. The condition predominantly affects the lower limb, with a predilection for the medial side; however, lateral involvement, as observed in the present case, is distinctly uncommon [1,7]. A major diagnostic challenge is distinguishing DEH from osteochondroma. Although both lesions share histological similarities, their anatomical origin is the key distinguishing factor. Osteochondromas arise from the metaphysis and are extra-articular, whereas DEH originates from the epiphysis and frequently demonstrates intra-articular extension [1,5,9]. Advanced imaging modalities, particularly MRI, are essential for assessing lesion extent and articular involvement and for pre-operative planning [9]. Azouz et al. classified DEH into three forms: localised (single epiphyseal involvement), classical (multiple epiphyses in a single limb), and generalised (entire limb involvement) [10]. Based on this classification, the present case can be categorised under the classical form, as it involves multiple epiphyses within the same anatomical region. A review of previously reported cases involving the ankle and sinus tarsi region (Table 1) demonstrates that most cases present with pain, swelling, and restricted range of motion, with the talus being the most commonly involved site [11,12,13,14,15,16,17,18,19].
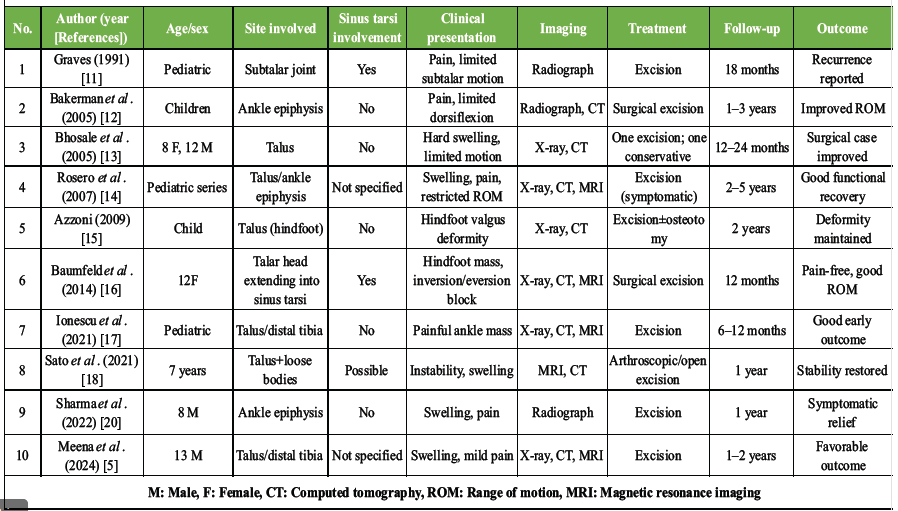
Table 1: Review of the literature on dysplasia epiphysealis hemimelica involving the ankle and sinus tarsi region
Sinus tarsi involvement is relatively rare and has been reported in only a limited number of cases, such as those described by Graves [11] and Baumfeld et al. [16]. Furthermore, most reported cases involve a single epiphysis, whereas multifocal involvement within the same joint region is uncommon. A similar unusual presentation involving multiple epiphyses in the upper limb has been reported by Kantiwal et al. [20], highlighting the spectrum of extensive disease involvement. In comparison, the present case is unique due to the simultaneous involvement of the distal fibular epiphysis and the talus with extension into the sinus tarsi. To the best of our knowledge, simultaneous involvement of the distal fibular epiphysis, talus, and sinus tarsi in DEH has rarely been reported in the literature and highlights the importance of comprehensive imaging evaluation to identify multifocal disease. Management strategies are guided by symptom severity and functional limitation. Asymptomatic lesions may be managed conservatively with observation [5,7]. However, symptomatic cases require surgical excision, particularly in the presence of pain, deformity, or joint dysfunction [2,5,19,21]. A literature review suggests that surgical excision generally results in good functional outcomes, although recurrence has been reported, especially in skeletally immature patients [11,22,23]. In our case, complete excision resulted in excellent functional recovery without recurrence at 12 months. Arthroscopic excision was not preferred because the lesion involved both the distal fibular epiphysis and the sinus tarsi region, requiring wider exposure for complete excision and adequate protection of surrounding neurovascular and soft-tissue structures. Despite its benign nature, DEH carries a risk of recurrence due to persistent epiphyseal activity in growing children [5,22,23]. Although no recurrence was observed at 12-month follow-up, the patient has been advised periodic long-term clinical and radiological surveillance until skeletal maturity to monitor for recurrence, physeal disturbance, deformity progression, or secondary degenerative changes. This case expands the existing spectrum of DEH by demonstrating concurrent multiepiphyseal involvement within the ankle joint, which has rarely been reported.
DEH is a rare epiphyseal disorder that can present with atypical multi-site involvement, as seen in this case, affecting both the distal fibula and talus with sinus tarsi extension. Differentiation from osteochondroma is essential and relies on clinicoradiological correlation. Symptomatic lesions require surgical excision to relieve pain and restore joint function. Careful resection with preservation of joint congruity results in favourable outcomes; however, long-term follow-up is necessary due to the risk of recurrence in skeletally immature patients.
Dysplasia epiphysealis hemimelica should be considered in children presenting with epiphyseal osteochondral lesions around the ankle. Unusual involvement of both the distal fibula and talus with sinus tarsi extension can occur. Early surgical excision in symptomatic cases provides excellent functional recovery and prevents long-term joint dysfunction.
References
- 1. Mouchet A, Belot J. Tarsomegalie. J Radiol Electrol 1926;10:1-8. [Google Scholar] [PubMed]
- 2. Trevor D. Tarso-epiphysial aclasis; A congenital error of epiphysial development. J Bone Joint Surg Br 1950;32-B:204-13. [Google Scholar] [PubMed]
- 3. Fairbank TJ. Dysplasia epiphysealis hemimelica (tarso-epiphysial aclasis). J Bone Joint Surg Br 1956;38-B:237-57. [Google Scholar] [PubMed]
- 4. Abd Ghani F, Sridharan R, Mohd Zaki F, Md Zain RR, Ibrahim S. Dysplasia epiphysealis hemimelica (Trevor-Fairbank disease): A case report. Hong Kong J Radiol 2019;22:e9-13. [Google Scholar] [PubMed]
- 5. Meena DS, Saini S, Sehrawat M, Yadav V, Kumar P. Dysplasia epiphysealis hemimelica (Trevor’s Disease) of talus treated with excision, periosteal flap, and open wedge osteotomy: A case report and review of literature. J Limb Lengthen Reconstr 2024;10:3-10. [Google Scholar] [PubMed]
- 6. Asha ML, Nagaraj BN, Kumar GA, Ashok ML. Dysplasia epiphysealis hemimelica (Trevor’s Disease): A rare case report with oral manifestations. Int J Res Med Sci 2015;3:1018-24. [Google Scholar] [PubMed]
- 7. Vogel T, Skuban T, Kirchhoff C, Baur-Melnyk A, Siegert S, Heimkes B. Dysplasia epiphysealis hemimelica of the distal ulna: A case report and review of the literature. Eur J Med Res 2009;14:272-6. [Google Scholar] [PubMed]
- 8. Assan BR, Chafaaoui H, Ahyee D, Janoyer M, Tolg C. Trevor’s disease of the wrist: A case report and literature review. J Orthop Rep 2024;3:100330. [Google Scholar] [PubMed]
- 9. Tyler PA, Rajeswaran G, Saifuddin A. Imaging of dysplasia epiphysealis hemimelica (Trevor’s Disease). Clin Radiol 2013;68:415-21. [Google Scholar] [PubMed]
- 10. Azouz EM, Slomic AM, Marton D, Rigault P, Finidori G. The variable manifestations of dysplasia epiphysealis hemimelica. Pediatr Radiol 1985;15:44-9. [Google Scholar] [PubMed]
- 11. Graves ML. Dysplasia epiphysealis hemimelica of the subtalar joint: A case report. Foot Ankle 1991;12:45-9. [Google Scholar] [PubMed]
- 12. Bakerman KA, Letts RM, Lawton L. Dysplasia epiphysealis hemimelica of the ankle. Foot Ankle Int 2005;26:580-4. [Google Scholar] [PubMed]
- 13. Bhosale PB, Jabbar AA, Muir LT. Dysplasia epiphysealis hemimelica of the talus: Two case reports. J Pediatr Orthop B 2005;14:423-7. [Google Scholar] [PubMed]
- 14. Rosero VM, Kiss S, Terebessy T, Köllö K, Szöke G. Dysplasia epiphysealis hemimelica (Trevor’s disease): 7 of our own cases and a review of the literature. Acta Orthop 2007;78:856-61. [Google Scholar] [PubMed]
- 15. Azzoni R. Dysplasia epiphysealis hemimelica of the talus. J Orthop Traumatol 2009;10:43-6. [Google Scholar] [PubMed]
- 16. Baumfeld D, Baumfeld T, Rocha RL. Trevor’s disease of the talus occupying the sinus tarsi. Case Rep Orthop 2014;2014:1-4. [Google Scholar] [PubMed]
- 17. Ionescu AM, Popescu B, Neagu O, Carp M, Tevanov I, Balanescu L, et al. Dysplasia epiphysealis hemimelica (Trevor’s Disease) in children, Two new cases: Diagnosis, treatment, and literature review. Children (Basel) 2021;8:907. [Google Scholar] [PubMed]
- 18. Sato T. Dysplasia epiphysealis hemimelica of the talus with intra-articular loose bodies: A case report. Case Rep Orthop 2021;2021:1-5. [Google Scholar] [PubMed]
- 19. Koshire S, Sarukte V, Aher G. A symptomatic Swollen ankle in an 8-year-old male child – a rare case report of dysplasia epiphysealis hemimelica. J Orthop Case Rep 2022;12:52-5. [Google Scholar] [PubMed]
- 20. Kantiwal P, Chawla S, Suhail A, Kumar Yadav S, Rao M. Exceptionally extensive Trevor’s disease involving all four radial carpals presenting with gross wrist deformity. Cureus 2026;18:e101327. [Google Scholar] [PubMed]
- 21. Dhillon MS, Dhillon M, Patel S, Sharma S. A lumpy-bumpy painful ankle-Trevor disease of the ankle in a 9-year-old. J Orthop Case Rep 2022;12:26-9. [Google Scholar] [PubMed]
- 22. Ouyang Z, Xu M, Li X, Peng D. Dysplasia epiphysealis hemimelica with involvement of the distal tibial epiphysis and talus: Recurrence of a case and literature review. J Foot Ankle Surg 2014;53:199-202. [Google Scholar] [PubMed]
- 23. Bahk WJ, Lee HY, Kang YK, Park JM, Chun KA, Chung YG. Dysplasia epiphysealis hemimelica: Radiographic and magnetic resonance imaging features and clinical outcome of complete and incomplete resection. Skeletal Radiol 2010;39:85-90. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 September 10, 2022 A Lumpy-Bumpy Painful Ankle – Trevor Disease of the Ankle in a 9-year-old
September 10, 2022 A Lumpy-Bumpy Painful Ankle – Trevor Disease of the Ankle in a 9-year-old July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report
May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series