
Mediolateral instability of the elbow can be treated with dual ligament reconstruction to achieve a good functional outcome even in neglected cases.
Dr Kalyan Deepak Sreenivas, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: drkalyan34@gmail.com
Abstract
Introduction: Injuries around the elbow can cause medial, lateral, or combined mediolateral instability. Surgical intervention is often required in cases of lateral instability, with lateral ulnar collateral ligament reconstruction being the preferred treatment. Medial instability is frequently seen in sports involving throwing, such as baseball and American football. In elite athletes, ligament reconstruction is preferred over conservative treatment or ligament repair to facilitate a faster return to professional sports. Combined medial and lateral ligament injuries are rare but need early repair or reconstruction. These injuries, when left untreated, can cause chronic disability and early-onset arthritis. In these cases, reconstructing both medial and lateral ligaments is essential.
Case Report: A 37-year-old patient presented with an injury 2 years ago. She was having persistent elbow pain affecting daily activities. MRI revealed a LUCL and UCL tear. We performed LUCL reconstruction using the triceps autograft and MUCL reconstruction using the PL autograft using the docking technique. Patient’s elbow function improved from Mayo’s elbow performance index of poor (40) to good (85).
Conclusion: Mediolateral instability can be treated with reconstruction of both the LUCL and UCL using tendon grafts via the docking technique, even in neglected cases, thereby achieving a good functional outcome.
Keywords: Global instability of the elbow, lateral ulnar collateral ligament, medial ulnar collateral ligament, reconstruction, elbow instability.
The elbow is the second most frequently dislocated joint after the shoulder [1]. The patients may develop recurrent dislocation and medial or lateral instability following elbow trauma [2]. Injuries to the lateral collateral ligament (LCL) complex and medial collateral ligament (MCL) complex can cause lateral or medial instability, respectively. LCL consists of the lateral ulnar collateral ligament (LUCL), annular ligament, and radial collateral ligament (RCL). The MCL complex comprises the medial ulnar collateral ligament (MUCL), the posterior bundle, and the transverse ligament. While isolated medial or lateral instability is common, combined mediolateral instability, resulting from concurrent MCL and LCL injuries, is rare. This uncommon injury typically requires surgical management [3]. If left untreated, elbow instability can lead to chronic pain, functional impairment, and early onset of arthritis. When treated early, surgical options include external fixation, ligament repair, or reconstruction. On the lateral side, the LUCL is the primary constraint against posterolateral rotator instability. Hence, LUCL reconstruction is necessary for its surgical treatment [4]. Likewise, MUCL is the primary static stabiliser to valgus stress at the elbow, and it is frequently injured in sports like baseball. Various techniques have been described for MUCL and LUCL reconstruction [3,5]. This article details the surgical approach for managing a chronic case of combined posterolateral and medial elbow instability that had remained untreated for 2 years. The patient underwent ligament reconstruction using the docking technique, with grafts derived from the triceps aponeurosis and palmaris longus (PL) tendons.
History and examination:
A 37-year-old woman with right-hand dominance presented to us with a history of injury to the right elbow following a road traffic accident and a fall from a two-wheeler onto her outstretched hand 2 years ago. The patient was treated conservatively in her local centre. The patient had persistent pain, had a history of instability, and was unable to do household activities such as lifting objects, cleaning the house, washing, and wearing clothes. She consulted a few local physicians and was treated with pain-relieving medications alone. On examination, she had tenderness on both the medial and lateral condyles and a range of movement (ROM) of 0–120 and 0–60° of pronation and supination. The varus and valgus stress tests were positive in extension and flexion (Fig. 1).

Figure 1: Valgus stress test, resting position, and varus stress test show significant medial and lateral instability.
Mayo’s elbow performance index of the patient was poor (score of 40). Magnetic resonance imaging (MRI) of the right elbow joint revealed a complete tear of the LUCL and anterior ulnar collateral ligament (UCL), along with moderate joint effusion and traumatic neuritis of the ulnar nerve (Figs. 2, 3, 4).
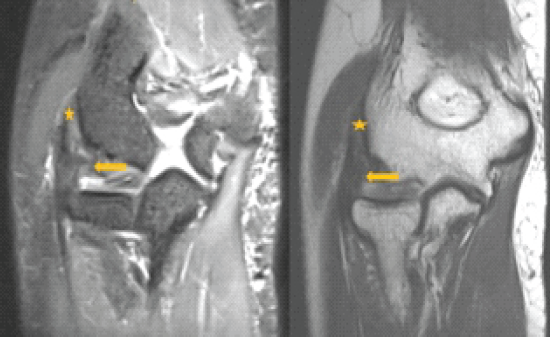
Figure 2: (a and b) Coronal short tau inversion recovery and T2-weighted images demonstrating complete tear of the radial collateral ligament and lateral ulnar collateral ligament with extensive fraying of the fibers (arrows). Note made of normal common extensor tendon origin (asterisk).
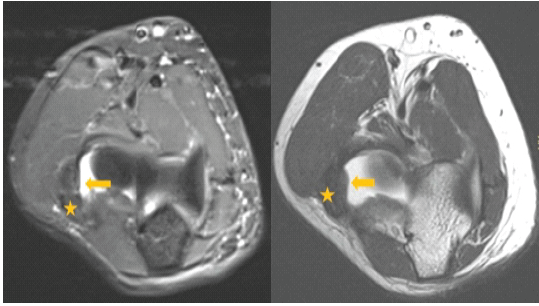
Figure 3: (a and b) Axial short tau inversion recovery and T2-weighted images demonstrating the complete absence of radial collateral ligament and lateral ulnar collateral ligament at their normal expected location (arrows). Note made of normal common extensor tendon (asterisk).
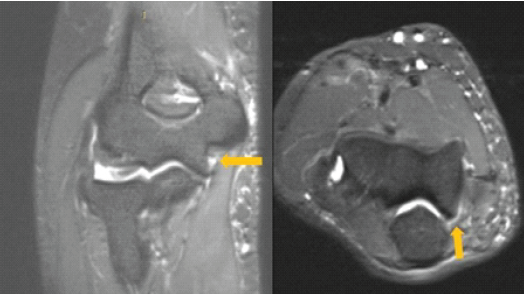
Figure 4: (a and b) Coronal and axial proton density fat saturation images demonstrating fraying of the fibers at the humeral attachment of posterior ulnar collateral ligament (arrows).
Management:
We diagnosed it as chronic posterolateral and medial instability with an MCL and LCL tear of the right elbow. The patient underwent LUCL reconstruction using the triceps autograft and MUCL reconstruction using the PL autograft using the docking technique.
Surgical technique:
Lateral reconstruction:
Graft harvest:
In the lateral decubitus position under general anaesthesia,, we took the triceps aponeurosis harvest using the technique described by Pucher et al. [4] A 12 cm curvilinear incision was taken from the posterior aspect of the elbow with a distal curve to the lateral side of the elbow (Fig. 5). A superficialal triceps aponeurosis of 5 mm thickness and 7 cm length was dissected from the ulnar side; the distal end was sutured using the modified Krackow technique with a no. 2 non-absorbable suture.

Figure 5: An incision over the distal triceps is curved toward lateral epicondyle and extended distally toward ulna as in Kocher’s approach.
Approach:
To expose the lateral side of the elbow, the distal end of the same posterior skin incision is extended using Kocher’s approach to the proximal ulna (Fig. 4). We split the tissues between the anconeus and extensor carpi ulnaris to reach the lateral collateral footprint at the supinator crest on the ulna.
Fixation of graft to ulna:
Two cortical holes, 1 cm apart, were drilled at this footprint. The sutures from the distal end of the triceps graft are passed into the proximal hole to exit from the distal hole and tied over an extracortical button.
Fixation of graft to humerus:
The proximal part of the Kocher approach is used to expose the common extensor tendon origin. The isometric centre of the elbow was identified by serial flexion and extension of the elbow. The graft was shortened to an adequate length and secured to the lateral humeral condyle using the docking technique. A 4.0-mm socket was drilled to a depth of 15 mm at the humeral footprint, and two smaller (2 mm) perforating tunnels were created from the anterior humerus to the base of this socket. Looped passing sutures were passed through these small perforating tunnels out to the large socket. The graft was pulled into the humerus as shown in the figure and tied over the bone bridge (Fig. 6). We did the varus stress test and found the elbow stable. The soft tissues and skin were closed after a thorough wash.
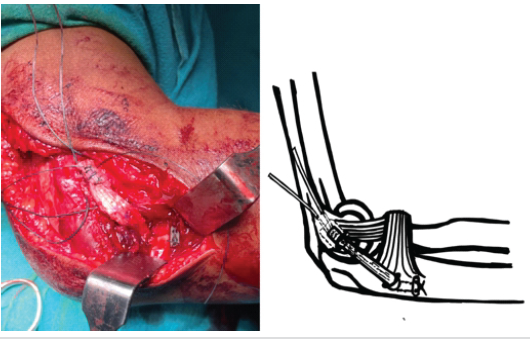
Figure 6: Lateral ulnar collateral ligament (LUCL) reconstruction and illustration. LUCL is reconstructed using triceps graft and fixed proximally using the docking technique and distally using the extramedullary endobutton technique.
Medial reconstruction:
We repositioned the patient to supine for medial side reconstruction. We planned to reconstruct the anterior UCL using the docking technique [6,7]. Graft harvest: The location of the PL tendon on the wrist crease is marked preoperatively. Intraoperatively, a 1-cm transverse incision is made over the palmaris at the wrist crease. Forceps are passed under the tendon. Great care is taken to ensure that the median nerve is not accidentally harvested. The tendon is held under tension and palpated proximally. A second 1-cm transverse incision is made over the tendon as far proximally as it can be palpated. Forceps are then passed under the tendon in the proximal incision, repeated a 3rd or 4th time. The tendon should be harvested as close to the tendon-muscle belly interface as possible to maximise graft length. The PL graft was then doubled.
Medial approach:
A medial-based curvilinear incision of 8 cm is made, centringaround the elbow joint. The ulnar nerve is identified as running between the two heads of the flexor carpi ulnaris (FCU) and is protected. The FCU is split in line with its fibres over the sublime tubercle to expose the attachment of the native UCL. The flexor-pronator raphe is split from the medial epicondyle to the sublime tubercle in the “safe zone” [8]. Valgus stress showed an opening of the ulnohumeral articulation, suggesting MCL insufficiency.
Fixation of graft to ulna and humerus:
We made two converging 3.5 mm drill holes 7 mm apart on either side of the sublime tubercle, 1 cm distal to the joint line. On the humeral side, we drilled a 4 mm entry socket and two small 2 mm exit sockets in the anterior aspect of the medial humeral condyle. One end of the tendon is tied with sutures and passed through the ulnar tunnels. The other end of the graft is then prepared to the exact length to fit inside the humeral tunnel. We pulled the sutures on the ends of the graft through the small tunnels to dock the graft into the 4 mm tunnels.. The graft is tensioned adequately and tied over the humeral bony bridge (Fig. 7). The elbow was checked for stability using the varus and valgus stress test and found stable on the table. The flexor pronator raphe is sutured. The wound was closed in layers.
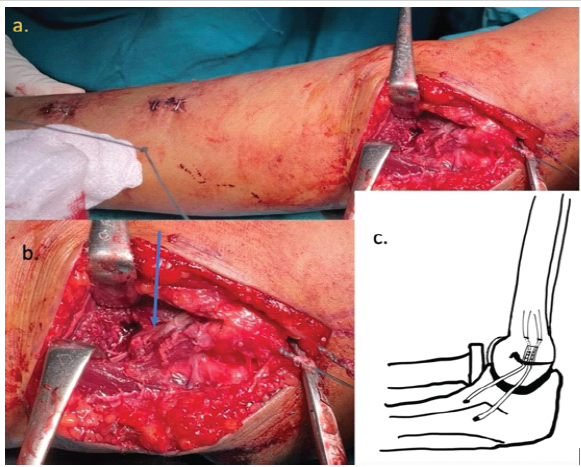
Figure 7: Medial ulnar collateral ligament reconstruction and illustration. (a) Shows incisions for palmaris longus (PL) graft harvest and medial approach. (b) The PL (blue arrow) is looped in the ulnar tunnel distally and tied over a bony bridge proximally using the docking technique. (c) Illustration showing a graft docked in the humerus tunnel to be tied over the bony bridge.
Post-operative care:
The post-operative X-ray showed satisfactory alignment without any signs of instability (Fig. 8). The patient’s elbow was immobilised using an above-elbow posterior slab at 90° of flexion for 2 weeks. After 2 weeks, the patient was allowed a gradual passive and active assisted ROM with a hinged elbow brace for 6 weeks. The patient’s symptoms of pain and instability have gradually improved. At 1-year follow-up, the patient had a full ROM and a Mayo Elbow performance score of 85 (Fig. 9).
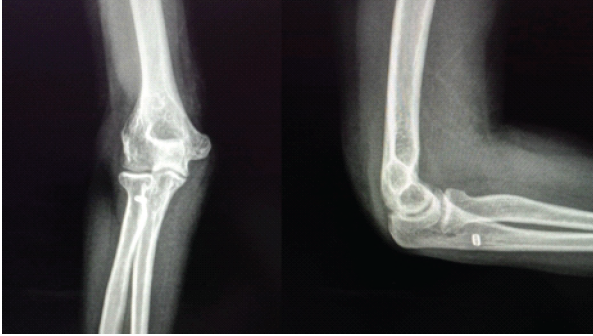
Figure 8: Post-operative radiograph shows normalized carrying angle and ulnohumeral congruity.

Figure 9: Elbow range of movement at 2-year follow-up with the surgical scars.
MCL and LCLs and ulnohumeral articulation are the primary stabilisers in the elbow joint. The majority of simple dislocations heal without recurrence or instability, but it is essential to check for instability, and in case of instability, an MRI assessment should be done [2]. LUCL resists posterolateral instability, and the anterior bundle of MCL resists medial instability. Damage to these ligaments leads to a painful, unstable elbow, affecting its function. Studies have shown good results with early repair of LUCL in acute cases [9]. Results for early repair of MCL are not satisfactory; hence, reconstruction is advised in isolated MCL injuries. Combined chronic rupture of the MCL and LCL is rare. Our patient presented 2 years after injury with the inability to do her daily activities because of the unstable elbow. Chronic mediolateral ligament instability needs reconstruction of the injured ligaments. Stability can be achieved using single-ligament reconstruction or dual ligament reconstruction techniques. Techniques can also vary depending on the graft and methods of fixation to the ulna or humerus. Van Riet et al. demonstrated a single gracilis tendon used as a single or double loop across the humerus and ulna to reconstruct both sides [9]. Finkbone and O’Driscoll published a modification of this, known as the box technique, without using hardware [3]. The advantage of single ligament reconstruction is the avoidance of multiple fixation points. Disadvantages include the need for gracilis tendon harvest and associated donor site morbidity. In a study on biomechanical evaluation, Hackl et al. have found comparable stability in both types of reconstructions [10]. Multiple techniques have been described for the individual reconstruction of the medial and lateral ligaments.
Lateral side:
Reconstructions are either anatomic or non-anatomic using autografts, allografts, or synthetic grafts. Autografts such as gracilis and triceps have better outcomes.
Humerus fixation:
Fixation to the humerus bone can be done using transosseous tunnels (Docking technique), suture anchor, or interferential screws [5]. The docking technique is the most commonly used and has good outcomes. Although all the above fixation methods have good reported outcomes individually, more comparative studies are still needed.
Ulna fixation:
Pucher et al. [4] have suggested using flipping of the endobutton intramedullary and tensioning the graft. We avoided the intramedullary flipping using two ulnar tunnels, with one for graft entry and a distal one for suture exit and tying over the endobutton (Fig. 6).
Medial side:
Approach to the medial side is associated with ulnar nerve complications. Smith et al. [8] have described a safe zone for exposure of the MCL footprint on the humerus.
Humerus fixation:
AUCL reconstruction is usually done using the modified Jobes or docking technique on the humerus. The docking technique has the advantage of less bone removal, avoidance of transposition of the ulnar nerve, and preservation of the flexor-pronator complex.
Ulna fixation:
In the docking technique, the graft is fixed near the sub-tubercle into two converging tunnels, as done in this case. Native MUCL has an extended footprint over the ulna. Camp et al. have proposed a novel technique for anatomical reconstruction of MUCL to make this more anatomical and stronger [6].
Rehabilitation:
Regardless of the surgical technique, elbow movement is encouraged 1 week after surgery. We applied a hinged elbow brace and allowed a gradual progressive increase in range of movement for the next six weeks. Some authors have suggested a wait for 3 weeks for ligament healing before starting ROM [2].
Outcomes:
Surgical treatment of instability has provided good to excellent results in medial or lateral individual ligament injuries. There have been very few studies on outcomes in medio-lateral reconstruction in combined ligamentous injuries. Krishna et al. [2] reported excellent results with the single loop technique in a 3-month-old neglected elbow dislocation. Finkbone and O’Driscoll [3], in their box-loop reconstruction technique for combined mediolateral instability, reported Mayo Elbow Performance Index (MEPI) scores of excellent and good in 7 out of 10 patients; three patients had fair outcomes, and no patient had poor results. The mean MEPI score after surgery was 84, similar to our case. There is a need for more clinical studies on outcomes comparing different methods of reconstruction.
Chronic mediolateral elbow instability managed with the reconstruction of both LUCL and MUCL is successful and beneficial even in neglected cases. The use of triceps and PL grafts avoids lower limb donor-site morbidity. The docking technique for graft fixation to the medial and lateral humerus gives good stability and a good functional outcome.
Chronic elbow instability can result if the injuries are not detected early and treated early. Neglected medio-lateral elbow instability can be treated effectively with dual ligament reconstruction.
References
- 1. Kuhn MA, Ross G. Acute elbow dislocations. Orthop Clin North Am 2008;39:155-61. [Google Scholar] [PubMed]
- 2. Krishna SV, Ballal M, Br V, Hs C. Multidirectional Instability in a Neglected Elbow Dislocation Managed with Circumferential Ligament Reconstruction. A Case Report. Rev Bras Ortop (Sao Paulo). 2020 Sep 25;58(1):168-172. doi: 10.1055/s-0040-1714232. PMID: 36969788; PMCID: PMC10038705. [Google Scholar] [PubMed] [CrossRef]
- 3. Finkbone PR, O’Driscoll SW. Box-loop ligament reconstruction of the elbow for medial and lateral instability. J Shoulder Elbow Surg 2015;24:647-54. [Google Scholar] [PubMed]
- 4. Pucher CJ, Lanzerath F, Hackl M, Müller LP. Lateral ulnar collateral ligament reconstruction of the elbow using a triceps tendon autograft – a technical note. Obere Extremität 2023;18:41-4. [Google Scholar] [PubMed]
- 5. Badhrinarayanan S, Desai A, Watson JJ, White CH, Phadnis J. Indications, outcomes, and complications of lateral ulnar collateral ligament reconstruction of the elbow for chronic posterolateral rotatory instability: A systematic review. Am J Sports Med 2021;49:830-7. [Google Scholar] [PubMed]
- 6. Camp CL, Bernard C, Benavitz B, Konicek J, Altchek DW, Dines JS. Reconstruction of the Medial Ulnar Collateral Ligament of the Elbow: Biomechanical Comparison of a Novel Anatomic Technique to the Docking Technique. Orthop J Sports Med. 2019 Jul 17;7(7):2325967119857592. [Google Scholar] [PubMed]
- 7. Rohrbough JT, Altchek DW, Hyman J, Williams RJ 3rd, Botts JD. Medial collateral ligament reconstruction of the elbow using the docking technique. Am J Sports Med 2002;30:541-8. [Google Scholar] [PubMed]
- 8. Smith GR, Altchek DW, Pagnani MJ, Keeley JR. A muscle-splitting approach to the ulnar collateral ligament of the elbow. Neuroanatomy and operative technique. Am J Sports Med 1996;24:575-80. [Google Scholar] [PubMed]
- 9. Van Riet RP, Bain GI, Baird R, Lim YW. Simultaneous reconstruction of medial and lateral elbow ligaments for instability using a circumferential graft. Tech Hand Up Extrem Surg 2006;10:239-44. [Google Scholar] [PubMed]
- 10. Hackl M, Heinze N, Wegmann K, Lappen S, Leschinger T, Burkhart KJ, et al. The circumferential graft technique for treatment of multidirectional elbow instability: A comparative biomechanical evaluation. J Shoulder Elbow Surg 2016;25:127-35. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction
June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction May 1, 2026 Functional Outcomes and Complications of Megaprosthetic Reconstruction in Limb-Salvage Surgery for Musculoskeletal Tumors: A Scoping Review
May 1, 2026 Functional Outcomes and Complications of Megaprosthetic Reconstruction in Limb-Salvage Surgery for Musculoskeletal Tumors: A Scoping Review
 April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability
April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability