
[box type=”bio”] Learning Point of the Article: [/box]
This article reports a new and esthetic surgical technique for metacarpal shaft fracture using a low-invasive simple locked wires fixator with a high degree of flexibility.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 66-69 | Yoichi Sugiyama, Kiyohito Naito, Nana Nagura, Kenji Goto, Kazuo Kaneko. DOI: 10.13107/jocr.2020.v10.i02.1700
Authors: Yoichi Sugiyama[1], Kiyohito Naito[1], Nana Nagura[1], Kenji Goto[1], Kazuo Kaneko[1]
[1]Department of Orthopaedics, Juntendo University School of Medicine, Tokyo, Japan.
Address of Correspondence:
Dr. Kiyohito Naito,
Department of Orthopaedics, Juntendo University, 1-5-29 Yushima, Bunkyo-ku, Tokyo 113-0034, Japan.
E-mail: knaito@juntendo.ac.jp
Abstract
Introduction: This article reports a case of metacarpal shaft fracture using a low-invasive simple locked wires fixator with a high degree of flexibility. A new surgical technique for this injury will also be presented.
Case Report: A 27-year-old female with the right 3rd metacarpal shaft fracture caused by falling down while riding a bicycle. The patient was a professional ballet dancer and requested treatment enabling an early return to exercise and non-noticeable wound. Pins were percutaneously inserted antegradely and retrogradely to the metacarpal bone as intramedullary pinning, then were connected using locked wires fixator. Post-operative immobilization was not necessary. The locked wire fixator was removed 6 weeks after surgery. Postoperatively, there were no limitations of the range of motion of the finger joints and the operative scar was almost unrecognizable.
Conclusion: This is a new breakthrough procedure facilitating. Furthermore, this surgical procedure may be selected as an esthetically useful method making a small wound because it can be percutaneously applied.
Keywords: Metacarpal shaft fracture, locked wires fixator, ballet dancer, intramedullary pinning.
Introduction
Metacarpal fractures are among the most commonly treated upper extremity injuries in adults and represent about 10% of all fractures [1]. The specific characteristics of each bone of the hand and the enhanced need for hand motion often complicate decision-making regarding the most appropriate method of treatment. Conservative treatment is selected for metacarpal shaft fractures in many cases, but surgical treatment is indicated for transverse fracture with dislocation and cases with rotatory deformity, shortening, and angular deformity [1]. The surgical methods include wire fixation, intramedullary pinning, screw fixation, and fixation with a locking plate that has recently been reported. Finger joint contracture is a problem with finger fracture treatment and it is important to select a treatment method enabling exercise therapy as early as possible after treatment. However, open surgery enabling early exercise therapy has problems, such as invasiveness, wound size, and risk of tendon damage and adhesion by implant, and no consensus viewpoint has been reached with regard to the selection of a treatment method [2]. This article reports a case of metacarpal shaft fracture using a low-invasive simple locked wires fixator with a high degree of flexibility, JuNction® (ARATA Co., Ltd., Tokyo, Japan). A new surgical technique for this injury will also be presented here.
Case Report
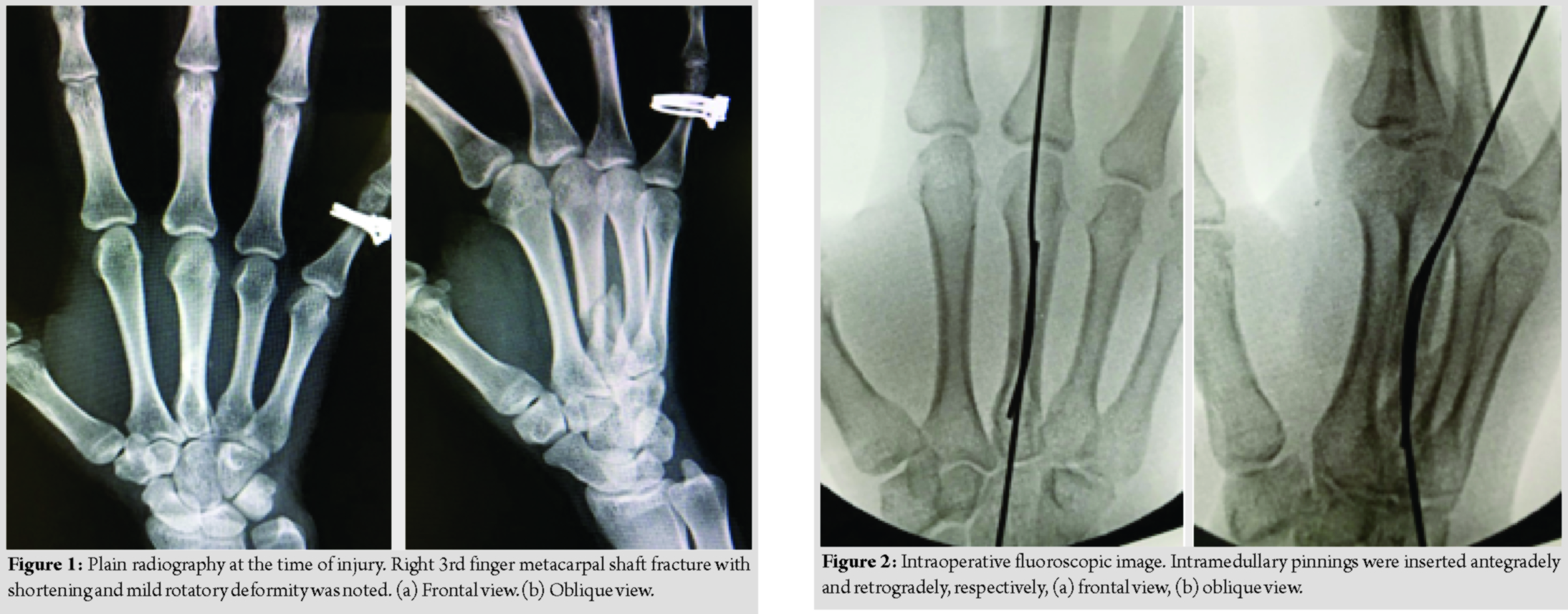
The patient was a 27-year-old female with the right 3rd metacarpal shaft fracture caused by falling down while riding a bicycle. On plain radiography, oblique fracture of the metacarpal shaft with shortening and mild rotatory deformity was noted (Fig. 1a and b). The patient was a professional ballet dancer and requested treatment enabling an early return to exercise and non-noticeable wound.
The locked wires fixator used, JuNction®, was comprised mini fixator pins (ARATA Co., Ltd., Tokyo, Japan), which are wire, and a box connecting the pins, “JuNction” (ARATA Co., Ltd., Tokyo, Japan). The concept of this medical device is the same as that of Meta-HUS® reported by Miyamoto et al. in 2015 [3], and it became available after approval by the Ministry of Health, Labour and Welfare in October 2017 in Japan.
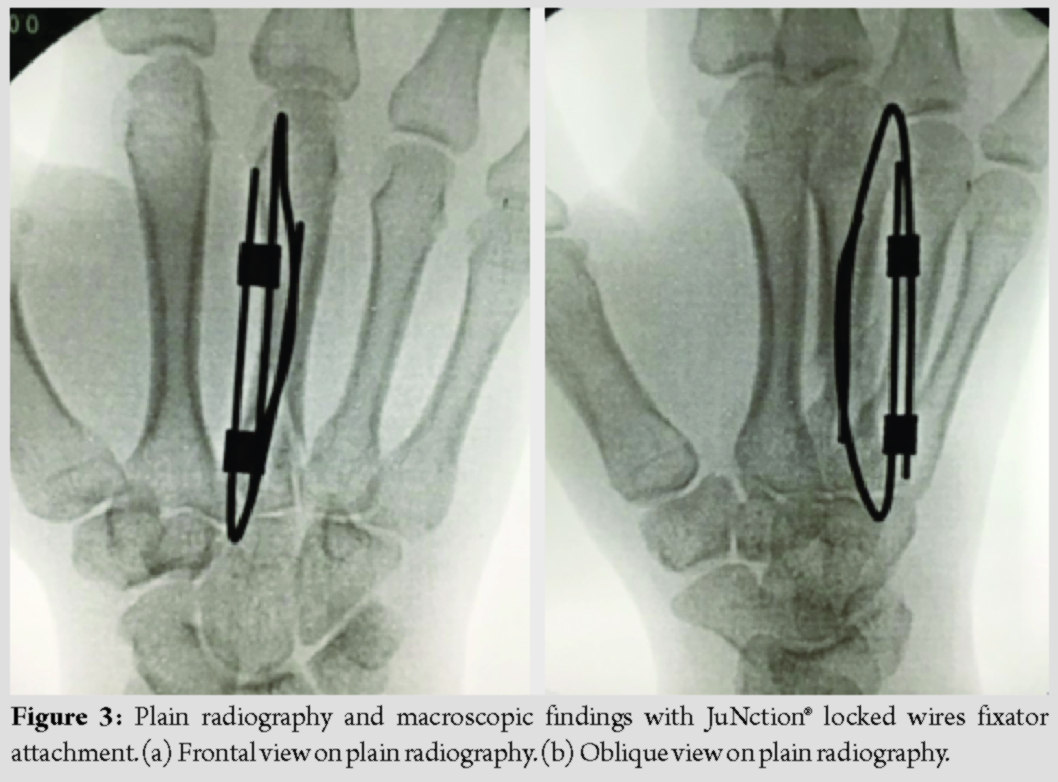
Surgery was performed under brachial plexus block 6 days after injury. A 1.2-mm mini fixator pin was percutaneously inserted antegradely from the base of the metacarpal bone as an intramedullary pinning and another 1.2-mm mini fixator pin was retrogradely inserted from a site proximal to the Metacarpophalangeal (MP) joint capsule of the metacarpal bone neck as intramedullary pinning (Fig. 2a and b). These pins were inserted through bone holes of cortex made of the same size pins. In addition, the inserted two mini fixator pins were connected using “JuNction” while retaining the manually reduced position to externally reduce and fix the fracture region (Fig. 3a and b). In this technique, the skin incision was not necessary because the pins were inserted percutaneously. The selection of wire diameter was dependent on the diameter of the medullary cavity of the metacarpal bone since two pins should be placed intramedullary. The c-arm is essential because intramedullary pinning was done by fluoroscopy. The operation time in this case was 30 min.
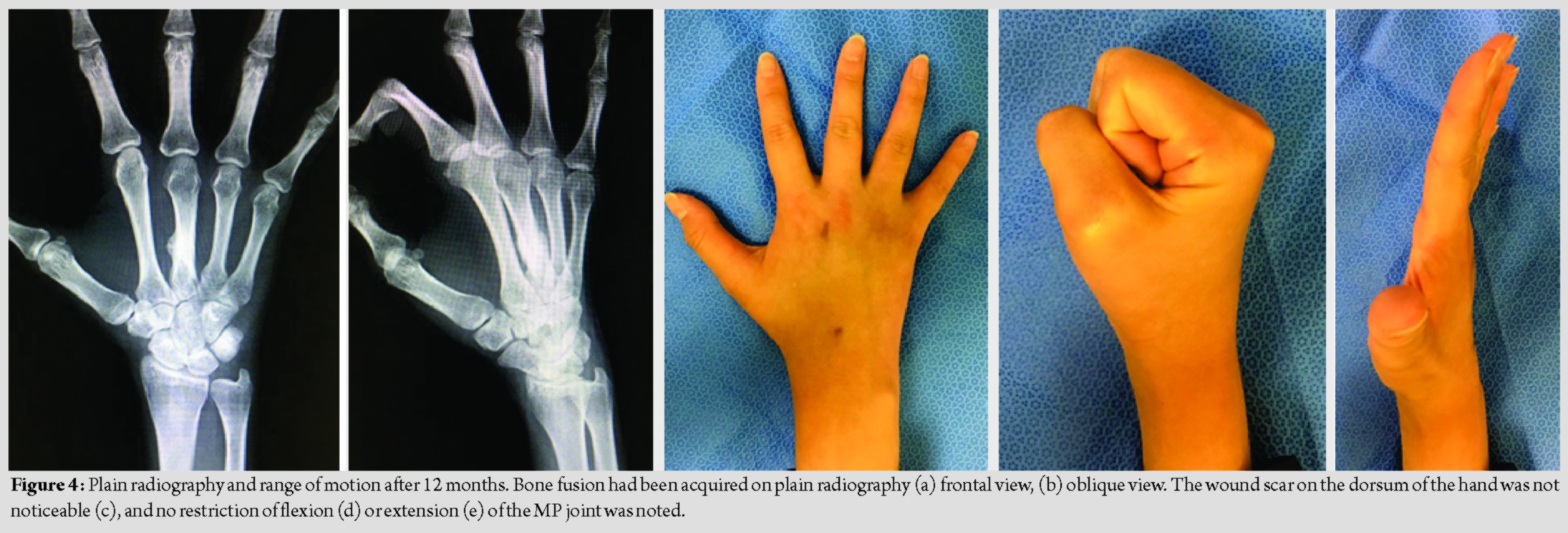
Post-operative immobilization was not necessary and the range of motion training was initiated with JuNction® attachment on the day following surgery. The JuNction and mini fixator pins were removed 6 weeks after surgery. On the final follow-up (12 months after surgery), bone fusion had been acquired without limitation of the range of motion of the finger joints including the MP joint, the patient had returned to a daily life and ballet dancing with VAS of 0/10 and Q-DASH of 2.27/100 without a problem (Fig. 4a-e).
Discussion
Various surgical methods for metacarpal shaft fractures have been reported [4,5]. Simple wire fixation, soft wire fixation, and intramedullary pinning require post-operative immobilization because the fixation force is insufficient and early initiation of range of motion training after surgery is difficult [6]. In contrast, strong fixation can be acquired by open surgery using a locking plate and range of motion training can be initiated early after surgery, but it has a risk for several complications. Reported complications of plate fixation include keloid scar formation of the wound region, adhesion of the extensor tendon, and joint contracture [7]. Screw fixation is a surgical procedure acquiring favorable fixation through a small skin incision, but it is not indicated for short oblique and transverse fractures into which a screw cannot be inserted. Moreover, Bouquet technique is a great way to get early mobility, but it still takes weeks of “buddy taping” to prevent malrotation [8]. The locked wires fixator we used is also suitable for the prevention of post-operative malrotation and basically there is no need for any taping. In general, the external fixator is used for open or comminuted fractures, severe soft-tissue damage, and comminuted intra-articular fractures. External fixation, which used to be bulky in the past, has been refined and expanded in recent years [9]. The locked wires fixator used in this case is a device capable of freely connecting pins which can be used more easily as compared with the conventional external fixator. The device is expected to expand its indication for fractures due to this simplicity. A biomechanical study on the fixing force of intramedullary rods suggested that rotational stability is improved by the insertion of several intramedullary rods [2]. It is also well-known that fixation is favorable as the rate of medullary cavity occupation by intramedullary rods increases [10]. In the present patient, the width of the narrowest region of the 3rd metacarpal bone was 2.5 mm on plain radiography. The medullary cavity occupation rate was to be 96% when two 1.2-mm mini fixator pins were inserted. There are 1.2, 1.5, and 1.8 mm mini fixator pins in JuNction® locked wire fixator adopted in this case and the device is applicable to a maximum of 3.6 mm medullary cavity in this surgical procedure, in which several wires were not inserted from a site proximal to the metacarpal bone, unlike Foucher’s modification, but two mini fixator pins were inserted from proximal and distal sites, respectively, as intramedullary pinning. This is a new breakthrough procedure facilitating: (1) Acquisition of a sufficient medullary cavity occupation rate for which favorable fixation of the fracture region can be expected and (2) prevention of postoperative malrotation through 1.2 mm × 2 = 2.4 mm rod formation externally by the two mini fixator pins. Furthermore, this surgical procedure may be selected as an esthetically useful method making a small wound because it can be percutaneously applied. Miyamoto et al. recommended the use of an external fixator, Meta-HUS®, which connects wires for fixation in treatment of 5thcarpometacarpaljoint dislocation fractures [3], because bone fragments can be strongly held compared with that in previous wire fixation and wires are inserted at the MP joint flexion position to permit finger movement early after surgery, expecting prevention of MP joint contracture. Furthermore, this external fixator is capable of freely connecting the wires, for which expansion of the indication for treatment of finger fractures may be expected. There are several limitations to this technique. First, the shortening of the metacarpal bone was not controlled. On the final follow-up (12 months after surgery), bone fusion had been acquired with the shortening of the third metacarpal bone (Fig. 4a). However, the limitation of the range of motion of the finger joints including the MP joint was not observed (Fig. 4c-e). It is considered that although the shortening of the metacarpal bone remained because the early movement was possible under the good fixing force of the locked wires fixator, the limitation of the range of motion did not occur. Furthermore, as with general percutaneous pinning, it is necessary to recognize the pin tract infection and the risk of the extensor tendon and superficial nerve injury or irritation.
Conclusion
This is a new breakthrough procedure facilitating. Furthermore, this surgical procedure may be selected as an esthetically useful method making a small wound because it can be percutaneously applied.
Clinical Message
Open surgery for metacarpal bone enabling early exercise therapy has problems, such as invasiveness, wound size, and risk of tendon damage and adhesion by an implant. This is a new breakthrough procedure facilitating. From this point of view, this surgical procedure may be selected as an esthetically useful method making a small wound because it can be percutaneously applied.
References
1. Corkum JP, Davison PG, Lalonde DH. Systematic review of the best evidence in intramedullary fixation for metacarpal fractures. Hand (N Y) 2013;8:253-60.
2. Hiatt SV, Begonia MT, Thiagarajan G, Hutchison RL. Biomechanical comparison of 2 methods of intramedullary K-wire fixation of transverse metacarpal shaft fractures. J Hand Surg Am 2015;40:1586-90.
3. Miyamoto H, Adi M, Taleb C, Zemirline A, Bodin F, Gay A, et al. Fifth carpometacarpal fracture dislocations fixed with Meta-HUS®: A series of 31 cases. Eur J Orthop Surg Traumatol 2015;25:477-82.
4 Al-Qattan MM, Al-Lazzam A. Long oblique/spiral mid-shaft metacarpal fractures of the fingers: Treatment with cerclage wire fixation and immediate post-operative finger mobilisation in a wrist splint. J Hand Surg Eur Vol 2007;32:637-40.
5. Downing ND, Davis TR. Intramedullary fixation of unstable metacarpal fractures. Hand Clin 2006;22:269-77.
6. Kollitz KM, Hammert WC, Vedder NB, Huang JI. Metacarpal fractures: Treatment and complications. Hand (N Y) 2014;9:16-23.
7. Facca S, Ramdhian R, Pelissier A, Diaconu M, Liverneaux P. Fifth metacarpal neck fracture fixation: Locking plate versus K-wire? Orthop Traumatol Surg Res 2010;96:506-12.
8. Foucher G. “Bouquet” osteosynthesis in metacarpal neck fractures: A series of 66 patients. J Hand Surg Am 1995;20:S86-90.
9. Dailiana Z, Agorastakis D, Varitimidis S, Bargiotas K, Roidis N, Malizos KN. Use of a mini-external fixator for the treatment of hand fractures. J Hand Surg Am 2009;34:630-6.
10. Zain Elabdien BS, Olerud S, Karlström G. Ender nailing of pertrochanteric fractures. Complications related to technical failures and bone quality. Acta Orthop Scand 1985;56:138-44.
 |
 |
 |
 |
 |
| Dr. Yoichi Sugiyama | Dr. Kiyohito Naito | Dr. Nana Nagura | Dr. Kenji Goto | Dr. Kazuo Kaneko |
| How to Cite This Article: Sugiyama Y, Naito K, Nagura N, Goto K, Kaneko K. Treatment for a Metacarpal Shaft Fracture using Locked Wire Fixator: A Case Report of New Surgical Technique. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 66-69. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


