
Chronic patellar tendonitis predisposes not only to bilateral tendon injury but also may increase the risk of concomitant ligamentous injury elsewhere in the lower extremity.
Dr. Mason Poffenbarger, HCA Medical City Healthcare UNT-TCU GME (Denton) Program, Denton, Texas, US. E-mail: mason.poffenbarger@medicalcityhealth.com
Abstract
Introduction: Bilateral patellar tendon injuries are rare, with few case reports in the current literature. To the authors’ knowledge, this is the first instance of reported bilateral patellar tendon injury with concomitant syndesmotic injury.
Case Report: A 35-year-old African American male presented for evaluation of bilateral knee pain and ankle pain with inability to bear weight after an injury during a recreational football game. He was diagnosed with bilateral patellar tendon ruptures and a right-sided syndesmotic ankle injury resulting in mortise instability. He was taken for a fluoroscopic ankle examination under anaesthesia and operative repair of his injuries after appropriate imaging was obtained. After repair, he was allowed to weight-bear on the left lower extremity but kept non-weight-bearing on the right, with both knees maintained locked in extension.
Conclusion: This case report demonstrates bilateral patellar tendon injury in the setting of chronic patellar tendonitis with an associated ankle syndesmosis disruption. We suggest that a heightened index of suspicion for additional ligamentous injuries should accompany the evaluation of these patients with a low threshold for advanced imaging or fluoroscopic examination under anaesthesia.
Keywords: Patellar tendon, syndesmosis, tendonitis, ankle instability.
Simultaneous bilateral patellar tendon (aka patellar ligament) rupture is a rare injury with few cases reported in the current literature [1,2,3,4]. Unilateral injury to the extensor mechanism is often associated with trauma or may occur spontaneously in the setting of chronic disease or tendon degeneration [5,6,7]. A recent meta-analysis was only able to identify 45 individual reports consisting of 90 ruptured patellar tendons for review [4]. The method of repair and post-operative rehabilitation protocols are not standardised, and several different methods of suture and anchor fixation have been described. No specific repair technique is known to be superior for immediate and long-term healing [4,5]. Post-operative rehabilitation protocols vary widely from strict non-weight-bearing; weight-bearing with the affected knee locked in extension; early limited range of motion (before 6 weeks postoperatively); and delayed range of motion (6 or more weeks postoperatively) [4,5,8].
History:
A 35-year-old male presented with bilateral knee pain and right ankle pain after an injury during a recreational football game. He was hit while jumping up for a pass and felt pain in both knees after landing. He denied a history of prior surgery to either knee, chronic medical problems, knee pain or instability, and chronic medication use.
Exam:
On physical examination, he was unable to perform a straight leg raise bilaterally. Tenderness to palpation was present over the inferior aspect of the bilateral patellae. Ankle examination revealed moderate oedema and tenderness to palpation. Sensation was intact throughout the bilateral lower extremities. Extremities were warm and appeared well perfused, with distal pulses symmetric. Laboratory workup was unremarkable.
Imaging:
X-rays of the bilateral knees demonstrated patella alta, patellar tendon calcifications, and mild varus deformity of the proximal tibia (Fig. 1). Images obtained of the right ankle demonstrated medial clear space widening (Fig. 2).
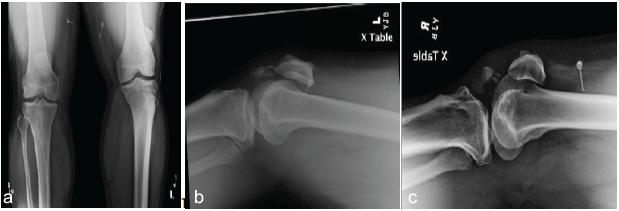
Figure 1: Anteroposterior and Lateral X-rays of bilateral knees. Patella alta of the left knee and varus deformity of the proximal left tibia, and mild-to-moderate degenerative changes of the right, resulting in medial tibiofemoral joint narrowing. Lateral X-rays of the left and right knees demonstrating peri-patellar and intra-tendinous calcifications consistent with chronic patellar tendonitis.
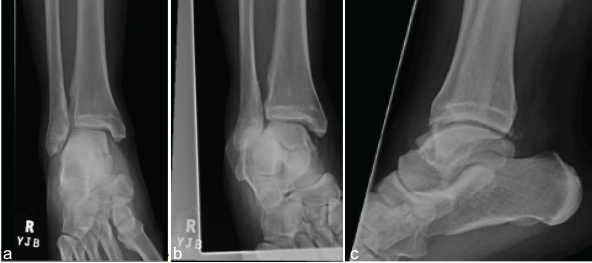
Figure 2: Anteroposterior (AP), mortise, and lateral radiographs of the right ankle obtained in the Emergency Department. Widening of the medial clear space noted on both AP and mortise views. Lucency in the medial talar body concerning for fracture. Calcification versus avulsion inferior to the medial malleolus that may be indicative of a deep deltoid ligament tear. Likely chronic calcifications posterior to the tibiotalar joint versus acute capsular avulsions.
Computed tomography (CT) was obtained to evaluate for occult fractures of the patellae, tibial plateau, and tibial plafond. Magnetic resonance imaging (MRI) studies of the same were also obtained to evaluate for intra-articular pathology that may require acute or staged treatment. CT of the bilateral knees demonstrated chronic patellar ligament changes, patella alta, and no acute fractures. CT of the ankles revealed syndesmotic asymmetry, calcification in the region of the right anterior deltoid ligament, and no acute fracture. MRI of the bilateral knees showed bilateral patellar tendon ruptures and patellar enthesopathy (Fig. 3). An MRI of the right ankle had findings of acute syndesmotic injury, sprain of the deltoid and spring ligaments, and lateral ankle ligamentous injury (Fig. 4).
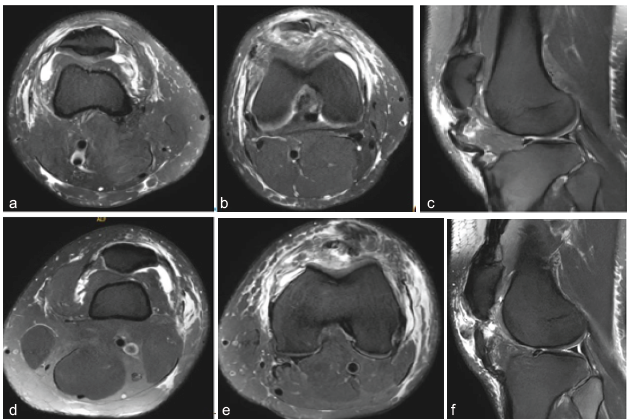
Figure 3: Magnetic resonance imaging (MRI) of the bilateral knees. (a, b, c) demonstrate right knee representative images depicting medial and lateral retinacular disruption and effusion. Sagittal image shows rupture of the patellar tendon approximately 1cm distal to the inferior patellar pole. (d, e, f) demonstrate representative images from MRI of the left knee showing medial and lateral retinacular injury with associated edema and joint effusion, and patellar tendon rupture approximately 5–15 mm distal to the inferior patellar pole.
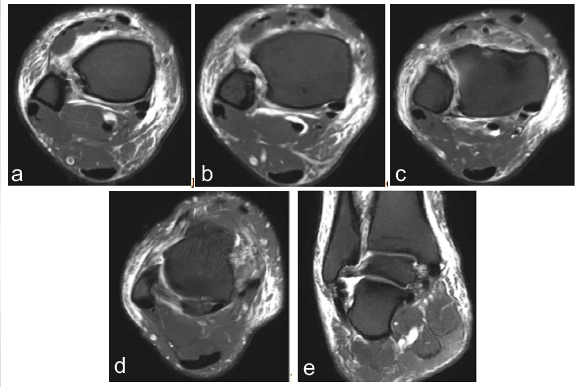
Figure 4: Magnetic resonance imaging of the right ankle. (a, b, c) demonstrate attenuated anterior inferior tibiofibular ligament with syndesmotic edema. (d) Demonstrating tearing of the anterior talofibular ligament. (e) Demonstrating sprain of deltoid and spring ligaments as well as injury to the calcaneofibular ligament.
Operative technique:
The left knee was addressed first to provide a stable limb for weight-bearing, and transfers should the need arise to abort the case before addressing all injuries. A midline anterior approach was made to the left knee. There was an avulsion of the patellar tendon with a thin fragment from the inferior pole of the patella. The avulsed fragment was not large enough to reliably accept internal fixation. Two FiberTape (Arthrex Inc.; Naples, FL) sutures were run in Krakow fashion up and down the patellar tendon for four limbs of suture exiting the superior aspect of the tendon. Next, 3 ACL guidewires were placed through the patella from inferior to superior and parallel to one another (Fig. 5).
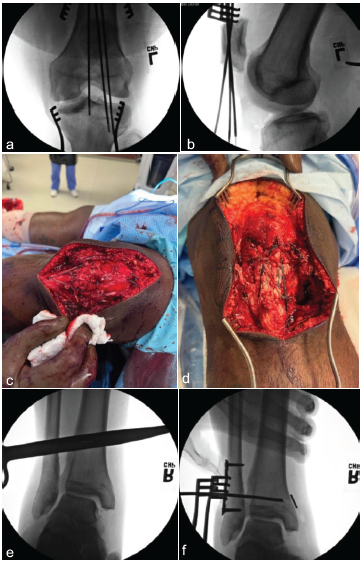
Figure 5: Fluoroscopic and clinical intraoperative images of bilateral knees and right ankle. (a) Demonstrates three longitudinal wires in the left patella for suture passage. (b) Demonstrates left knee final patellar tendon repair, including Internal Brace. (c) Demonstrates the final right patellar tendon repair with suture anchor reinforcement in the patella (Fiber Tack) and tibia (Swivelock). (d) Demonstrates external rotation stress view on mortise, demonstrating widening of the tibiofibular clear space as well as the medial clear space. (e) Demonstrates clear space between the medial button and the tibial cortex, indicative of interposed soft tissue. (g) Demonstrates removal of medial soft tissue interposed between the suture button and medial distal tibial cortex through a mini-open approach. (h) Demonstrates repeat external rotation stress view on Mortise after syndesmotic fixation with suture device, and lateral plate demonstrates stability with appropriate tibiofibular clear space, tibiofibular overlap, and medial clear space. (i) Demonstrates a lateral view confirming appropriate implant placement as well as anterior-posterior stability of the fibula in relation to the tibia during live fluoroscopic Cotton Test.
The suture was then passed through the patella using these guidewires (2 tails in the centre guidewire, 1 in each of the medial and lateral guidewires). The tails were then tied down over a bone bridge on the superior patella. The suture was tied with the knee in slight hyperextension. The knee could be passively flexed to 60 degrees without a sign of repair failure. As this would be his only weight-bearing side for the immediate post-operative period, Internal Brace (Arthrex Inc., Naples, FL) augmentation was performed. This was accomplished by passing a suture tape through the quadriceps tendon as close to the superior patellar pole as possible and securing it to the tibial tubercle with a 4.75 mm SwiveLock (Arthrex Inc., Naples, FL) anchor with the knee in approximately 45° of flexion (Fig. 5). Patellar position and alignment were confirmed fluoroscopically, and the retinaculum was repaired, followed by wound closure. As with the left knee, the right leg was then gravity exsanguinated and the tourniquet inflated to 250 mmHg, and an approach was made. The patellar tendon was found to have a midsubstance rupture, with a few fibres appearing to remain intact. This tear was repaired in end-to-end fashion using 2 separate FiberTapes (Arthrex Inc., Naples, FL). The tissue was well reapproximated by this repair, but given the chronic tendinosis and degeneration of this tissue, the decision was made to augment the repair with reinforcement via suture anchors. Two FiberTak (Arthrex Inc., Naples, FL) anchors were placed into the inferior pole of the patella, and the preloaded sutures were run in Krakow fashion into the patellar tendon. Pre-loaded Fibertapes were then crossed from each anchor and taken to two 4.75 mm SwiveLock anchors, one medial and one lateral to the tibial tubercle (Suture Bridge technique). These were tensioned with the knee in approximately 45° of flexion (Fig. 5). Patellar position and alignment were confirmed fluoroscopically; the wound was irrigated; the tourniquet was deflated and appropriate haemostasis achieved; the retinaculum was repaired; and the wound was closed. The ankle was then examined under fluoroscopy and found to be unstable, as demonstrated by increased tibiofibular clear space and medial clear space on external rotation stress exam (Fig. 5). The fibula remained axially stable with no proximal fibula fracture. A direct lateral approach to the fibula was made, and a 1/3 tubular plate was applied and affixed to the distal fibula. Quadricortical drilling was performed, and a TightRope XP (Arthrex Inc., Naples, FL) was placed approximately 1.5 cm proximal to the tibial plafond, running parallel to the joint line. Clear space was noted between the suture button and the medial tibial cortex on fluoroscopic imaging, and a small incision was made medially to remove medial tissue to allow the button to rest directly on bone (Fig. 5). Repeat external rotation stress and the Cotton stress test in AP and lateral planes were performed after fixation and demonstrated a stable ankle mortise (Fig. 5). Bilateral knee immobilisers were placed, and a constrained ankle-motion boot was applied to the right leg.
Post-operative follow-up:
The patient was made non-weight-bearing on the right leg and weight-bearing as tolerated on the left leg. An PT/OT evaluation was performed, and he participated in therapy while inpatient and was ultimately discharged home. He was allowed to begin ankle range of motion exercises at 2 weeks while non-weight-bearing. At his 6-week post-operative visit, he was ambulatory with a walker with bilateral knee immobilisers and allowed to progress to full range of motion with weight-bearing as tolerated on both legs. At 10 weeks postoperatively, examination revealed 0–80° of flexion in the left knee and 0–90° in the right knee. The right ankle was found to have dorsiflexion just beyond neutral. X-rays obtained at that time demonstrated bilateral patellae and ankle mortises in anatomical position and alignment (Fig. 6). He was encouraged to continue weight-bearing and working with physical therapy to regain motion and strength in the bilateral lower extremities.
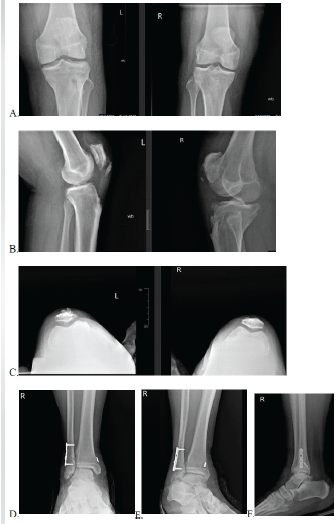
Figure 6: Ten-week post-operative weight-bearing X-rays. (a, b, and c demonstrate Anteroposterior (AP), lateral, and sunrise view radiographs of the bilateral knees. (d, e, and f) demonstrate AP, mortise, and lateral view radiographs of the right ankle.
Bilateral patellar tendon rupture is a rare injury, with fewer than 100 cases reported in the literature [8]. Commonly cited risk factors include rheumatoid arthritis, systemic lupus erythematosus, chronic renal disease, hyperparathyroidism, diabetes mellitus, chronic fluoroquinolone use, and systemic steroid use, none of which were reported by the patient or confirmed by laboratory testing in this case [4,9]. However, other studies have indicated that patellar tendonitis is a possible predisposing risk factor, and our patient has radiographic evidence of bilateral patellar tendonitis [4]. Similar to other cases, this patient’s bilateral rupture followed a traumatic event that placed high-force loads on the tendons [4,5,10]. The distinctiveness of this case is further accentuated by the concurrent right ankle syndesmotic injury. To the best of our knowledge, no prior cases report bilateral patellar tendon ruptures with concomitant syndesmotic ankle instability. Interestingly, studies have shown an association between limited ankle dorsiflexion and increased incidence of patellar tendinopathy in athletes [10]. Decreased dorsiflexion range, which could be an associated marker of ankle instability, was found to result in a significantly increased chance of developing patellar tendinopathy within a year [10]. Given the rarity and complexity of this case, care was taken to appropriately plan the method and sequence of repairs. Moreover, the consideration of post-operative mobility led to augmentation of the left-sided patellar tendon repair with an internal brace [5,10,11]. After syndesmotic fixation, intraoperative fluoroscopic external rotation and Cotton stress tests were used to confirm the construct’s stability in accordance with existing literature [12,13]. The combination of bilateral patellar tendon ruptures and a syndesmotic injury presented a challenge in formulating a postoperative mobilisation and rehabilitation protocol. Patients with isolated patellar tendon ruptures are often allowed to weight-bear immediately with the knee in extension [5,8,11,14,15]. Conversely, syndesmotic injuries are often made non-weight-bearing for at least 2 weeks postoperatively with a wide variety in the timing and graduation of weight-bearing after those injuries [9,11,12,16]. Patients with patellar tendon ruptures are typically placed in either a knee immobiliser or a hinged brace with limited motion and locked in extension during weight-bearing [3]. Murphy et al. described their post-operative rehabilitation protocol in a 2022 case report. Physical therapy was gradually introduced to strengthen the quadriceps muscles, and after 6 weeks, the patient can gradually increase weight-bearing with the knee in flexion. However, they advised the avoidance of weight-bearing with the knee flexed past 70°. During the 3rd and 4th months postoperatively, they emphasise the development and maintenance of a normal gait without a brace, while also increasing the range of motion to be able to squat to 70° of flexion. They recommend a gradual return to a normal baseline mobility with the goal of participating in sport around 6–12 months post-operatively [10]. Post-operative weight-bearing and range of motion protocols vary widely for syndesmosis injuries. Porter et al. recommend that patients with isolated syndesmotic injury and repair be made non-weight-bearing in a splint or walking boot for the 1st week before starting protected weight-bearing as tolerated [12]. Per their protocol, normal weight-bearing should be performed by week 3 in the boot or a stirrup brace [12]. The decision to start ankle range of motion exercises at the 2-week mark aligns with past protocols [12]. Review of publicly available postoperative protocols focused on ankle and syndesmotic injury reveals a wide variation in initiation of weight-bearing and exercise [8,9,11,17]. Some recommend weight-bearing as tolerated in a fracture boot starting 2 weeks postoperatively, while others initiate only range-of-motion exercises [9,11,15,16,17]. Those protocols with weight-bearing starting at the 6-week postoperative mark also differ, with some starting partial weight-bearing and others allowing full weight-bearing [9,11,15,16,17]. The optimal timing of weight-bearing and gradation of weight-bearing has not been established in the literature to this point. We sought to protect the syndesmosis repair without imposing undue immobility on our patient. In this case, the combined injuries necessitated modification: Non-weight-bearing on the right leg was advised to protect both the repaired patellar tendon and the syndesmotic fixation, while the left leg was allowed weight-bearing as tolerated with the knee locked in extension. The decision to allow weight-bearing as tolerated on the left leg with an isolated patellar tendon repair allowed for some mobilisation postoperatively.
In patients with multiple injuries, extra care must be taken to ensure proper diagnosis and repair with long-term healing of all injuries.
- Bilateral patellar tendon rupture often indicates underlying chronic tendon pathology
- When one ligament tear is found, care should be taken to evaluate other ligamentous and tendinous structures of the lower extremity
- Post-operative therapy should be directed not only at recovery after injury and surgery but also toward injury prevention.
References
- 1. Rose PS, Frassica FJ. Atraumatic bilateral patellar tendon rupture: A case report and review of the literature. J Bone Joint Surg Am 2001;83:1382-6. [Google Scholar] [PubMed]
- 2. Divani K, Subramanian P, Tsitskaris K, Crone D, Lamba M. Bilateral patellar tendon rupture. JRSM Short Rep 2013; 4(11): DOI: 10.177/ [Google Scholar] [PubMed]
- 3. Kamienski M. Bilateral patellar tendon rupture. Orthop Nurs 2017;36:379-82. [Google Scholar] [PubMed]
- 4. Foley J, Elhelali R, Moiloa D. Spontaneous simultaneous bilateral patellar tendon rupture. BMJ Case Rep 2019;12:e227931. [Google Scholar] [PubMed]
- 5. Taylor BC, Tancev A, Fowler T. Bilateral patellar tendon rupture at different sites without predisposing systemic disease or steroid use. Iowa Orthop J 2009;29:100-4. [Google Scholar] [PubMed]
- 6. Backman LJ, Danielson P. Low range of ankle dorsiflexion predisposes to patellar tendinopathy in junior elite basketball players: A 1-year prospective study. Am J Sports Med 2011;39:2626-33. [Google Scholar] [PubMed]
- 7. Torkaman A, Yousof Gomrokchi A, Elahifar O, Barmayoon P, Shojaei SF. Simultaneous bilateral rupture of patellar tendons in a diabetic haemodialysis patient: A case report. Caspian J Intern Med 2018;9:306-11. [Google Scholar] [PubMed]
- 8. Fernandes A, Rufino M, Hamal D, Mousa A, Fossett E, Cheema KS. Simultaneous bilateral patellar tendon rupture: A systematic review. Cureus 2023;15:e41512. [Google Scholar] [PubMed]
- 9. Botker J, MD. Syndesmosis Fixation with Tight Rope Rehabilitation Protocol. The Orthopaedic and Fracture Clinic. Available from: https://www.ofc-clinic.com/sites/ofcclinic.com/files/Syndesmosis%20Fixation%20with%20Tight%20Rope%20Rehabilitation%20Protocol_1.pdf [Last accessed on 2024 Dec 26]. [Google Scholar] [PubMed]
- 10. Murphy SM, McAleese T, Elghobashy O, Walsh J. Bilateral patellar tendon rupture following low-energy trauma in a young patient without predisposing risk factors. Trauma Case Rep 2022;40:100643. [Google Scholar] [PubMed]
- 11. Ferrel J, MD. Ankle Fracture and Syndesmosis Fixation – Rehab Protocol; 2024. Available from: https://www.orthopedicone.com/wp-content/uploads/2024/10/rehab-protocol-ankle-fractureand-syndesmosis-.pdf [Last accessed on 2024 Dec 26]. [Google Scholar] [PubMed]
- 12. Porter DA, Jaggers RR, Barnes AF, Rund AM. Optimal management of ankle syndesmosis injuries. Open Access J Sports Med 2014;5:173-82. [Google Scholar] [PubMed]
- 13. Vivtcharenko VY, Giarola I, Salgado F, Li S, Wajnsztejn A, Giordano V, et al. Comparison between cotton test and tap test for the assessment of coronal syndesmotic instability: A cadaveric study. Injury 2021;52 Suppl 3:S84-8. [Google Scholar] [PubMed]
- 14. Massachusetts General Brigham Sports Medicine. Rehabilitation Protocol for Patella/Quad Tendon Repairs; 2021. Available from: https://www.massgeneral.org/assets/mgh/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-patella-quad-tendon.pdf [Last accessed on 2026 Jun 14]. [Google Scholar] [PubMed]
- 15. Seybold, J., MD, and Grindal, E., PA-C. Syndesmosis Repair with Tightrope and Internal Brace. Twin Cities Orthopaedics; 2021. Available from: https://tcomn.com/wpcontent/uploads/2021/05/seybold_syndesmosis-rehab_2021-05.pdf [Last accessed on 2024 Dec 26]. [Google Scholar] [PubMed]
- 16. Stirton, J., MD. Ankle/Syndesmosis ORIF Physical Therapy. Union of General Orthopaedics and Sports Medicine: An affiliate of Union General Health System; 2019. Available from: https://jacobstirtonmd.com/wpcontent/uploads/2019/11/ankle-and-syndesmosis-rehab-protocol.pdf [Last accessed on 2024 Dec 26]. [Google Scholar] [PubMed]
- 17. Reddy, M., MD. Ankle Syndesmosis Repair Rehabilitation Protocol. Baylor Scott and White Orthopaedic Associates of Dallas, 2023. Available from: https://s40764.pcdn.co/wp-content/uploads/sites/132/2023/04/ankle-syndesmosis-repair-protocol.pdf [Last accessed on 2024 Dec 26]. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Neglected Ruptures of the Patellar Tendon: Report of Three Cases in the Orthopedic Trauma Department of Dalal Jamm Hospital, Dakar
April 1, 2026 Neglected Ruptures of the Patellar Tendon: Report of Three Cases in the Orthopedic Trauma Department of Dalal Jamm Hospital, Dakar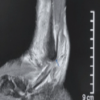 February 1, 2026 Split Peroneus Brevis: An Overlooked Cause of Ankle Dysfunction
February 1, 2026 Split Peroneus Brevis: An Overlooked Cause of Ankle Dysfunction July 1, 2025 Fusion under the Scope: Minimally Invasive Arthroscopic Tibiotalocalcaneal Arthrodesis in the Setting of Post-traumatic Fibular Loss: A Case Report
July 1, 2025 Fusion under the Scope: Minimally Invasive Arthroscopic Tibiotalocalcaneal Arthrodesis in the Setting of Post-traumatic Fibular Loss: A Case Report May 10, 2024 Complete Ankle Joint that is Tibiotalar and Distal Tibiofibular Coalition Presenting with Foot and Ankle Pain – A Case Report
May 10, 2024 Complete Ankle Joint that is Tibiotalar and Distal Tibiofibular Coalition Presenting with Foot and Ankle Pain – A Case Report