
Compared to high-speed drill, piezoelectric surgery demonstrates superior safety and efficiency in cervical laminectomy.
Dr. Ahmed Jahwari, Department of Orthopaedics, Medical City for Military and Security Services, Muscat, Oman. E-mail: spinemcmss@gmail.com
Abstract
Introduction: Piezoelectric bone surgery is an emerging technique that facilitates the selective cutting of mineralised tissue while preserving soft tissue integrity. Conventional tools such as the high-speed drill (HSD) and Kerrison rongeur are associated with complications, such as dural tears and neurovascular injury. This study compares intraoperative and post-operative (operative time, blood loss, complications, and post-operative pain) outcomes of cervical laminectomy performed using piezoelectric surgery (PS) versus high-speed drilling.
Materials and Methods: A prospective comparative study was done, including forty-two patients with cervical spondylotic myelopathy, who were enrolled from January 2019 to January 2025 for standard laminectomy levels from C3 to C6. They were allocated into two groups using the alternating allocation method. Twenty-one underwent primary laminectomy using a piezoelectric device (Piezotome), and twenty-one underwent laminectomy using an HSD.
Results: The piezoelectric group (n = 21; 8 women, 13 men) had a mean age of 63 years and a mean Japanese Orthopaedic Association (mJOA) pre-operative score of 12.4 ± 2.4. The HSD group (n = 21; 5 women, 16 men) had a mean age of 61.2 years and a mJOA score of 12.2 ± 2.8. Laminectomy time per level was significantly shorter in the piezoelectric group (2.2 ± 0.8 min) compared to the HSD group (6.4 ± 2.2 min). Mean blood loss (after subtracting irrigated amount of normal saline) was 220 mL in the piezoelectric group versus 412 mL in the HSD group. No dural tears occurred in the piezoelectric group, while two were reported in the HSD group. Post-operative pain (visual analogue scale at 24 h) was also lower in the piezoelectric cohort (P < 0.05).
Conclusion: PS demonstrates superior safety and efficiency in cervical laminectomy, with reduced operative time, blood loss, and complication rates compared to traditional high-speed drilling.
Keywords: Piezoelectric, high-speed burr, high-speed drill, spondylotic myelopathy.
Cervical spondylotic myelopathy (CSM) is a prevalent degenerative spinal condition affecting the elderly population, characterised by progressive spinal cord compression leading to neurological deficits. Surgical decompression, particularly multilevel cervical laminectomy, remains the gold standard treatment in patients with moderate to severe symptoms. The goals of surgery include relief of spinal cord compression, prevention of further neurological decline, and restoration of functional capacity. Conventionally, tools, such as the high-speed drill (HSD) and Kerrison rongeur, have been employed for bony decompression. While effective, these instruments pose a risk of inadvertent injury to the dura mater and nearby neurovascular structures. Studies have shown that the rotational energy and thermal output generated by HSDs may cause collateral damage, especially in confined operative fields. Complication rates associated with HSDs range from 3% to 10%, depending on the level of surgical experience, anatomy, and intraoperative conditions [1,2]. Piezoelectric bone surgery employs ultrasonic microvibrations that selectively cut mineralised tissue while preserving adjacent soft tissues. This selective cutting mechanism has been shown to significantly reduce iatrogenic soft tissue injury compared to conventional rotary instruments [3]. Recent comparative studies in spinal surgery have demonstrated reduced intraoperative blood loss [4], shorter operative times [5], and lower complication rates [6] when using ultrasonic bone scalpels compared to HSD. In addition, piezoelectric surgery (PS) has demonstrated biological advantages, including improved osteogenesis and preservation of cellular viability, which may enhance post-operative healing [7,8]. Clinical studies have also reported improved surgical field visibility due to reduced bleeding [9], contributing to safer decompression procedures. Despite these advantages, its application in cervical spine surgery remains relatively underexplored. This study aims to compare intraoperative and post-operative outcomes between PS and high-speed drilling in cervical laminectomy.
A prospective comparative study was conducted at our institution by a single surgeon after ethics committee approval with the form (REC/MCMSS/2024/059). A total of forty-two patients diagnosed with CSM from January 2019 to January 2025, who were indicated for standard laminectomy C3-C6, were included. They were divided into two groups using the randomised alternating allocation method. Patients were divided into two equal groups: the piezoelectric group (n = 21). These patients underwent laminectomy using Piezotome (Fig. 1) and the HSD group (n = 21), where these patients underwent laminectomy using HSD (Fig. 2) and standard instruments.

Figure 1: Midas RexTM MR8TM high-speed drill system.

Figure 2: PIEZOSURGERY® plus (Mectron Medical).
The inclusion criteria for the study were as follows: Patients aged 40–75 years with a clinical and radiological diagnosis of CSM and no prior cervical spine surgery. Exclusion criteria were as follows: Patients with cervical spine trauma or tumours, and similarly, any prior cervical surgical intervention.
Operative technique:
A standard posterior midline approach was used. In the piezoelectric group, laminectomy was performed using a Piezotome, allowing selective bone cutting while preserving soft tissue [3]. In the HSD group, bone removal was performed using an HSD followed by Kerrison rongeurs. Data collection included demographic details, such as operative time per level (in minutes), intraoperative blood loss (in millilitres), dural tears, intraoperative neural injury, and postoperative pain (visual analogue scale [VAS] score at 24 h). Data were analysed using the Statistical Package for the Social Sciences software. Mean values were compared using an independent samples Student’s t-test and categorical variables using a chi-square test. P < 0.05 was considered with 95% standard deviation.
The demographic distribution was similar between groups. The piezoelectric group had a mean age of 63 years (8 females, thirteen males), and the HSD group had a mean age of 61.2 years (5 females, 16 males). Pre-operative modified Japanese Orthopaedic Association (mJOA) scores were comparable (12.4 ± 2.4 vs 12.2 ± 2.8). Laminectomy time per level was significantly shorter in the piezoelectric group (2.2 ± 0.8 min) compared to the HSD group (6.4 ± 2.2 min). Mean blood loss (after subtracting irrigated amount of normal saline) was 220 mL in the piezoelectric group versus 412 mL in the HSD group. No dural tears occurred in the piezoelectric group, while two were reported in the HSD group. Post-operative pain (VAS at 24 h) was also lower in the piezoelectric cohort (P < 0.05). (Table 1, bar charts 1 and 2, Figs. 3, 4, and 5).
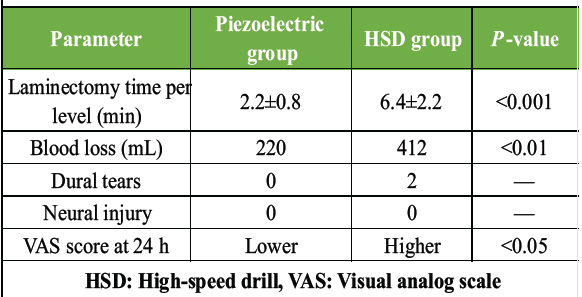
Table 1: Summary of operative outcomes
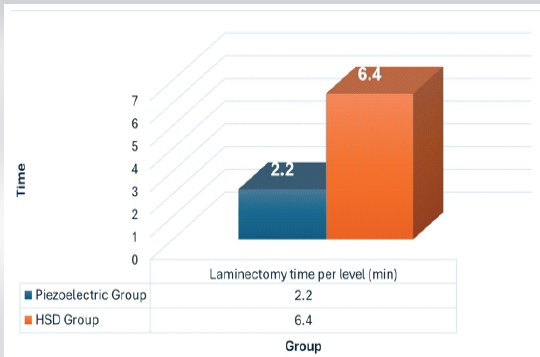
Bar Chart 1: Comparison of time.
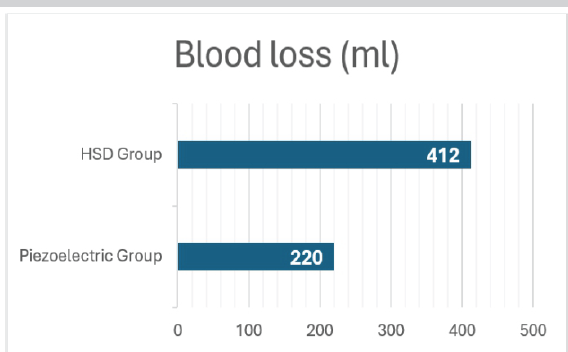
Bar Chart 2: Comparison of blood loss.
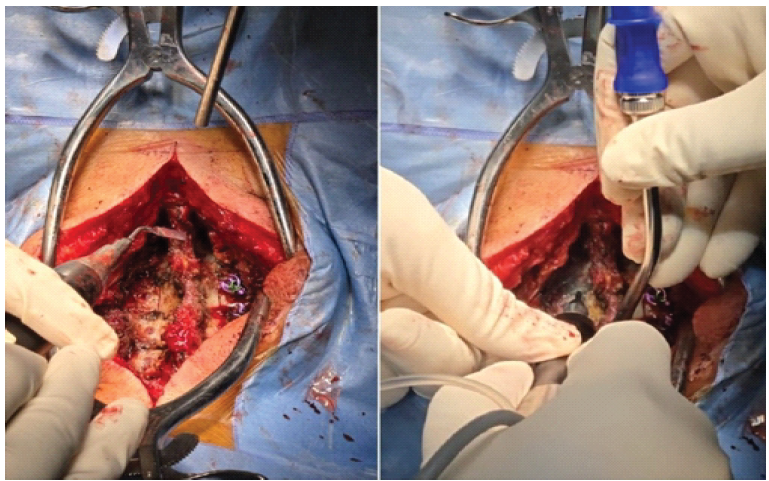
Figure 3: Use of PIEZOSURGERY® plus (Mectron Medical).
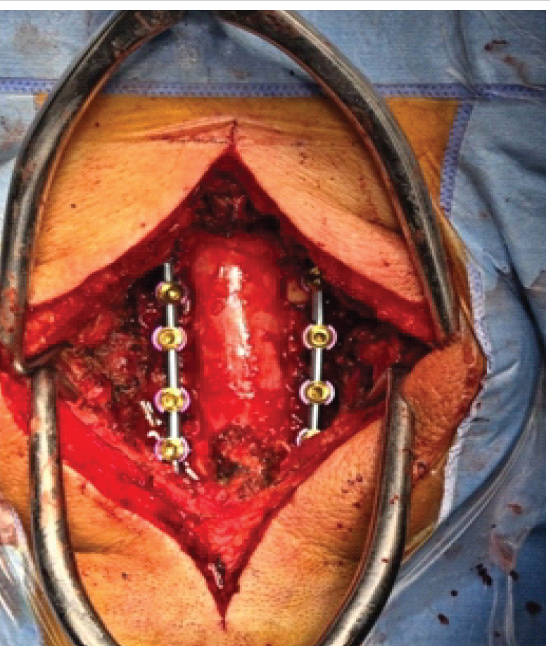
Figure 4: Completed laminectomy.
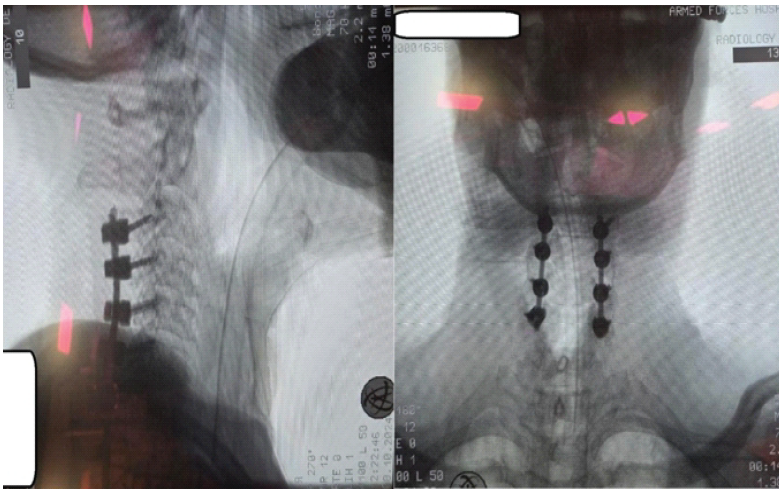
Figure 5: Intraoperative C-arm images of a sample patient who underwent C3-C6 laminectomy.
Our findings support growing evidence that ultrasonic bone scalpels improve surgical safety in spinal procedures. Studies have demonstrated reduced blood loss [4,9], improved precision [3], and decreased complication rates [6,10]. Our findings reinforce the growing body of evidence supporting the safety and efficacy of PS in spinal applications. The significantly reduced laminectomy time, along with decreased blood loss and a lower incidence of complications, suggests that piezoelectric tools offer tangible intraoperative advantages. Meta-analyses have further confirmed that ultrasonic devices are associated with lower rates of dural injury and improved perioperative outcomes compared to conventional drills [5,11]. The improved tactile feedback during PS has also been reported as an advantage. Surgeons can better feel resistance changes, which enhances safety when approaching the dura or nerve roots. This is particularly beneficial in revision cases or when anatomical variants are present, as surgical landmarks may be altered. We hypothetically presume that the learning curve will be faster [12]. Recent randomised and multicentre studies have also shown consistent improvements in operative efficiency and safety profiles [13]. While our study highlights the favourable operative profile of piezoelectric instruments, it also acknowledges potential limitations. The technique requires familiarity and a short learning curve. In addition, some authors have reported prolonged cutting time in sclerotic bone or when operating over large surface areas, although this was not a significant limitation in our cohort. The cost of acquisition and maintenance may also limit accessibility in lower-resource settings. Nonetheless, given the improved safety profile, lower risk of soft tissue damage, and enhanced recovery outcomes, the investment may be justified, particularly in centres with high spine surgery volumes.
Limitation:
An ideal study would have yielded more accurate results if it had been multicenter, involving multiple surgeons. Demographic data, medical comorbidities, age, and gender were not matched in each group. These were the limitations of our study.
In conclusion, piezoelectric bone surgery offers clinical advantages over traditional high-speed drilling in cervical spine laminectomy. Our study demonstrates that this technique results in significantly reduced operative time and blood loss (after subtracting the irrigated amount of normal saline), as well as lower rates of complications, such as dural tears. In addition, patients in the piezoelectric group experienced less post-operative pain, which could translate into improved recovery profiles and shorter hospital stays. Given its precision, safety profile, and biological advantages, PS has the potential to become a preferred method for spinal decompression, particularly in anatomically delicate regions such as the cervical spine. Further multicenter, randomised controlled studies are recommended to validate these findings and explore long-term outcomes, cost-effectiveness, and learning curves associated with broader clinical adoption.
Piezoelectric surgery demonstrates superior safety and efficiency in cervical laminectomy, with reduced operative time, blood loss, and complication rates compared to traditional high-speed drilling
References
- 1. Chen X, Zhang L, Liu H, Wang Q, Yang H. Application of ultrasonic bone scalpel in cervical laminectomy: A systematic review and meta-analysis. World Neurosurg 2023;174:e362-71. [Google Scholar] [PubMed]
- 2. Li Z, Wang H, Chen G, Zhang Y. Clinical outcomes of ultrasonic bone scalpel versus high-speed drill in spinal decompression: A comparative study. Eur Spine J 2022;31:2135-43. [Google Scholar] [PubMed]
- 3. Wang T, Liu S, Zhao Y, Sun C. Safety and efficacy of ultrasonic osteotome in cervical spine surgery: A prospective cohort study. Spine J 2021;21:1462-70. [Google Scholar] [PubMed]
- 4. Zhou X, Li F, Chen Z, Liu Z. Ultrasonic bone scalpel reduces complications in cervical decompression surgery: A retrospective comparative study. J Orthop Surg Res 2021;16:421. [Google Scholar] [PubMed]
- 5. Wu D, Wang F, Zhang Y.. Ultrasonic bone curette versus high-speed drill in spinal surgery: A meta-analysis of clinical outcomes. Medicine (Baltimore) 2022;101:e29045. [Google Scholar] [PubMed]
- 6. He B, Yan L, Guo H, Liu T, Wang X, Hao D., et al. Application of piezosurgery in spinal surgery: A systematic review of safety and clinical outcomes. Front Surg 2022;9:892345. [Google Scholar] [PubMed]
- 7. Kim CH, Chung CK, Choi Y, Kuo CC, Lee U, Yang SH, et al. Reduced intraoperative blood loss using ultrasonic bone scalpel in posterior cervical decompression: A randomized controlled trial. Clin Spine Surg 2024;37:E95-101. [Google Scholar] [PubMed]
- 8. Krishnan A, Samal P, Mayi S, Degulmadi S, Rai RR, Dave B. [Google Scholar] [PubMed]
- 9. Thoracic spine stenosis: does ultrasonic osteotome improve outcome in comparison to conventional technique? Malays Orthop J. 2021;15:62–69. [Google Scholar] [PubMed]
- 10. Dave BR, Krishnan A, Rai RR, Degulmadi D, Mayi S, Gudhe M. [Google Scholar] [PubMed]
- 11. The Effectiveness and Safety of Ultrasonic Bone Scalpel Versus Conventional Method in Cervical Laminectomy: A Retrospective Study of 311 Patients. Global Spine J. 2020;10(6):760–766. [Google Scholar] [PubMed]
- 12. Renjith KR, Eamani NK, Raja DC, Shetty AP. Ultrasonic bone scalpel in spine surgery. J Orthop. 2023;41:1–7. doi:10.1016/j.jor.2023.05.002 [Google Scholar] [PubMed] [CrossRef]
- 13. Sun J, Li Y, Zhao Z, Wang Q. Clinical efficacy and safety of ultrasonic bone scalpel in posterior cervical decompression surgery: A randomized controlled study. Spine (Phila Pa 1976) 2022;47:1285-92. [Google Scholar] [PubMed]
- 14. Wu L, Wang S.Effect of Ultrasonic Osteotome on Therapeutic Efficacy and Safety of Spinal Surgery: A System Review and Meta-Analysis. Comput Math Methods Med. 2022;2022:9548142. doi:10.1155/2022/9548142. [Google Scholar] [PubMed] [CrossRef]
- 15. Kumar V, Neradi D, Salaria AK, Dagar A, Singh S, Sharma G. [Google Scholar] [PubMed]
- 16. Role of Ultrasonic Bone Scalpel in Spine Surgery: a Review Article. SN Comprehensive Clinical Medicine. 2020;2:1883–1889Park [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Bilateral Tendoachilles Xanthoma in a Young Female: A Rare Case Report
September 1, 2025 Bilateral Tendoachilles Xanthoma in a Young Female: A Rare Case Report September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber
September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber May 1, 2025 A Rare Case of Bilateral Xanthomatosis of Tendon of Achilles: A Case Report
May 1, 2025 A Rare Case of Bilateral Xanthomatosis of Tendon of Achilles: A Case Report December 10, 2021 Recurrent Giant Cell Tumor of Distal Radius with Pulmonary Metastasis: A Case Report
December 10, 2021 Recurrent Giant Cell Tumor of Distal Radius with Pulmonary Metastasis: A Case Report