
The AGN1 triphasic calcium implant provides immediate stability and complete resorption, effectively treating a paediatric simple bone cyst.
Nicolas De Ridder, Department of Orthopaedics and Traumatology, University Hospitals Leuven (UZ Leuven), Leuven, Belgium. E-mail: nicolasderidder@outlook.com
Abstract
Introduction: Simple bone cysts (SBCs) are benign lesions in children, typically in the proximal humerus. While many are asymptomatic, some necessitate treatment because of impending pathological fractures. Different treatment modalities exist, but no consensus on the best method has been established.
Case Report: To the best of our knowledge, this case report describes the first reported clinical application of AGN1 (Ossure™), a CE-marked triphasic calcium-based resorbable implant, in the treatment of a large SBC. A 10-year-old girl with a history of recurrent fractures secondary to a large SBC in the right humerus underwent curettage and AGN1 implantation. The procedure provided immediate stability after implantation and promoted bone healing during the resorption phase. She experienced rapid functional recovery with full mobility in 2 weeks. Early radiographic imaging showed rapid integration at 3 months. Long-term follow-up at nearly 3 years postoperatively confirmed complete resorption of the implant with restoration of normal bone architecture, leaving only a small, asymptomatic residual cyst distally.
Conclusion: Current treatments for SBCs, including corticosteroid injections and bone grafting, show varying success rates. AGN1, known for its osteo-enhancing properties in other clinical applications, provided immediate structural support and facilitated rapid bone regeneration with complete resolution of a large SBC in this case. AGN1 may offer a promising alternative for treating large SBCs, especially in patients at high risk of fractures. Its ability to provide early mechanical stability and promote bone regeneration warrants further clinical investigation to assess its use in select cases.
Keywords: AGN1, bone substitute, local osteo-enhancement procedure, simple bone cyst, unicameral bone cyst.
Simple bone cysts (SBCs), also referred to as unicameral bone cysts, are benign fluid-filled lesions mainly seen in the long bones of paediatric patients. They are predominantly seen in the proximal humerus, followed by the proximal femur. These cysts were first thoroughly documented by Virchow in 1876. The exact aetiology remains unknown, although the vascular theory suggests that increased osseous pressure compared to normal bone marrow pressure results in venous drainage obstruction. A cyst can be considered active when in direct contact with the growth plate and inactive when it is not [1]. SBCs have attracted attention not only due to their clinical presentation but also because of the management challenges they present. Most of these cysts are asymptomatic and do not require treatment. However, a follow-up study demonstrated that, contrary to historical belief, these cysts do not spontaneously resolve [2]. However, sometimes they can cause pain, or larger cysts can lead to cortical thinning with subsequent pathological fractures, necessitating treatment. The primary aim of treatment in these cases is to reduce fracture risk by encouraging cyst healing. Numerous therapies have been proposed, the most common being observation, percutaneous injection with corticosteroids or bone marrow aspirate, open curettage with bone grafting or artificial bone substitute, or curettage with elastic stable intramedullary nailing (ESIN). These treatments all have variable healing and recurrence rates, and there seems to be no gold standard for treatment [3]. We present a case we treated in our hospital with curettage and implantation of a relatively new biomaterial, AGN1 (Ossure™; AgNovos Healthcare, New York, NY, USA) [4]. AGN1 is a CE-marked tri-phasic resorbable calcium implant, used in local osteo-enhancement procedures (LOEP). In this minor procedure, severe osteoporosis of the proximal femoral neck in high-risk patients is treated by curettage and injection of AGN1 locally to increase bone mineral density in the proximal femur in patients at high risk for hip fractures. This achieves instant biomechanical strengthening of the bone [5,6]. While progressively resorbing over time, it will act as an osteoconductive scaffold to promote physiological bone remodelling and new trabecular bone formation within the enhancement site [4,7,8]. The primary goal in our case was to offer a stable situation to prevent new pathological fractures, as well as rapid healing of the large bone cyst. A comprehensive literature search in PubMed and Embase (up to March 2026) using the terms “AGN1” OR “triphasic calcium matrix” AND “bone cyst” yielded no previous clinical reports in this population, making this a novel application of the material.
A 10-year-old girl was referred to our regional hospital after sustaining a recurrent pathological fracture to the right humerus due to a minor fall (Fig. 1).
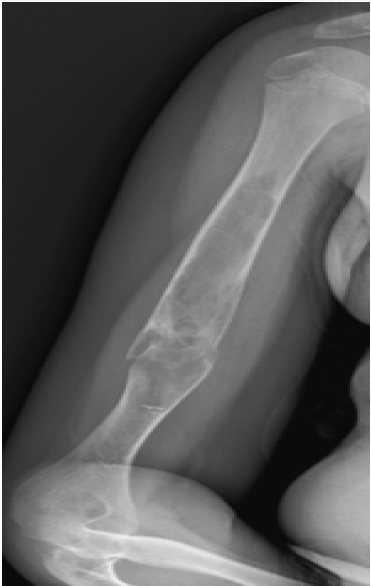
Figure 1: Radiograph of the pathological humerus fracture.
She had a known history of a large SBC in the right diaphyseal humerus, with a first pathological fracture occurring the year before after a trivial trauma as well. This fracture healed well conservatively. Magnetic resonance imaging 1 year before the fracture already confirmed the diagnosis of a large SBC, measuring 125 × 24 × 29 mm and thus expanding in most of the humeral diaphysis (Fig. 2).
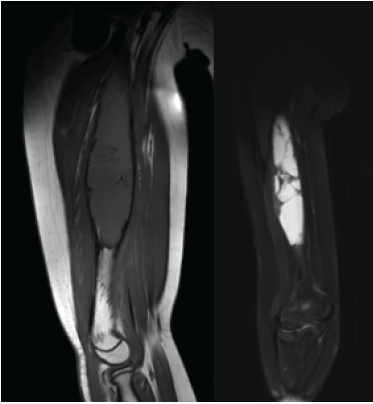
Figure 2: Magnetic resonance imaging of the large simple bone cyst 1 year before the fracture.
Surgical intervention was considered necessary because of the risk of recurrent pathological fracture in the future and to address the patient’s functional self-restriction and avoidance of sports participation. Conservative management through serial corticosteroid injections was dismissed, as this approach typically requires multiple interventions under general anaesthesia, particularly given the extensive volume of the cyst. Operatively, AGN1 was selected over traditional ESIN to provide immediate, rigid structural support without the need for future hardware removal. Furthermore, the use of this synthetic triphasic matrix was preferred over autologous bone grafting to eliminate donor site morbidity, which is particularly relevant in the paediatric population. Following detailed informed consent, the patient underwent curettage and grafting with AGN1 (Ossure™) in January 2023, 3 months after the fracture. A 1 cm stab incision over the fragile lateral humerus was used to create a cortical window for curettage, allowing access to the cyst while minimising soft-tissue disruption. Under fluoroscopic guidance, the cyst was carefully curetted to remove the inner lining of the lesion, followed by suction/irrigation to remove the debris. Cytological evaluation of the curettage material yielded only bloody fluid without atypical cells, confirming the benign, unicameral nature of the lesion. Following meticulous curettage and irrigation, the AGN1 implant was prepared according to the manufacturer’s instructions. Under fluoroscopic guidance, a total volume of 41 cc was injected through the cortical window, ensuring complete volumetric filling of the cystic cavity and direct contact with the inner cortical walls to maximise osteoconductive potential. The wound was closed with sutures. The AGN1 offers direct structural support as it completely hardens in 20 min, ensuring immediate stability. Unlike traditional non-resorbable polymeric bone cements, this triphasic calcium matrix functions as a fully resorbable, osteoconductive scaffold. Over the subsequent months, the material undergoes progressive resorption and is completely replaced by newly formed physiological bone, thereby ensuring early mechanical stability while eliminating the long-term risks associated with permanent inert implants. The post-operative rehabilitation protocol allowed for immediate active and passive range of motion of the shoulder and elbow to encourage rapid functional recovery. By 2 weeks postoperatively, the patient was completely pain-free and demonstrated a full, normal range of motion. To protect the humerus from peak loading during the initial integration phase, a removable brace was worn during higher-impact activities, and sports participation was strictly prohibited for a duration of 6 weeks. Beyond the 6-week mark, following clinical and radiographic confirmation of initial stability, all restrictions were lifted as tolerated. A baseline radiograph was taken the day after the surgery (Fig. 3).
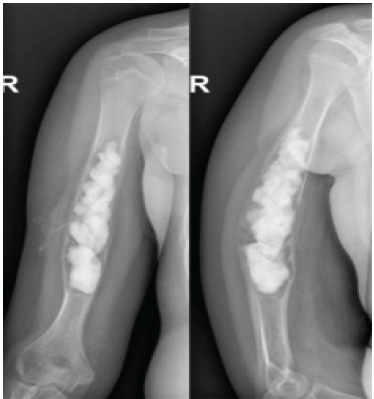
Figure 3: Radiograph of the humerus 1 day post-operative.
At 6 weeks there was already a partial bony incorporation of the AGN1 implant material with extensive periosteal callus formation (Fig. 4).
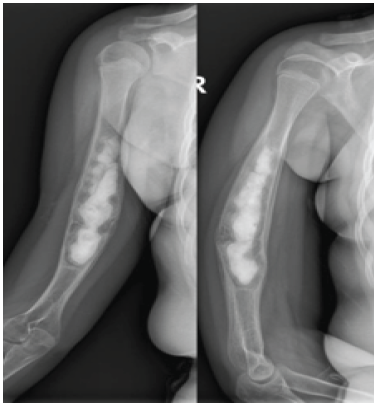
Figure 4: Radiograph of the humerus 6 weeks post-operative.
Serial radiographic imaging at 3 and 6 months postoperatively demonstrated progressive consolidation and global densification of the bone structure, indicating successful integration of the implant material (Fig. 5 and 6).
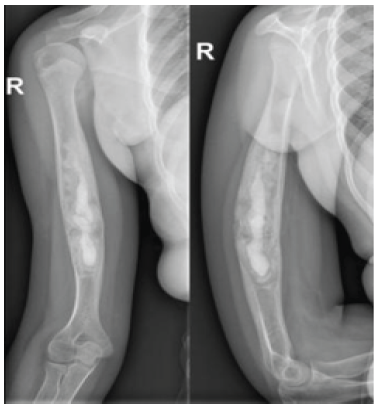
Figure 5: Radiograph of the humerus 3 months post-operative.

Figure 6: Radiograph of the humerus 6 months post-operative.
At the long-term follow-up in December 2025, almost 3 years postoperatively, plain radiographs were evaluated to objectively assess cyst healing. Imaging demonstrated substantial resorption of the AGN1 implant with restoration of a physiological trabecular bone architecture in the proximal humerus (Fig. 7).
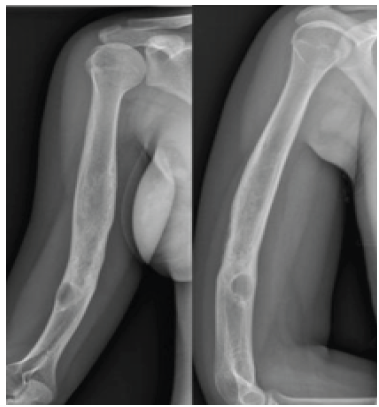
Figure 7: Radiograph of the humerus 3 years post-operative.
A residual radiolucency measuring 13 × 22 mm was noted in the distal aspect of the previously treated area. According to the validated Capanna criteria for bone cyst healing, this outcome is classified as Grade II (“healed with residual defect”) [9]. This static residual finding was clinically asymptomatic, required no further intervention, and did not compromise the overall biomechanical integrity of the humerus. This shows a remarkably fast stabilisation of the large cystic lesion, which in turn stimulated the surrounding bone to regenerate more effectively, leading to a notable enhancement in overall skeletal integrity.
The current treatments of SBCs have variable healing and recurrence rates, and to date, there is no superior treatment yet [10]. In a 2024 meta-analysis (including 4973 SBC’s), Ruiz-Alleramos found a success rate of 44.7% with conservative treatment in 387 patients [3]. However, because most cysts are incidental findings, observation remains the preferred treatment in asymptomatic cysts without risk of cortical thinning and pathological fracture. Scaglietti first described the injections of steroids in these lesions in 1979, with an initially high response in 90% of the patients [11]. These findings, however, were not replicated in subsequent studies. A Cochrane review of 2017 (only including one randomised controlled trial) showed that more children in the steroid injection group had radiographic healing compared to the bone marrow injection group (16/38 vs. 9/39, P = 0.01) after 2 years of follow-up, thus favouring steroid injections, which are also less invasive than bone marrow injections [1,12]. These treatments often involve multiple injections, each requiring hospitalisation and general anaesthesia for the child, resulting in significant physical and emotional impact. Ruiz-Arellanos, however, found a lower success rate for corticosteroid injections at 63.81% versus 70.35% for bone marrow injections [3,13]. A decision analysis favoured injections with bone marrow. Performing a decompression of the cyst wall in combination with injections increased the success rate to 77.04% (vs. 62.37% without decompression). This suggests that decompressing the cyst wall after injection is more important than what specific compound is used for injection [3]. This finding also supports the venous theory as a plausible aetiology. Curettage is the most common intervention among members of the European Paediatric Orthopaedic Society and the Paediatric Orthopaedic Society of North America, as stated in a survey from 2020 [14]. The overall success rate is 79.97%, but success varies with the material used for packing the defect. Interestingly, autologous bone grafting, the most invasive option, had the least success with only 63.32%. Better success was seen with allografts (78.48%) and bone substitute materials such as calcium sulphate pellets (87.07%) [3]. The higher success of these bone substitutes compared to autografts could be explained by the absence of cytokines, which are considered a contributing factor for SBCs by inducing bone resorption [15]. Several systematic reviews and comparative studies have further highlighted the ongoing challenges in defining the most effective surgical approach for these lesions [16,17]. Comparing these established modalities reveals significant clinical trade-offs. Intralesional injections lack immediate biomechanical stability and frequently necessitate multiple interventions under general anaesthesia. Autologous bone grafting provides excellent osteogenesis but is inherently limited by donor site morbidity and restricted paediatric graft volume. While ESIN offers excellent mechanical stabilisation (success rates up to 91.16% with primary curettage), it remains highly invasive and necessitates a secondary surgical procedure for hardware removal [3,14]. In this context, an off-the-shelf synthetic biomaterial that couples immediate load-bearing capabilities with physiological remodelling effectively bridges the gap between purely biological (injections/grafts) and purely mechanical (ESIN) interventions. The AGN1 used in our case has previously been studied in the context of osteoenhancement procedures in hip fracture prevention in osteoporosis or after removal of hip implants. It is a triphasic resorbable material (calcium sulphate, brushite, and beta-tricalcium phosphate [TCP] granules) that hardens in 20 min without exceeding 35°C to prevent thermal damage to the bone [7]. When hard, it provides an immediate increase in bone strength compared to the pre-implantation state, as proved in a cadaveric study on proximal femurs [5]. The resorption that follows leaves an open-pore structure promoting bone ingrowth on the beta-TCP granules, which works as a scaffold for new bone formation [7]. These properties of AGN1 offer a dual benefit: early mechanical support within 1 h after surgery and long-term bone reinforcement through progressive resorption. These findings have been validated in animal as well as human studies, with complete resorption of the material [4,6,8,18]. A prospective cohort study of LOEP procedures in 12 patients confirmed these findings in humans: AGN1 was safe to use and strengthened the femoral neck on a bone mineral density scan by 68% after 12 weeks. After 24 weeks, 83% of the product was resorbed, with 100% resorption by the end of the follow-up period on a computed tomography scan (5–7 years) [6]. Our long-term follow-up of nearly 36 months clinically validates these resorption kinetics in a paediatric patient; the implant material was completely replaced by physiologically structured bone. The presence of a small distal residual cyst highlights the natural history of SBCs but remained clinically silent due to the robust cortical and trabecular reinforcement provided by the initial osteoenhancement. In our case, the use of AGN1 provided immediate biomechanical stability and led to rapid cyst healing, aligning with previous findings on its osteo-enhancing properties. However, potential disadvantages of this novel technique must be acknowledged, including the current lack of extensive paediatric safety data and the learning curve required for precise fluoroscopic-guided implantation. The patient’s early functional recovery and radiographic evidence of complete integration within 3 months suggest that AGN1 may offer a valuable alternative to traditional bone grafting techniques, particularly in cases where immediate structural support is desired. However, this report is inherently limited by its single-case design and the complete absence of comparative data. While the outcomes in this specific patient are promising, generalisability to all paediatric SBCs cannot be assumed. Future larger, prospective comparative studies are strictly required to establish its definitive long-term efficacy, optimal indications, and how it directly compares against established SBC treatment modalities.
To the best of our knowledge, this case represents the first reported clinical application of AGN1 in the treatment of a large paediatric SBC. While the rapid functional recovery and robust long-term bone regeneration (with Capanna Grade II healing at nearly 3 years) observed in this single patient are highly encouraging, these findings must be interpreted with appropriate caution. Due to the inherent limitations of a case report, the broader efficacy and generalisability of this approach remain unproven. Larger, controlled comparative studies are necessary to definitively confirm whether AGN1 can routinely serve as a safe and superior treatment option for fracture-prone SBCs compared to current standard therapies.
This case demonstrates that AGN1 can safely replace bone grafts in the operative treatment of cavitated paediatric bone cysts. By providing immediate stability and complete resorption, it offers a highly effective, less invasive surgical alternative.
References
- 1. Zhao JG, Wang J, Huang WJ, Zhang P, Ding N, Shang J. Interventions for treating simple bone cysts in the long bones of children. Cochrane Database Syst Rev 2017;2:CD010847. [Google Scholar] [PubMed]
- 2. Donaldson S, Wright JG. Simple bone cysts: Better with age? J Pediatr Orthop 2015;35:108-14. [Google Scholar] [PubMed]
- 3. Ruiz-Arellanos K, Larios F, Inchaustegui ML, Gonzalez MR, Pretell-Mazzini J. Treatment and outcomes of 4,973 unicameral bone cysts: A systematic review and meta-analysis. JBJS Rev 2024;12:e00159. [Google Scholar] [PubMed]
- 4. Shaul JL, Hill RS, Bouxsein ML, Burr DB, Tilton AK, Howe JG. AGN1 implant material to treat bone loss: resorbable implant forms normal bone with and without alendronate in a canine critical size humeral defect model. Bone 2022;154:116246. [Google Scholar] [PubMed]
- 5. Stroncek JD, Shaul JL, Favell D, Hill RS, Huber BM, Howe JG, et al. In vitro injection of osteoporotic cadaveric femurs with a triphasic calcium‐based implant confers immediate biomechanical integrity. J Orthop Res 2019;37:908-15. [Google Scholar] [PubMed]
- 6. Howe JG, Hill RS, Stroncek JD, Shaul JL, Favell D, Cheng RR, et al. Treatment of bone loss in proximal femurs of postmenopausal osteoporotic women with AGN1 local osteo-enhancement procedure (LOEP) increases hip bone mineral density and hip strength: A long-term prospective cohort study. Osteoporos Int 2020;31:921-9. [Google Scholar] [PubMed]
- 7. Guido D, Raspanti F, Gabbiani N, Innocenti M, Civinini R. Osteo-enhancement procedures in hip fracture prevention: Definition and local interventions. Int J Bone Fragility 2022;2:16-9. [Google Scholar] [PubMed]
- 8. Shaul J, Hill R, Bruder S, Tilton A, Howe J. Triphasic calcium‐based implant material resorbs and is replaced with bone in ovariectomised rats with or without bisphosphonate treatment. J Orthop Res 2022;40:2271-80. [Google Scholar] [PubMed]
- 9. Capanna R, Dal Monte A, Gitelis S, Campanacci M. The natural history of a unicameral bone cyst after steroid injection. Clin Orthop Relat Res 1982;166:204-11. [Google Scholar] [PubMed]
- 10. Pala E, Trovarelli G, Angelini A, Cerchiaro MC, Ruggieri P. Modern treatment of unicameral and aneurysmatic bone cysts. EFORT Open Rev 2024;9:387-92. [Google Scholar] [PubMed]
- 11. Scaglietti O, Marchetti PG, Bartolozzi P. The effects of methylprednisolone acetate in the treatment of bone cysts. Results of three years of follow-up. J Bone Joint Surg Br 1979;61-B:200-4. [Google Scholar] [PubMed]
- 12. Wright JG, Yandow S, Donaldson S, Marley L, Simple Bone Cyst Trial Group. A randomised clinical trial comparing intralesional bone marrow and steroid injections for simple bone cysts. J Bone Joint Surg Am 2008;90:722-30. [Google Scholar] [PubMed]
- 13. Lee SY, Chung CY, Lee KM, Sung KH, Won SH, Choi IH, et al. Determining the best treatment for a simple bone cyst: A decision analysis. Clin Orthop Surg 2014;6:62-71. [Google Scholar] [PubMed]
- 14. Farr S, Balacó IM, Martínez-Alvarez S, Hahne J, Bae DS. Current trends and variations in the treatment of unicameral bone cysts of the humerus: A survey of EPOS and POSNA members. J Pediatr Orthop 2020;40:e68-76. [Google Scholar] [PubMed]
- 15. Aarvold A, Smith JO, Tayton ER, Edwards CJ, Fowler DJ, Gent ED, et al. The role of osteoblast cells in the pathogenesis of unicameral bone cysts. J Child Orthop 2012;6:339-46. [Google Scholar] [PubMed]
- 16. Kadhim M, Thacker M, Kadhim A, Holmes L Jr. Treatment of unicameral bone cyst: Systematic review and meta-analysis. J Child Orthop 2014;8:171-91. [Google Scholar] [PubMed]
- 17. Hou HY, Wu K, Wang CT, Chang SM, Lin WH, Yang RS. Treatment of unicameral bone cysts: A comparative study of selected techniques. J Bone Joint Surg Am 2010;92:855-62. [Google Scholar] [PubMed]
- 18. De Schepper J, Howe JJ. A surgical procedure to deliver a triphasic calcium-based implant material to address local bone loss and strengthen an osteoporotic proximal femur: A case report. Int J Bone Fragility 2022;2:77-9. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Revision Reconstruction of a Humeral Simple Bone Cyst Using Fibular Strut Graft, Iliac Crest Bone Graft, and Posterior Plating in a Young Adult: A Case Report
June 1, 2026 Revision Reconstruction of a Humeral Simple Bone Cyst Using Fibular Strut Graft, Iliac Crest Bone Graft, and Posterior Plating in a Young Adult: A Case Report February 1, 2026 Symptomatic Fatty Involution of a Simple Bone Cyst in the Proximal Humerus: A Rare Case Report
February 1, 2026 Symptomatic Fatty Involution of a Simple Bone Cyst in the Proximal Humerus: A Rare Case Report October 10, 2022 Proximal Phalanx Enchondroma with Pathological Fracture Treated with Curettage and Bone Substitute Placement – A Case Report
October 10, 2022 Proximal Phalanx Enchondroma with Pathological Fracture Treated with Curettage and Bone Substitute Placement – A Case Report June 6, 2021 A Case Report of Penetrating Extremity Trauma: A Near Miss Encounter
June 6, 2021 A Case Report of Penetrating Extremity Trauma: A Near Miss Encounter