
In polyskeletal trauma, individualised staged fixation based on physiology, associated injuries, soft-tissue status, and rehabilitation goals provides safer outcomes than rigid fixation algorithms.
Dr. S Depak Charan, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: depakcharan@yahoo.in
Abstract
Introduction: Polyskeletal trauma involving multiple long-bone fractures presents major challenges in deciding the sequence and timing of fracture fixation. While early total care may benefit physiologically stable patients, staged management based on damage control orthopaedics is often safer in complex trauma. Evidence guiding fracture sequencing remains limited. This study reviews five patients managed using individualised staged fixation strategies.
Materials and Methods: A retrospective case series was conducted at a tertiary trauma centre after institutional ethics committee approval (IEC Ref: CSP-MED/26/FEB/126/62; dated February 27, 2026). Five adult patients with fractures involving two or more long bones were included. Data were collected from case records, operative notes, and radiographs. Variables analysed included injury pattern, associated injuries, temporary stabilisation, timing of definitive fixation, fixation sequence, and early outcomes.
Results: All patients initially underwent damage control stabilisation using external fixation or splintage where indicated. Definitive fixation was performed in stages after physiological optimisation. Pelvic instability, pulmonary injury, cardiac contusion, metabolic comorbidity, soft-tissue compromise, and operative positioning influenced sequencing decisions. All patients achieved fracture stabilisation without major early implant-related complications.
Conclusion: Fracture sequencing in polyskeletal trauma should be individualised rather than protocol-driven. A staged approach guided by damage control orthopaedic principles allows safe definitive fixation while minimising systemic stress.
Keywords: Polyskeletal trauma, damage control orthopedics, multiple fractures, fracture fixation, case series.
Polyskeletal trauma describes injuries in which fractures occur in more than one long bone, usually after high-energy events, such as road traffic accidents or falls from height [1]. These injuries are frequently accompanied by additional systemic trauma, including thoracic injuries, abdominal trauma, traumatic brain injury, or circulatory instability, which makes treatment planning more complex. Trauma remains one of the major causes of mortality in the younger population, and skeletal injuries contribute substantially to long-term disability among survivors [1,2,3]. Previous epidemiological studies have shown that fractures of the femur and tibia represent a significant proportion of extremity injuries in polytrauma patients. When multiple long bones are fractured, the overall inflammatory response is greater, increasing the likelihood of complications, such as pulmonary dysfunction, delayed fracture healing, and systemic inflammatory response syndrome [4,5,6]. Historically, the concept of early total care promoted immediate definitive fixation of major fractures to facilitate mobilisation and reduce complications. However, further research demonstrated that extensive early surgery may aggravate physiological stress in severely injured patients. This led to the development of the Damage Control Orthopaedics (DCO) approach, where temporary stabilisation is performed initially, and definitive procedures are delayed until the patient’s physiological condition improves [7,8,9,10]. (Table 1). In patients with multiple skeletal injuries, the surgeon must also decide the order in which fractures should be fixed, which can depend on factors such as haemodynamic stability, associated injuries, soft-tissue damage, and surgical positioning requirements. Because clear guidelines for fracture sequencing remain limited, decision-making often relies on clinical judgement and experience. This report presents five cases of polyskeletal trauma managed with staged fixation, highlighting practical considerations that influenced the sequence and timing of definitive fracture stabilisation.
This retrospective case series was conducted at a tertiary trauma centre after approval from the institutional ethics committee (IEC Ref: CSP-MED/26/FEB/126/62; dated February 27, 2026). Adult patients presenting with fractures involving at least two long bones were included. Patients with isolated fractures or incomplete documentation were excluded. Information was obtained from hospital case records, operative notes, and radiological investigations. Data collected included patient demographics, mechanism of injury, fracture distribution, associated injuries, temporary stabilisation techniques, timing of definitive fixation, and early postoperative outcomes. Initial management in all cases followed the principles of DCO, with temporary stabilisation using external fixation or splintage when required. Definitive surgical procedures were carried out in stages after physiological stabilisation, taking into account the patient’s condition, associated injuries, and soft-tissue status (Table 1).
Case 1:
A 21-year-old male presented following a high-velocity accident with pubic symphysis diastasis and left sacroiliac disruption, an open segmental fracture of the distal femoral shaft, a left lateral malleolus fracture, and a fracture of the proximal phalanx of the second finger. Initial treatment included debridement of the open wound, application of knee-spanning external fixation, pelvic external fixation, and splintage of the ankle. After stabilisation of the patient’s general condition, definitive procedures were performed in stages. Pubic symphysis plating and ankle fixation were carried out after three days, followed by intramedullary nailing of the femur 1 week later. The finger fracture was treated non-operatively. (Figure 1)
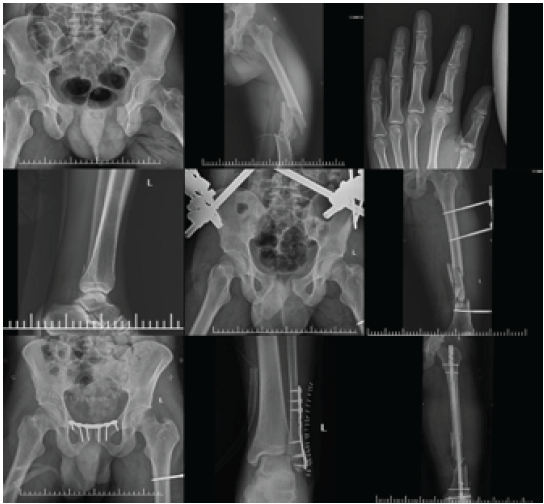
Figure 1 Case 1 – Sequential management of polyskeletal trauma demonstrating staged fixation strategy. (a) Pre-operative pelvic radiograph showing pubic symphysis diastasis with left sacroiliac joint disruption. (b) Pre-operative radiograph of the left femur demonstrating a distal third segmental femoral shaft fracture. (c) Pre-operative radiograph of the left hand showing fracture of the second proximal phalanx. (d) Pre-operative radiograph of the left ankle showing a lateral malleolus fracture. (e) Immediate post-initial surgery radiograph showing pelvic external fixation for temporary stabilization. (f) Radiograph following initial damage control orthopedics demonstrating left femur knee-spanning external fixation. (g) Post-operative radiograph after definitive fixation showing pubic symphysis plating. (h) Post-operative radiograph showing open reduction and internal fixation of the left lateral malleolus with plate osteosynthesis. (i) Final radiograph demonstrating definitive fixation of the left femoral shaft using an intramedullary interlocking nail. The sequence highlights prioritization of pelvic stabilization and soft-tissue management before definitive long-bone fixation.
Figure 1[1.1][DS1.2]:
A 59-year-old female with poorly controlled diabetes sustained bilateral femoral shaft fractures along with a comminuted fracture of the right proximal tibia. Initial damage control management involved external fixation of the left femur and knee-spanning external fixation on the right side. Definitive fixation was staged, beginning with plate fixation of the proximal tibia and intramedullary fixation of the ipsilateral femur after ten days. The contralateral femur was treated with intramedullary nailing 2 weeks later. (Figure 2)

Figure 2 Case 2 – Staged fixation in bilateral femoral fractures with ipsilateral prioritization in the presence of metabolic comorbidity. (a) Post-operative radiograph showing definitive fixation of the right femur using a long proximal femur nail. (b) Radiograph demonstrating alignment and fixation of the right femur following intramedullary stabilization. (c) Post-operative radiograph showing plate osteosynthesis of the comminuted right proximal tibial fracture. (d) Radiograph following initial damage control orthopedics demonstrating left femoral shaft fracture stabilized with external fixation. (e and f) Post-operative radiograph demonstrating definitive fixation of the left femoral shaft using an intramedullary interlocking nail. (g) Final radiograph showing bilateral femoral fixation following staged surgical management. The sequence highlights prioritization of ipsilateral fracture fixation to facilitate early weight bearing, with delayed definitive fixation of the contralateral limb due to metabolic comorbidity and infection risk.
Case 3:
A 35-year-old male sustained a distal third fracture of both bones of the left leg, a right subtrochanteric femur fracture, a posterior column acetabular fracture, and a comminuted patella fracture. Temporary stabilisation included external fixation of the femur and ankle. One week later, intramedullary nailing of the tibia and open reduction with internal fixation of the acetabulum were performed. Intramedullary fixation of the femur was completed during the following week. (Figure 3)

Figure 3 Case 3 – Staged fixation in polyskeletal trauma demonstrating positioning-based sequencing for acetabular surgery. (a) Pre-operative pelvic radiograph showing right acetabular posterior column fracture. (b) Pre-operative radiograph of the right femur demonstrating a subtrochanteric fracture. (c) Pre-operative radiograph of the left leg showing a distal third both-bone fracture. (d) Pre-operative radiograph of the right knee showing a comminuted patella fracture. (e) Radiograph following initial damage control orthopedics demonstrating right femur external fixation. (f) Radiograph showing left lower limb stabilized with ankle-spanning external fixation. (g) Post-operative radiograph showing intramedullary interlocking nailing of the left tibia. (h) Post-operative pelvic radiograph demonstrating open reduction and internal fixation of the right acetabular posterior column. (i) Final radiograph showing definitive fixation of the right femur using an intramedullary interlocking nail. The sequence highlights prioritization of contralateral long-bone fixation to facilitate patient positioning for acetabular surgery, followed by staged definitive fixation.
Case 4:
A 25-year-old male presented with multiple injuries, including an open comminuted fracture of the distal femur, a tibial shaft fracture, pubic diastasis with sacroiliac disruption, a clavicle fracture, and an intra-articular distal radius fracture. Additional injuries included rib fractures and a cardiac contusion. Initial treatment consisted of wound debridement and knee-spanning external fixation. Definitive fixation was performed sequentially: distal femur plating and pelvic stabilisation were performed first, followed by tibial nailing and clavicle fixation, and finally distal radius plating. (Figure 4)
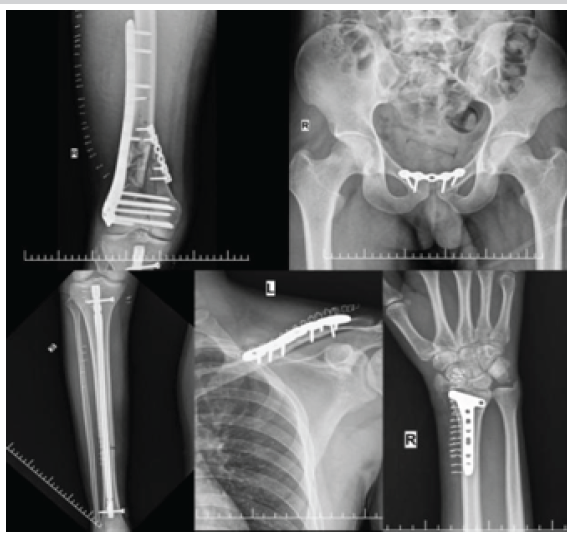
Figure 4 Case 4 – Staged fixation in severe polyskeletal trauma with prioritization based on systemic stability and associated injuries. (a) Post-operative radiograph showing open reduction and internal fixation of the right distal femur with plate osteosynthesis. (b) Post-operative pelvic radiograph demonstrating pubic symphysis plating for pelvic stabilization. (c) Radiograph showing definitive fixation of the right tibial shaft using an intramedullary interlocking nail. (d) Post-operative radiograph demonstrating plate osteosynthesis of the left midshaft clavicle fracture. (e) Post-operative radiograph showing open reduction and internal fixation of the right distal radius fracture. The sequence highlights prioritization of lower limb and pelvic stabilization, followed by upper limb fixation, with timing influenced by associated thoracic injuries and cardiac contusion.
Case 5:
A 24-year-old female sustained an open distal femoral fracture accompanied by fractures of the fourth and fifth metacarpals, pneumothorax, and aspiration pneumonitis. Initial management included wound debridement and temporary external fixation of the femur. After improvement in respiratory status, definitive distal femur plating was performed 4 days later. Skin grafting for the associated soft-tissue injury was carried out 1 week later. (Fig. 5)

Figure 5 Case 5 – Staged fixation in polyskeletal trauma influenced by associated pulmonary injury. (a) Pre-operative radiograph of the left distal femur showing an open comminuted distal femoral fracture. (b) Pre-operative radiograph of the left hand demonstrating fractures of the fourth metacarpal base and fifth metacarpal head. (c) Radiograph following initial damage control orthopedics showing left femur stabilized with knee-spanning external fixation. (d) Post-operative radiograph demonstrating definitive fixation of the left distal femur using plate osteosynthesis. The sequence highlights delayed definitive fixation due to associated pulmonary injury, emphasizing the role of physiological optimization before surgical intervention.
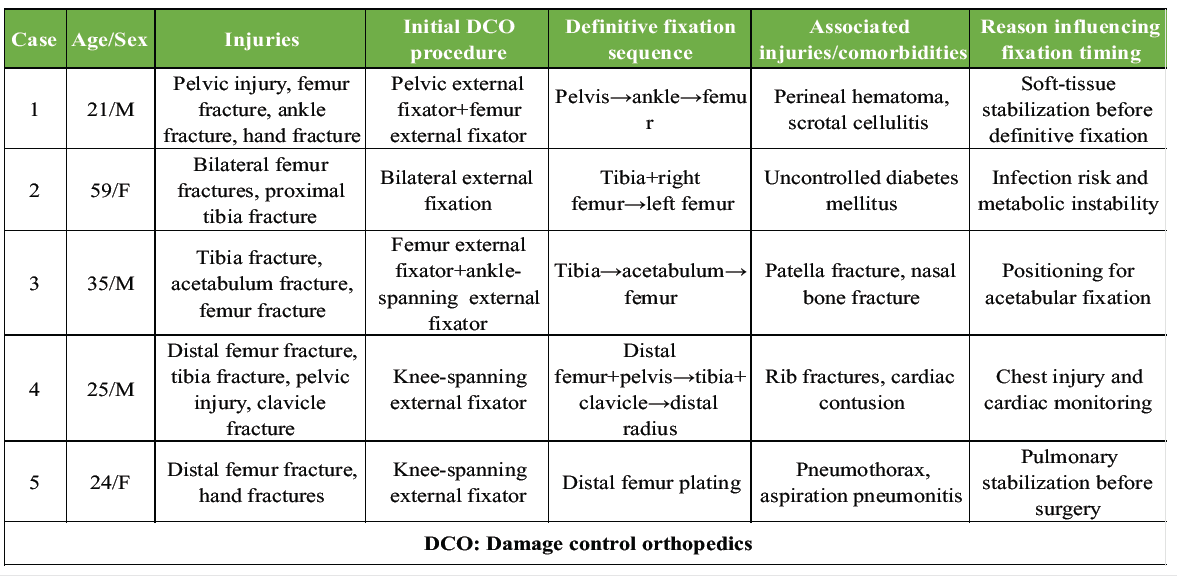
Table 1: DCO: Damage control orthopedics
Treatment of patients with multiple skeletal injuries requires balancing fracture stabilisation with the patient’s physiological reserve. While immediate complete fixation may suit stable patients, severely injured individuals often benefit from staged management based on DCO concepts [7,8,9,10]. In this series, pelvic instability was prioritised in selected patients to improve mechanical stability and simplify nursing care. Fractures affecting potential weight-bearing limbs were frequently addressed early to support rehabilitation. Chest trauma, cardiac contusion, uncontrolled diabetes, and soft-tissue compromise influenced delayed reconstruction to reduce perioperative risk. Operative logistics also affected sequencing. In one patient, stabilisation of the contralateral limb enabled safer positioning for acetabular surgery. Such practical factors are rarely emphasised in protocols but strongly influence real-world decisions. Prevention of fat embolism syndrome remains an important consideration in patients with multiple long-bone fractures. Early temporary stabilisation using external fixation or splintage helps reduce ongoing marrow embolisation and systemic inflammatory response. Adequate resuscitation, maintenance of oxygenation, correction of acidosis, and avoidance of prolonged surgical procedures in physiologically unstable patients are essential to minimise pulmonary and systemic complications. Recent literature recommends conversion to definitive fixation only after clinical and physiological optimisation, including haemodynamic stability and improvement of associated thoracic or systemic injuries. In the present series, staged fixation following temporary stabilisation allowed safer definitive reconstruction without major early implant-related complications [9,10]. These cases demonstrate that fracture sequencing should remain individualised rather than protocol-driven. Repeated physiological assessment, multidisciplinary care, and staged operative planning remain central to successful outcomes.
Strengths and limitations:
The major strength of this study is the presentation of real-world fracture sequencing strategies in patients with complex polyskeletal trauma managed using individualised staged fixation principles. The series highlights practical clinical decision-making based on patient physiology, associated injuries, soft-tissue conditions, rehabilitation goals, and operative considerations. Inclusion of varied injury patterns also demonstrates the adaptability of staged fixation strategies within the same damage control framework. However, this study has several limitations. The sample size was small and retrospective in nature, limiting generalisability. Functional outcomes and long-term follow-up were not uniformly available for all patients. In addition, heterogeneity of fracture patterns and associated injuries prevented direct comparison between cases. Larger prospective studies are required to establish standardised recommendations regarding optimal fracture fixation sequencing in polyskeletal trauma. Overall, these cases demonstrate that fracture sequencing should be individualised and guided by the patient’s clinical status rather than rigid protocols. [10]
Polyskeletal trauma presents significant challenges in determining the sequence and timing of fracture fixation. A staged surgical strategy based on damage control orthopaedic principles allows stabilisation of major injuries while minimising physiological stress. Careful evaluation of systemic condition, associated injuries, and operative requirements remains essential in planning fracture fixation in complex trauma patients.
In patients with multiple skeletal injuries, the order of fracture fixation should be tailored to physiology, associated injuries, and functional goals. Staged fixation often provides safer outcomes than immediate definitive fixation of all fractures.
1. Erne F, Ihle C, Ehnert S, Histing T, Nüssler AK, Maurer E. Distinct patient characteristics and risk profiles in upper vs lower leg fractures: Insights from a comprehensive cohort study. Diagnostics (Basel) 2025;16:11.
2. Steinfeld E, Horst K, Ansems K, Dahms K, Dormann J, Janka H, et al. Optimal timing of stabilisation and operative technique for extremity fractures in polytrauma patients: A systematic review and meta-analysis. Eur J Trauma Emerg Surg 2025;51:27.
3. Miller B, Phillips M, Krech L, Biberstein B, Parker J, Pounders S, et al. Outcomes of simultaneous versus staged intramedullary nailing fixation of multiple long bone lower extremity fractures. Injury 2023;54:110831.
4. Devendra A, Nishith PG, Dilip Chand Raja S, Dheenadhayalan J, Rajasekaran S. Current updates in management of extremity injuries in polytrauma. J Clin Orthop Trauma 2021;12:113-22.
5. Dattatri R, Jain VK, Iyengar KP, Vaishya R, Garg R. Anaesthetic considerations in polytrauma patients. J Clin Orthop Trauma 2021;12:50-7.
6. Upadhyaya GK, Iyengar KP, Jain VK, Garg R. Evolving concepts and strategies in the management of polytrauma patients. J Clin Orthop Trauma 2021;12:58-65.
7. Arnold SC, Lagazzi E, Wagner RK, Rafaqat W, Abiad M, Argandykov D, et al. Two big bones, one big decision: When to fix bilateral femur fractures. Injury 2024;55:11610.
8. Ajayakumar T, Nizaj N, Annie T, Lekshmi TP. Isolated cerebral fat embolism syndrome in a polytrauma patient with complete recovery – a case report. J Orthop Case Rep 2022;12:23.
9. Becker N, Hammen A, Bläsius F, Weber CD, Hildebrand F, Horst K. Effect of injury patterns on the development of complications and trauma-induced mortality in patients suffering multiple trauma. J Clin Med 2023;12:5111.
10. Iyengar KP, Venkatesan AS, Jain VK, Shashidhara MK, Elbana H, Botchu R. Risks in the management of polytrauma patients: Clinical insights. Orthop Res Rev 2023;15:27-38. [/references_numberd]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures
June 1, 2026 Comparison of Surgical Outcomes and Perioperative Laboratory Parameters Following Minimally Invasive Plate Osteosynthesis versus Conventional Plating in Long Bone Fractures May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing April 1, 2026 Bicolumnar Stabilization of Bicondylar Tibial Plateau Injuries: A Prospective Study of Combined Buttress Plate and Titanium Elastic Nail Fixation
April 1, 2026 Bicolumnar Stabilization of Bicondylar Tibial Plateau Injuries: A Prospective Study of Combined Buttress Plate and Titanium Elastic Nail Fixation April 1, 2026 Brown Tumors of Hyperparathyroidism: A 13-Year Retrospective Case Series from a Tertiary Center in South India
April 1, 2026 Brown Tumors of Hyperparathyroidism: A 13-Year Retrospective Case Series from a Tertiary Center in South India