
[box type=”bio”] Learning Point of the Article: [/box]
Syndromic association of Polyostotic FD can be difficult to diagnose sometimes and may present in an unusual fashion, a correct Clinico-Radio-Pathological evaluation helps in the correct diagnosis and hence allows us to give the most appropriate management.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 80-83 | Mishil Parikh, Ajay Puri, Amrita Guha, Kavita Khirwal, Ashish Gulia. DOI: 10.13107/jocr.2020.v10.i02.1708
Authors: Mishil Parikh[1], Ajay Puri[2], Amrita Guha[3], Kavita Khirwal[4], Ashish Gulia[2]
[1]Department of Musculoskeletal Oncology, Apollo Hospitals, Navi Mumbai, Maharashtra, India,
[2]Department of Surgical Oncology, Bone and Soft Tissue Services, Tata Memorial Hospital, Mumbai, Maharashtra, India,
[3]Department of Radiodiagnosis, Tata Memorial Hospital, Mumbai, Maharashtra, India,
[4]Department of Surgical Pathology, Tata Memorial Hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Ashish Gulia,
Department of Surgical Oncology, Bone and Soft Tissue Services, Tata Memorial Hospital, Parel, Mumbai, Maharashtra, India.
E-mail: aashishgulia@gmail.com
Abstract
Introduction: Fibrous dysplasia (FD) is a benign intramedullary pathologic condition that is characterized by the replacement of bone with fibrous tissue. FD may be monostotic or polyostotic with the craniofacial bones, and the proximal femur is most commonly involved.
Case Report: A 39-year-old lady presented to our hospital, a tertiary care center with asymmetric swelling of her arms, for over 20 years. Radiographs revealed gross enlargement with marrow expansion of the right humerus, scapula with ground-glass matrix, along with a multiseptated cystic appearance. Positron emission tomography-computed tomography screening for the activity of these lesions incidentally demonstrated a few lung nodules, which on biopsy was found to be atypical adenomatous hyperplasia. The lady also had endocrine dysfunction in the form of diabetes mellitus, for which she was on treatment.
Conclusion: In this article, we briefly review the available literature to decipher if any of the associated syndromes with polyostotic FD (being the dominant clinical feature) are known to have associations which explain the above findings. There is a need to recognize the underlying pattern so that appropriate genetic counseling, if any, can be provided to such patients.
Keywords: Fibrous dysplasia, polyostotic, forequarter amputation.
Introduction
Fibrous dysplasia (FD) is a benign intramedullary pathologic condition that is characterized by the replacement of bone with fibrous tissue [1, 2]. The hallmark of the disease is a solitary focal or generalized multifocal inability of bone-forming tissue to produce mature lamellar bone and an arrest at the level of woven bone [3]. The entity was originally described by Lichtenstein [4], in 1938. FD may be monostotic or polyostotic with the craniofacial bones and the proximal femur is most commonly involved [5]. It arises mostly in the first or second decade of life as a slow-growing, painless lesion of the involved bone. Most uncomplicated cases are managed by observation since they usually run a benign clinical course and become dormant by adulthood. About 1% of cases, however, show the malignant transformation, usually osteosarcoma or chondrosarcoma and all cases must, therefore, be followed up yearly. In our case, we present a patient with polyostotic FD affecting the entire length of the right humerus, bilateral scapula, left ulna, and the left second metacarpal, along with diabetes mellitus and a few lung lesions on computed tomography, which were found to be atypical adenomatous hyperplasia on biopsy.
Case Report
A 39-year-old lady presented to our facility with a 20-year history of the right arm swelling which only progressively increased in size, to involve the entire arm, in the past 3 months (Fig. 1). There was a non-progressive swelling in the opposite distal arm as well. It was painless and there were no associated skin lesions. There was a history of open reduction and internal fixation of the right arm, following a swelling and subsequent distal humerus fracture.

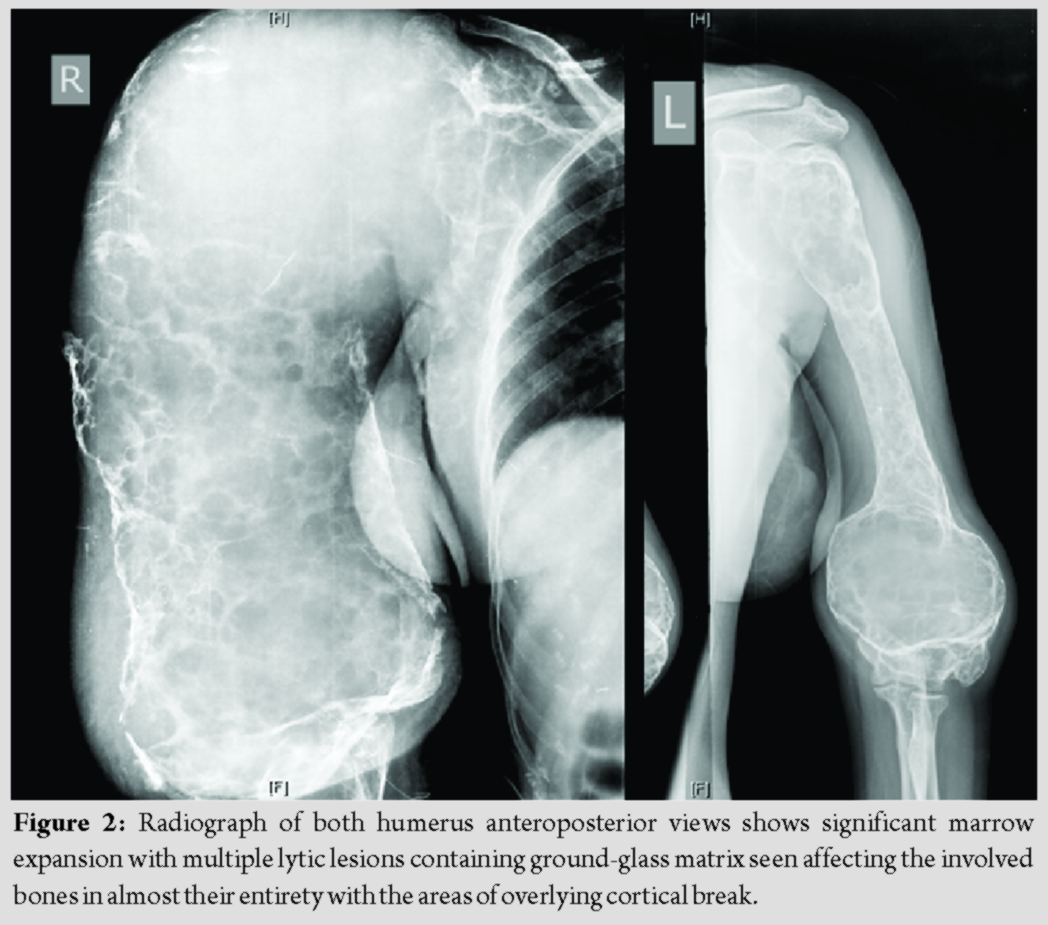
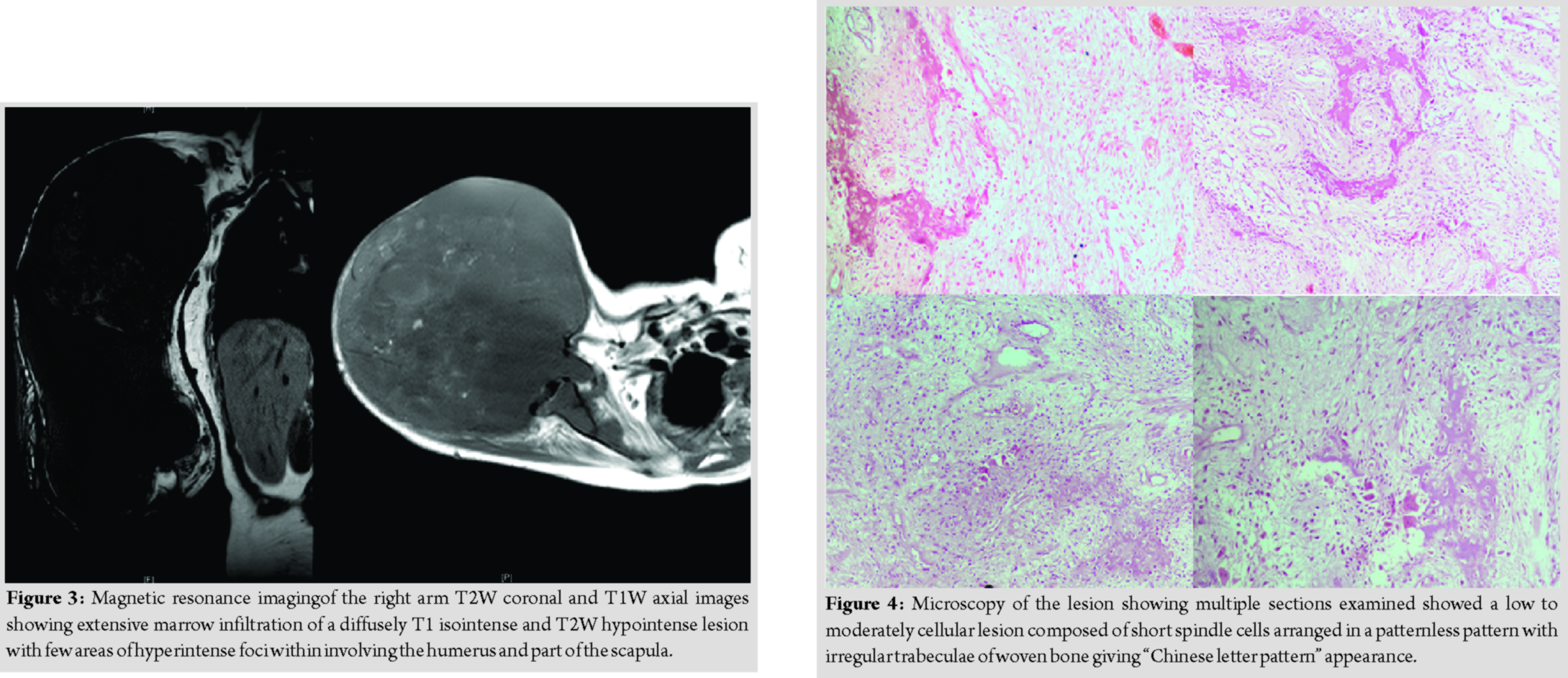
Radiological studies showed extensive lucent, ill-identified, “ground-glass” appearing lesions involving the entire right humerus (Fig. 2 and 3). There were incidental findings of similar lesions in both scapulae, right ulna, and left second metacarpal. Positron emission tomography scan showed avid lytic, expansile lesions involving the entire length of the right humerus, bilateral scapula, right ulna, and left second metacarpal. There were also lung nodules in the left upper lobe (≈8mm) and lower lobe (≈5mm) as well as in the right middle lobe (≈7mm).
Her alkaline phosphatase was 573. The parathyroid hormone was normal.
Histopathological examination of the biopsy samples from the bones showed woven bone fragments exhibiting calcification with focal cellular fibroblastic proliferation, including occasional osteoclast-like giant cells. On immunohistochemistry, the cells were negative for beta-catenin and p53, KI67 labeling was<1%. These features were concluded to be consistent with a fibrous-osseous lesion (Fig. 4).
CT-guided biopsy of the lung lesions showed features compatible with atypical adenomatous hyperplasia of the lungs with no evidence of malignancy.

After clinical, radiological, and histopathologic review at our joint clinic meeting, a diagnosis of polyostotic FD was made and the patient was worked up for a forequarter amputation (Fig. 5 and 6).

The patient, after a follow-up of 2 years, is asymptomatic for her other lesions (Fig. 7).
Discussion
Polyostotic FD accounts for 20–25% ofall FDs. Both mono- and polyostotic FDs are characterized by post-zygoticactivating mutations of signal-transducing G proteins encoded by GNAS1 on chromosome 20 [6]. Polyostotic FD has been found to have associations with McCune–Albright syndrome [7] (neuroendocrine abnormalities with Café-Au-Lait spots) and Mazabraud syndrome (FD with intramuscular myxomas) [8]. A wide range of neuroendocrine abnormalities has been described in association with McCune–Albright syndrome, such as precocious puberty, hyperthyroidism, and Cushing’s syndrome, but does not typically include diabetes mellitus. Only a few isolated case reports [9] have reported this association with diabetes. However, no known associations of polyostotic FD with atypical adenomatous hyperplasia of the lung which could be a premalignant lesion and is defined by the proliferation of atypical cuboidal or columnar epithelial cells along with the alveoli and respiratory bronchioles [10] have been reported in literature. This is the first reported patient in literature to have polyostotic FD, diabetes mellitus, and atypical adenomatous hyperplasia of lung and highlights the merit in a study that would evaluate the possibility of an underlying genetic mechanism so as to improve our understanding and management of these patients.
Conclusion
Polyostotic FD has been found to have associations with McCune–Albright syndrome, Mazabraud syndrome, etc. There is a need to recognize the underlying pattern so that appropriate genetic counseling, if any, can be provided to such patients.
Clinical Message
FD can be monostotic or polyostotic. Syndromic association of polyostotic FD can be difficult to diagnose sometimes and may present in an unusual fashion. Correct clinico-radio-pathological evaluation helps in the correct diagnosis and hence allows us to give the most appropriate management.
References
1. Canitezer G, Gunduz K, Ozden B, Kose HI. Monostotic fibrous dysplasia. Dentistry 2013;3:1667.
2. Agarwal M, Balayi N, Sumanthi MK, Sunitha JD, Geetanshu D, Neelakshi SR. Fibrous dysplasia: A review. TMU J Dent 2014;1:25-9.
3. Dorfman HD. New knowledge of fibro-osseous lesions of bone. Int J Surg Pathol 2010;18:62S-5.
4. Lichtenstein L. Polyostotic fibrous dysplasia. Arch Surg 1938;36:874-98.
5. Nayar R, Nayar AK. Fibrous dysplasia: Report of an unusual case. IOSR J Dent Med Sci 2013;8:39-41.
6. Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E, Spiegel AM. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N Engl J Med 1991;325:1688-95.
7. Albright F, Butler AM, Hempton AO. Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females-report of five cases. N Engl J Med 1937;216:727-46.
8. Resnick D. Diagnosis of Bone and Joint Disorders. 4th ed. Philadelphia, PA: Saunders; 2002. p. 4285-840.
9. Chihaoui M, Hamza N, Lamine F, Jabeur S, Yazidi M, Ftouhi B, et al. McCune-Albright syndrome associated with diabetes mellitus. Arch Pediatr 2012;19:282-4.
10. Weng S, Tsuchiya E, Satoh Y, Kitagawa T, Nakagawa K, Sugano H. Multiple atypical hyperplasia of Type II pneumocytes and bronchioloalveolar carcinoma. Histopathology 1990;16:101-3.
 |
 |
 |
 |
 |
| Dr. Mishil Parikh | Dr. Ajay Puri | Dr. Amrita Guha | Dr. Kavita Khirwal | Dr. Ashish Gulia |
| How to Cite This Article: Parikh M, Puri A, Guha A, Khirwal K, Gulia A. Case of Atypical Adenoid Hyperplasia of Lung with Polyostotic Fibrous Dysplasia and Diabetes Mellitus: A Random Coincidence or a Possible Unrecognized Syndromic Association? Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 80-83. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


