
Undiagnosed primary hyperparathyroidism can present as metabolic bone failure leading to rare bilateral femoral neck fractures in young adults, highlighting the need for early endocrine evaluation in unexplained skeletal symptoms.
Dr. M Sharath Raj, Department of Orthopedic Surgery, Postgraduate Institute of Medical Education and Research, Madhya Marg, Sector 12, Chandigarh - 160012, India. E-mail: sharathraj.pgi@gmail.com
Abstract
Introduction: Primary hyperparathyroidism, though commonly diagnosed through hypercalcemic symptoms, can rarely present as advanced skeletal pathology due to delayed recognition. Metabolic bone disease, including osteitis fibrosa cystica and fragility fractures, represents a late and uncommon manifestation in the modern diagnostic era.
Case Report: We report a rare case of a 26-year-old male who presented with bilateral femoral neck fractures following 4.5 years of progressive hip pain. He had a history of parathyroid adenoma excision 2 years prior and was diagnosed with “hungry bone syndrome” postoperatively. Imaging revealed classic skeletal changes of severe metabolic bone disease, including osteolysis, spinal deformities, and multiple cystic lesions. He underwent staged bilateral total hip arthroplasty with good functional recovery over 1 year.
Conclusion: This case underscores the importance of considering primary hyperparathyroidism in young patients presenting with unexplained skeletal complaints. Early recognition and management are essential to prevent irreversible bone damage and avoid debilitating complications such as bilateral femoral neck fractures.
Keywords: Primary hyperparathyroidism, parathyroid adenoma, metabolic bone disease, bilateral femoral neck fracture, hungry bone syndrome, total hip arthroplasty.
One of the most prevalent endocrine conditions is primary hyperparathyroidism. One acute presentation that revolves around hypercalcemic homeostasis is typically used to establish the diagnosis [1]. In the past 20 years, indolent forms involving the bones have hardly been seen, and the characteristics that coincide with dystrophies, skeletal dysplasia, and cancers may make diagnosis more difficult [2,3]. 2–3% of all neck of femur fractures in people under 50 are femoral neck fractures [4]. High-energy trauma accounts for the majority of fractures in this age range [4,5]. In young adults, bilateral atraumatic femoral neck fractures occurring simultaneously are regarded as extremely uncommon occurrences. There were not many cases in this age range documented in the literature [6,7]. Avascular necrosis and non-union are among the consequences linked to these fractures [8,9]. Anatomical reduction, early fixation, and rehabilitation are crucial to avoid such devastating complications. We report this rare case of bilateral neck of femur fracture in a young adult, along with varied manifestations of metabolic bone failure that are pathognomonic of hyperparathyroidism. We also highlight the current evidence-based practices in the management of various bony manifestations.
A 26-year-old male patient came in with a history of bilateral hip pain that had been ongoing for 4.5 years. His medical journey began with a referral from the endocrinology department after the removal of a right inferior parathyroid adenoma (RIPA) 2 years prior. This adenoma was discovered incidentally while evaluating his generalised weakness and persistent bilateral hip pain, which had started 2 years before the surgery. When he presented, he reported that the hip pain had continued for 4.5 years. About 4.5 years ago, he had been asymptomatic until he developed hip pain, which also led to a noticeable change in his gait. Radiographic imaging showed atraumatic fractures in both hips. In addition, the patient has been experiencing intermittent abdominal pain for the past year, described as nausea and vomiting, localised to the flank without any radiation to the back. In the 2 years leading up to his referral, he reported symptoms including anorexia, weight loss, muscle mass loss, and general fatigue. His medical history includes the removal of a benign tumour beneath the left molar tooth, thought to be an epulis, 9 years ago. After the excision of RIPA in 2022, the findings are summarised in Table 1.
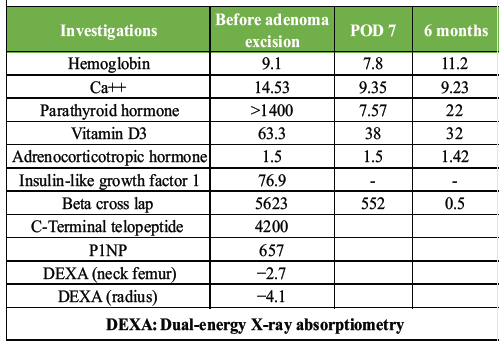
Table 1: Serial laboratory investigations before and after parathyroid adenoma excision
The patient was diagnosed with “hungry bone syndrome” and was treated with replacement therapy. His overall condition improved and stabilised with the administration of parenteral calcium gluconate and neutral phosphate. On examination, the patient was found to be conscious, cooperative, and orientated, with a Glasgow Coma Scale of E4V5M6. Systemic examination findings include: Weight: 54 kg, height: 152 cm, body mass index: 19 kg/m,2 AS: 160 cm, US: LS 75:88 cm (−0.85), and a scar mark noted. Central nervous system: E4V5M6, motor power assessed at 5/5 in both lower limbs and upper limbs bilaterally, reflexes graded at 2+ for triceps, biceps, knee, and ankle; plantar reflex is flexor. The patient has lost three molar teeth in the left jaw and exhibits lordosis with a bilateral waddling gait, along with a scar mark on the abdomen. An initial physical examination of the hips revealed a negative Patrick test, full range of motion, and mild soreness in the groin area; the Harris Hip Score was 60 in both hips. Generalised muscle atrophy was noticed. The plain radiographs revealed bilateral neck of femur fractures (both of which were graded as Type IV according to Garden’s classification) with multiple small cysts in the femoral head and acetabulum; moderate joint space narrowing features suggesting osteoarthritis (OA) and overriding of the greater trochanter; generalised osteoporosis; and multiple lytic lesions in the tibia and pelvis, along with regional changes like severe anterolateral bowing of the femur (Fig. 1), salt-and-pepper skull, kyphoscoliosis in the spine with cod-fish and rugger jersey appearance (Fig. 2) and acro-osteolysis of the hand (Fig. 3).
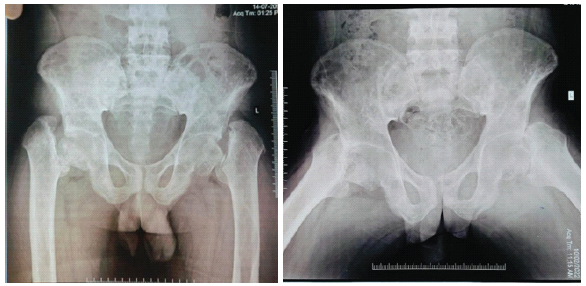
Figure 1: Hip joint (bilateral neck of femur fracture and osteoarthritis changes).
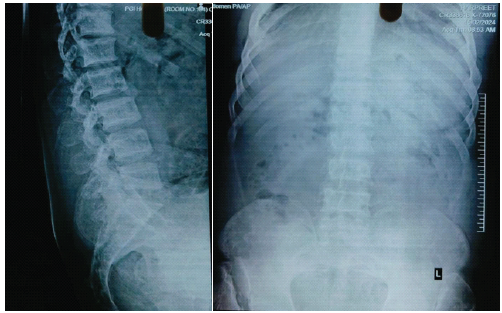
Figure 2: Spine (kyphoscoliosis in the spine with cod-fish and rugger jersey appearance).

Figure 3: (Acro-osteolysis of hand).
All these metabolic changes in the skeleton as identified in the imaging studies are summarised in Table 2.
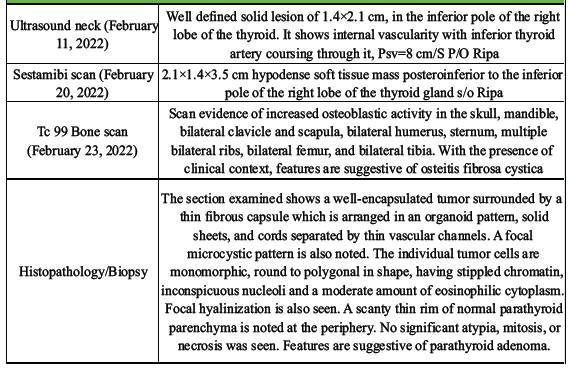
Table 2: Imaging studies
The patient underwent optimisation and was deemed suitable for surgical intervention a few days following admission. A total hip arthroplasty (THA) was indicated due to the presence of established OA changes. Our senior consultant (AA) decided to perform a hybrid THA, utilising an uncemented cup and a cemented stem, in light of the observed cortico-medullary irregularities in the femur (Fig. 4).
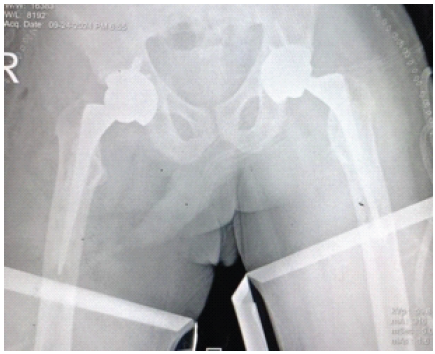
Figure 4: Post-operative X-ray.
Postoperatively, the patient remained non-weight-bearing on both legs for 4 days. Subsequently, he began knee-bending exercises, practised side-sitting, and was assisted in walking with a walker under supervision. He was ultimately discharged in an improved condition. Subsequent follow-ups at 1 month, 3 months, 6 months, and 1 year revealed that the patient could walk independently and bear weight fully, exhibiting no limping and a pain-free gait. He was able to walk and run slowly but was unable to squat. Approximately 12 months later, the patient returned for another evaluation. He was able to walk without a limp and reported no further pain. Daily activities were performed within the permissible range of motion associated with total hip replacement. An X-ray indicated a normal right hip with the implant in place after 1 year (Fig. 5). The Harris Hip Score improved to 90 on both sides, and the left hip’s range of motion increased to 120° of flexion. Impingement tests yielded negative results, and flexion, abduction, and external rotation were within normal limits.

Figure 5: One-year follow-up X-ray.
Parathyroid adenomas, especially solitary ones, are the predominant cause of primary hyperparathyroidism, with adenomatous parathyroid tissue often located in ectopic sites [10]. Approximately 5% of these adenomas are identified in the mediastinum, with 95% of those situated within the thymus [11]. Post-operative hypocalcemia is frequently observed in the early stages following parathyroid surgery. A specific condition known as “hungry bone syndrome” can lead to significant hypocalcemia immediately after surgery, which may prove resistant to treatment. While mild hypocalcemia can often be managed with oral calcium supplements, severe cases necessitate parenteral calcium administration. Skeletal involvement in primary hyperparathyroidism is estimated to occur in about 2% of cases [12]. Evidence supporting the notion that reduced bone density due to hyperparathyroidism correlates with a higher fracture rate is limited Wilson et al., [13]. Found no significant increase in vertebral fractures among 174 hyperparathyroid patients, whereas Peacock [14] reported a higher incidence of both vertebral and cortical fractures in this population. The occurrence of femoral neck fractures resulting from ectopic parathyroid adenomas is exceedingly rare, and prompt surgical intervention is essential to mitigate the risks of non-union and avascular necrosis [15].
This case highlights the severe skeletal manifestations that can result from delayed diagnosis of primary hyperparathyroidism, including bilateral femoral neck fractures in a young adult. Despite advancements in diagnostic modalities, indolent presentations involving bone metabolism continue to occur and can lead to significant morbidity if not recognised early. Comprehensive endocrine evaluation in young patients with unexplained musculoskeletal symptoms is essential. Timely surgical and orthopaedic interventions, combined with metabolic correction, can lead to favourable functional outcomes even in advanced cases.
In young patients presenting with unexplained bone pain or fragility fractures, especially in the absence of trauma, clinicians should consider underlying metabolic bone disorders such as primary hyperparathyroidism. Early diagnosis and multidisciplinary management are crucial to prevent severe skeletal complications and optimize patient outcomes.
References
- 1. MadkhaliT, AlhefdhiA, ChenH, ElfenbeinD. Primary hyperparathyroidism. Ulus Cerrahi Derg 2016;32:58-66. [Google Scholar] [PubMed]
- 2. MuthukrishnanJ, HarikumarKV, SangeetaJ, SinghMK, ModiK. Nerve, muscle or bone disease? Look before you leap. Singapore Med J2009;50:e293-4. [Google Scholar] [PubMed]
- 3. Ullah E, Ahmad M, Ali SA, Redhu N. Primary hyperparathyroidism having multiple Brown tumours mimicking malignancy. Indian J Endocrinol Metab 2012;16:1040-2. [Google Scholar] [PubMed]
- 4. RobinsonCM, Court-BrownCM, McQueenMM, ChristieJ. Hip fractures in adults younger than 50 years of age. Epidemiology and results. Clin Orthop Relat Res 1995;312:238-46. [Google Scholar] [PubMed]
- 5. Askin SR, Bryan RS. Femoral neck fractures in young adults. Clin Orthop Related Res 1976;114:259-64. [Google Scholar] [PubMed]
- 6. HaronianE, SilverJW, MesaJ. Simultaneous bilateral femoral neck fracture and greater tuberosity shoulder fracture resulting from a seizure. Orthopaedics 2002;25:757-8. [Google Scholar] [PubMed]
- 7. Shah HM, Grover A, Gadi D. Bilateral neck femur fracture following a generalised seizure – a rare case report. Arch Bone Joint Surg 2014;2:255-7. [Google Scholar] [PubMed]
- 8. StocktonDJ, O’HaraLM, O’HaraNN, LefaivreKA, O’BrienPJ, and SlobogeanGP. High rate of reoperation and conversion to total hip arthroplasty after internal fixation of young femoral neck fractures: A population-based study of 796 patients. Acta Orthop2019;90:21-5. [Google Scholar] [PubMed]
- 9. Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury2015;46:484-91. [Google Scholar] [PubMed]
- 10. Palmer JA, Brown WA, Kerr WH, Rosen IB, Walters NA. The surgical aspects of hyperparathyroidism. Arch Surg 1975;110:1004-7. [Google Scholar] [PubMed]
- 11. Geelhoed GW, Krudy AG, Doppman JL. Long-term follow-up of patients with hyperparathyroidism treated by transcatheter staining with contrast agent. Surgery1983;94:849-62. [Google Scholar] [PubMed]
- 12. Silverberg SJ, Shane E, DeLaCruz L. Skeletal disease in primary hyperparathyroidism. J Bone Miner Res 1989;4:283-91. [Google Scholar] [PubMed]
- 13. Wilson RJ, Rao DS, Ellis B, Kleerekoper M, Parfitt AM. Mild asymptomatic primary hyperparathyroidism is not a risk factor for vertebral fractures. Ann Intern Med 1988;109:959-62. [Google Scholar] [PubMed]
- 14. Peacock M. Interpretation of bone loss determinations as they relate to fracture: Implications for asymptomatic primary parathyroidism. J Bone Miner Res 1991;6:S77-82. [Google Scholar] [PubMed]
- 15. BrownJT, AbramiG. Transcervical femoral fracture. A review of 195 patients treated by sliding nail-plate fixation. J Bone Joint Surg Br 1964;46:648-63. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Bilateral Distal Quadriceps Tendon Rupture in a Young Male Following Minimal Trauma: First Presentation of Primary Hyperparathyroidism Due to a Parathyroid Adenoma
November 1, 2025 Bilateral Distal Quadriceps Tendon Rupture in a Young Male Following Minimal Trauma: First Presentation of Primary Hyperparathyroidism Due to a Parathyroid Adenoma January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty
January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty July 1, 2025 A Primary Hyperparathyroidism in an Adolescent Female with Pathological Fractures and Multiple Bone Lesions Due to Parathyroid Adenoma: Case Report
July 1, 2025 A Primary Hyperparathyroidism in an Adolescent Female with Pathological Fractures and Multiple Bone Lesions Due to Parathyroid Adenoma: Case Report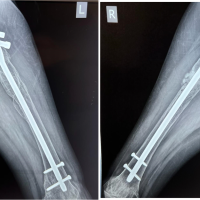 September 1, 2024 A Case of Parathyroid Adenoma with Bilateral Subtrochanteric Pathological Femur Fracture – A Rare Case Report
September 1, 2024 A Case of Parathyroid Adenoma with Bilateral Subtrochanteric Pathological Femur Fracture – A Rare Case Report