
Recurrent multilevel calcified lumbar disc herniation may require spinal fusion when repeated decompression and discectomy fail to prevent recurrence.
Dr. Shinji Kotaka, Orthopaedic and Microscopic Spine and Spinal Cord Surgery Center, Hiroshima City North Medical Center Asa Citizens Hospital, Hiroshima, Japan. E-mail: kotaka_shinji1216@yahoo.co.jp
Abstract
Introduction: Calcified lumbar disc herniation (LDH) is a rare subtype of LDH, and recurrent multilevel presentations in adults have not been reported. Its optimal management remains unclear, especially in cases resistant to standard decompression and discectomy.
Case Report: A 58-year-old woman presented with a 6-month history of bilateral lower extremity pain, numbness, and intermittent claudication, with walking limited to 10–20 m. Magnetic resonance imaging revealed L4/5 spinal canal stenosis without evidence of disc calcification on computed tomography. Posterior decompression at L4/5 resulted in significant symptom improvement. Two years later, right leg pain developed after a fall, and imaging confirmed a calcified disc herniation at L3/4 compressing the L4 nerve root. Discectomy provided complete relief. Three months later, a calcified herniation at L5/S1 extended bilaterally, compressing both S1 nerve roots. Discectomy was performed, and histopathology confirmed calcium pyrophosphate dihydrate deposition. One month later, recurrent bilateral symptoms occurred, with imaging revealing a new calcified herniation at L2/3 and a persistent fluid-filled herniation sac at L5/S1. Surgical treatment relieved the L2/3 lesion but not the L5/S1 findings. Subsequent recurrence at L1/2 prompted staged spinal fusion: lateral lumbar interbody fusion from L2/3 to L4/5, followed by posterior fusion from T10 to the pelvis. At 1-year follow-up, no new herniations were observed, and symptoms remained controlled.
Conclusion: Recurrent multilevel calcified lumbar disc herniation is exceptionally rare and may be refractory to conventional decompression and discectomy. In such cases, extensive spinal fusion can be an effective strategy to prevent recurrence and achieve long-term symptom resolution.
Keywords: Calcified lumbar disc herniation, multilevel herniation, recurrent herniation, and spinal fusion.
Lumbar disc herniation (LDH) is one of the most common degenerative intervertebral disc diseases. Although there remains little consensus regarding the optimal treatment for symptomatic LDH, both surgical and non-surgical interventions can yield favourable outcomes in appropriately selected patients [1,2]. Calcified lumbar disc herniation (CLDH) is a rare subtype of LDH characterised by calcification at the site of herniation. At present, there is no established treatment standard for CLDH. Some studies indicate conservative treatment may be effective even for symptomatic cases, while others recommend early surgical decompression due to potential symptom progression. Therefore, indications for surgical intervention remain controversial [3]. Previous reports have demonstrated favourable outcomes with posterior decompression (with discectomy when indicated) using endoscopic or microscopic techniques for CLDH [4,5]. However, all of these cases involve single-level CLDH, and no cases of multilevel or recurrent CLDH have been reported to date. The uniqueness of the present case lies in multiple, independently occurring calcified disc herniations. Herein, we describe a unique case of recurrent multilevel CLDH successfully managed by lumbar spinal fusion.
A 58-year-old Asian female presented to our clinic with a 6-month history of bilateral lower extremity pain, numbness, and intermittent claudication. Symptoms were localized to the posterolateral aspects of both legs, limiting her walking distance to 10–20 m. Neurological examination revealed diminished bilateral lower limb tendon reflexes without obvious muscle weakness, and straight leg-raising tests were negative. Magnetic resonance imaging (MRI) showed spinal canal stenosis at L4/5, while computed tomography (CT) revealed no evident disc calcification (Fig. 1a, b, c).
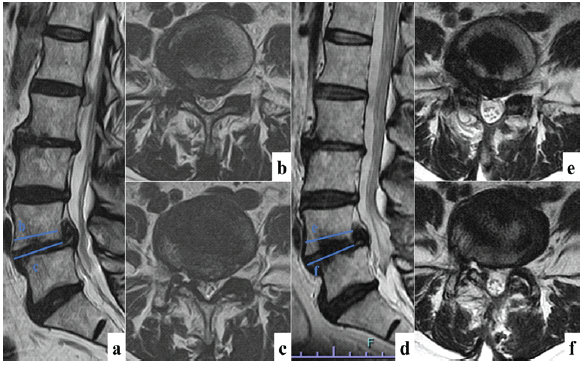
Figure 1: Pre- and post-operative Magnetic resonance imaging (MRI) findings of L4-5 spinal canal stenosis treated with decompression. MRI (a) sagittal image, (b and c) axial image demonstrated a spinal canal stenosis of L4-5 level. Post-operative MRI (d) sagittal image, (e and f) axial image demonstrated spinal canal decompression was obtained.
Following unsuccessful conservative treatment, posterior decompression at L4/5 was performed, resulting in significant symptom relief postoperatively. Adequate decompression was confirmed by post-operative MRI (Fig. 1d, e, f). Two years after initial surgery, the patient developed right lower extremity pain following a fall. Imaging studies identified a disc herniation at the right L3/4 level compressing the L4 nerve root (Figs. 2a, b, c). Discectomy provided complete symptom resolution, confirmed by post-operative MRI (Fig. 2d, e, f).
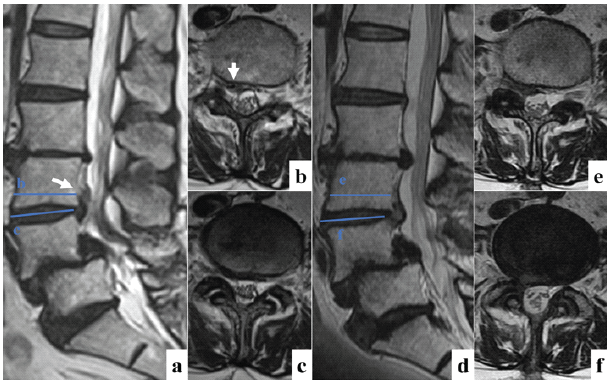
Figure 2: Pre- and post-operative Magnetic resonance imaging (MRI) findings of L3-4 upper lumbar disk herniation treated with discectomy. MRI (a) sagittal image, (b and c) axial image demonstrated upper disk herniation at the L3-L4 level. The arrows are pointing to an upper lumbar disk herniation. Post-operative MRI (d) sagittal image, (e and f) axial image demonstrated that all herniated disk fragments had disappeared.
Three months post-second surgery, the patient experienced new-onset left leg pain progressing to bilateral involvement. CT and MRI revealed another calcified herniation extending from the right side of L5/S1 to the left at the S1 vertebral level, compressing bilateral S1 nerve roots (Fig. 3a, b, c, d, e, f). Surgical discectomy removed calcified fragments, and histopathology confirmed calcium pyrophosphate dihydrate deposition (Fig. 3g and h). Post-operative MRI showed fluid accumulation within the disc herniation sac, compressing nerve roots (Figs. 3i, j, k).
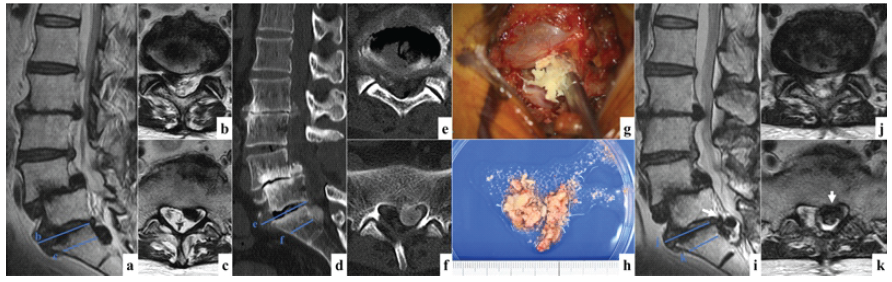
Figure 3: Pre- and post-operative image and intraoperative micrographs findings of L5-S1 disk herniation treated with discectomy. Magnetic resonance imaging (MRI) (a) sagittal image, (b and c) axial image demonstrated disk herniation extending from the right side of L5-S1 to the left at the S1 vertebral level. Computed tomography (d) sagittal image, (e and f) axial image showed calcification in the herniated mass. (g) Intraoperative micrographs showing that a calcified herniated mass was presented between the right S1 nerve root and dura. (h) Macroscopic findings of the herniated mass revealed a calcium-rich degenerative disk herniation. Post-operative MRI (i) sagittal image, (j and k) axial image showed fluid accumulation within the disk herniation sac, compressing S1 nerve roots. The arrows are pointing to the disk herniation sac with fluid.
One month later, the patient developed bilateral leg pain and numbness again. Imaging studies revealed a new calcified herniation at L2/3 (left side) and a persistent fluid-filled herniation sac at L5/S1 (Fig. 4a, b, c, d, e, f, g, h, i, j). Discectomy at L2/3 and partial capsule removal at L5/S1 yielded no symptom improvement (Figs. 4k and l). MRI confirmed herniation resolution at L2/3 but persistence of a reduced fluid-filled sac at L5/S1 (Fig. 4m, n, o).
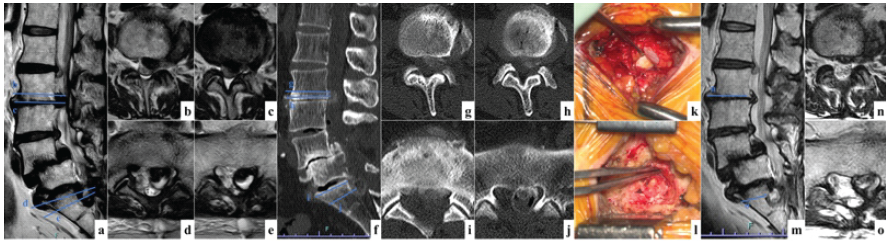
Figure 4: Pre- and post-operative image and intraoperative micrographs findings of L2-3 and L5-S1 disk herniation. Magnetic resonance imaging (MRI) (a) sagittal image, (b, c, d, and e) axial image) demonstrated disk herniation at L2-3 (b and c) and fluid-filled herniation sac at L5-S1 (d and e). Computed tomography (f) sagittal image, (g, h, i, and j) axial image showed calcification in the herniated mass at both levels. (k and l) Intraoperative micrographs at the L2-3 level showed a calcified herniated mass lateral to the left L3 nerve root, with a heavily calcified herniated area inside. Post-operative MRI (m) sagittal image, (n and o) axial image confirmed herniation resolution at L2-3 but persistence of a reduced fluid-filled sac at L5-S.
Post-operative symptoms fluctuated, and subsequent MRI revealed another new calcified herniation at L1/2 extending centrally (Fig. 5a, b, c, d, e, f). Anticipating recurrence with discectomy alone, we proceeded with spinal fusion: lateral lumbar interbody fusion from L2/3 to L4/5, followed 1 week later by posterior fusion from pelvis to T10 (Figs. 5g and h).
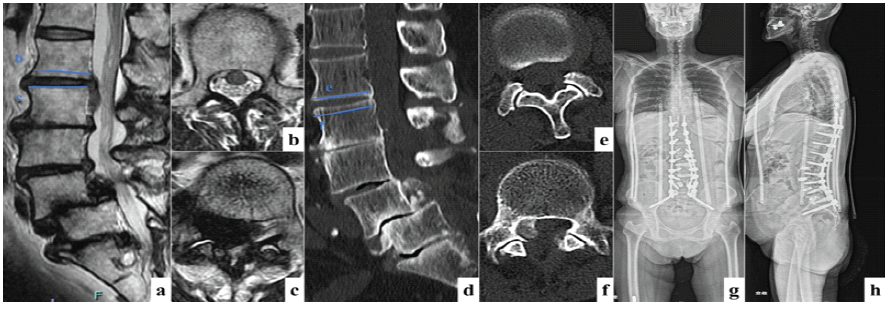
Figure 5: Preoperative image findings of L1/2 and post-operative extensive spinal fusion. Magnetic resonance imaging (a) sagittal image, (b and c) axial image demonstrated disk herniation extending from the center to the right at the L1-2 level. Computed tomography (d) sagittal image, (e and f) axial image showed calcification in the herniated mass. Post-operative X-ray images (g) P-A, (h) lateral showed spinal fusion from T10 to pelvis performed to avoid the recurrence of disk herniation. Lateral interbody fusion at L2-3, L3-4, and L4/5, transforaminal lumbar interbody fusion at L5-S1, pedicle screws placed from T10 to S1, and an S2 alar-iliac screw placed in the pelvis were used for posterior fixation.
Extensive combined anterior and posterior spinal fusion was intentionally performed in a staged manner, as previous studies have suggested that staged long-segment fusion may reduce surgical invasiveness and perioperative burden compared with single-stage surgery [6]. At the 1-year follow-up, no further herniations occurred, and the patient remains clinically stable.
Adult CLDH, as demonstrated by this case, is notably rare. No previous reports have documented multiple, independently occurring calcified herniations at several lumbar levels. CLDH is characterised by calcification within the herniated material, although its exact prevalence remains unclear [7]. Its pathophysiology is poorly understood, with suggested origins including intervertebral disc calcification (IDC) and calcification of herniated disc fragments [8]. IDC typically involves calcification within the intervertebral disc space, reported in 5–6% of adults on conventional radiography [9,10,11]. IDC is easily identified via characteristic CT imaging findings [12]. Pathogenesis of IDC has been associated with disc degeneration. Shao et al. identified osteogenic markers (BMP-2, Osterix, and osteocalcin) in degenerated discs, suggesting a potential link [13]. IDC-associated herniations often show a distinctive “tail sign” on CT imaging, characterised by calcification extending continuously from the disc space into the spinal canal [14]. However, our patient lacked this sign, suggesting secondary calcification within nucleus pulposus fragments post-herniation. Previous studies attribute calcification to chronic disc herniation (>6 months’ duration), prolonged use of Traditional Chinese Medicine (TCM), developmental changes, or unidentified factors (infection or microtrauma) [4,15]. Infectious discitis was considered as a differential diagnosis; however, laboratory investigations showed no evidence of infection, and histopathological examination revealed calcium pyrophosphate dihydrate deposition without inflammatory changes. Nevertheless, our patient’s short symptomatic period and absence of TCM use leave the cause unresolved. This case’s distinctiveness lies in recurrent, multilevel independent CLDH events, ultimately managed effectively through spinal fusion. Literature typically reports good outcomes following posterior decompression and discectomy for single-level CLDH without recurrence [5]. However, our case indicates that conventional approaches may prove insufficient for recurrent multilevel cases, warranting consideration of spinal fusion to achieve symptom resolution and prevent further recurrence. At our institution, spinal fusion is not routinely performed, even in cases of degenerative spondylolisthesis with instability. Therefore, fixation was not planned during the index surgery, and decompression alone was selected according to our standard treatment strategy.
Recurrent multilevel CLDH is extremely rare. This case demonstrates that when repeated decompression and discectomy fail to prevent recurrence, lumbar spinal fusion should be considered to achieve long-term stability and symptom resolution.
Recurrent multilevel CLDH is rare and may not respond to repeated decompression or discectomy; spinal fusion should be considered to achieve durable symptom relief and prevent further recurrence.
References
- 1. Larequi-Lauber T, Vader JP, Burnand B, Brook RH, Kosecoff J, Sloutskis D, et al. Appropriateness of indications for surgery of lumbar disc hernia and spinal stenosis. Spine (Phila., Pa., 1976) 1997;22:203-9. [Google Scholar] [PubMed]
- 2. Gibson JN, Grant IC, Waddell G. The Cochrane review of surgery for lumbar disc prolapse and degenerative lumbar spondylosis. Spine (Phila., Pa., 1976) 1999;24:1820-32. [Google Scholar] [PubMed]
- 3. Xu N, Wei F, Liu X, Jiang L, Liu Z. Calcific discitis with giant thoracic disc herniations in adults. Eur Spine J 2016;25:204-8. [Google Scholar] [PubMed]
- 4. Dabo X, Ziqiang C, Yinchuan Z, Haijian N, Kai C, Yanbin L, et al. The clinical results of percutaneous endoscopic interlaminar discectomy (PEID) in the treatment of calcified lumbar disc herniation: A case-control study. Pain Physician 2016;19:69-76. [Google Scholar] [PubMed]
- 5. Wang H, Zhou T, Gu Y, Yan Z. Evaluation of efficacy and safety of percutaneous transforaminal endoscopic surgery (PTES) for surgical treatment of calcified lumbar disc herniation: A retrospective cohort study of 101 patients. BMC Musculoskelet Disord 2021;22:65. [Google Scholar] [PubMed]
- 6. Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Staged posterior and anterior spinal fusion for adult spinal deformity. Spine (Phila., Pa. 1976) 2006;31:242-8. [Google Scholar] [PubMed]
- 7. Yang Q, Xu HW, Hurday S, Xu BS. Construction strategy and progress of whole intervertebral disc tissue engineering. Orthop Surg 2016;8:11-8. [Google Scholar] [PubMed]
- 8. Paolini S, Ciappetta P, Guiducci A, Principi M, Missori P, Delfini R. Foraminal deposition of calcium pyrophosphate dihydrate crystals in the thoracic spine: Possible relationship with disc herniation and implications for surgical planning. Report of two cases. J Neurosurg Spine 2005;2:75-8. [Google Scholar] [PubMed]
- 9. Weinberger A, Myers AR. Intervertebral disc calcification in adults: A review. Semin Arthritis Rheum 1978;8:69-75. [Google Scholar] [PubMed]
- 10. Cohen JA, Abraham E. The calcified intervertebral disc. A non-specific roentgenologic sign. J Med Soc N J 1973;70:459-60. [Google Scholar] [PubMed]
- 11. Bywaters EG, Hamilton EB, Williams R. The spine in idiopathic haemochromatosis. Ann Rheum Dis 1971;30:453-65. [Google Scholar] [PubMed]
- 12. Al Qaraghli MI, De Jesus O. Lumbar Disc Herniation. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560878. Accessed June 18, 2026. [Google Scholar] [PubMed]
- 13. Shao J, Yu M, Jiang L, Wei F, Wu F, Liu Z, et al. Differences in calcification and osteogenic potential of herniated discs according to the severity of degeneration based on Pfirrmann grade: A cross-sectional study. BMC Musculoskelet Disord 2016;17:191. [Google Scholar] [PubMed]
- 14. Chen J, Huang K, Dai S, Chen Y, Xu W, Fang X. Lumbar intervertebral disc calcification with massive herniation: A case report. J Int Med Res 2025;53:. [Google Scholar] [PubMed]
- 15. Jasper GP, Francisco GM, Telfeian AE. Clinical success of transforaminal endoscopic discectomy with foraminotomy: A retrospective evaluation. Clin Neurol Neurosurg 2013;115:1961-5. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report
May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report April 10, 2024 Concomitant Cement Spacer and Peri-spacer Fractures Seven Years After First-stage Revision Knee Arthroplasty: A Case Report
April 10, 2024 Concomitant Cement Spacer and Peri-spacer Fractures Seven Years After First-stage Revision Knee Arthroplasty: A Case Report March 10, 2024 Pediatric Synovial Osteochondromatosis of the Knee with Leg Length Discrepancy: A Case Report
March 10, 2024 Pediatric Synovial Osteochondromatosis of the Knee with Leg Length Discrepancy: A Case Report October 28, 2014 Auto Bone Banking: Innovative Method for Bone Preservation
October 28, 2014 Auto Bone Banking: Innovative Method for Bone Preservation