
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Proper preoperative planning and implant selection helps in getting better outcome in cases of hip arthritis with hypo plastic proximal femur.
Case Report | Volume 11 | Issue 4 | JOCR April 2021 | Page 48-51 | Neetin P Mahajan, Lalkar Laxman Gadod, Ajay S Chandanwale, Prasanna Kumar G S, Mrugank Narvekar, Ishan Gajbe. DOI: 10.13107/jocr.2021.v11.i04.2148
Authors: Neetin P Mahajan[1], Lalkar Laxman Gadod[2], Ajay S Chandanwale[3], Prasanna Kumar G S[1], Mrugank Narvekar[2], Ishan Gajbe[2]
[1]Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India,
[2]Department of Orthopaedics, Kamala Nehru Hospital, Pune, Maharashtra, India,
[3]Directorate of Medical Education and Research(DMER), Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Lalkar Laxman Gadod,
Department of Orthopaedics, Kamala Nehru Hospital, Pune, Maharashtra, India.
E-mail: lalkar73gadod@gmail.com
Abstract
Introduction: Primary total hip replacement in hypo plastic proximal femur is difficult due to the presence of a small canal, soft- tissue contracture, fragility of bone, and poor femoral cement mantle when used. Intraoperatively, there could be occurrence of fracture of the femur, inadequate fit, and fill with cement less femoral component. It is found unilaterally in cases of osteonecrosis of femoral head, post- traumatic, and in sequelae of childhood septic arthritis.
Case Report: A 45-year- old male patient presented to the OPD with complaints of pain in the left hip and difficulty in walking since for 4 years. The patient had a history of fever and swelling over the left hip in childhood with no treatment taken for the same. X-ray of pelvis with both hips showed deformed femoral head, short neck, narrow femoral canal (Grade 1 Dorr), and arthritic changes in acetabulum. We managed with total hip replacement using Wagner cone stem. Postoperatively, the patient is having good range of motion and having no difficulty in walking and weight- bearing. Functional outcome is good as per Harris hip score.
Conclusion: Total hip replacement in hypo plastic femur with arthritis is always a challenging problem. It requires surgical expertise and proper implant selection and pre-operative planning, which prevents intraoperative and post-operative complications. Wagner cone stem is a very good option in managing this type of patients.
Keywords: Unilateral hypo plastic proximal femur, childhood septic arthritis, narrow femoral canal (Grade 1 Dorr), total hip replacement, Wagner cone stem.
Introduction
Primary total hip replacement in hypoplastic proximal femur is difficult due to the presence of a small canal, soft-tissue contracture, fragility of bone, and poor femoral cement mantle when used. Intraoperatively, there could be occurrence of fracture of the femur, inadequate fit, and fill with cementless femoral component [1]. Bilateral hypoplastic hip is seen in developmental dysplasia of hip, primary osteoarthritis of hip, chronic juvenile arthritis, rheumatoid arthritis, and spondyloepiphyseal dysplasia. It is found unilaterally in cases of osteonecrosis of femoral head, post-traumatic, and in sequelae of childhood septic arthritis [1, 2]. It is also seen in patients with sickle cell anemia and achondroplasia [2]. Treatment options for osteoarthritis with proximal femoral hypoplasia include acetabular reconstruction, femoral osteotomy, total hip arthroplasty using curved stem of the 102-size Weber rotation, miniature anatomical medullary locking stem, and Wagner cone prosthesis [1, 2, 3]. Wagner cone prosthesis used in a narrow femoral canal (Dorr Grade 1) provides ease for the surgeon to correct femoral head version and also ensures the correct placement due to the presence of a 5° tapered stem and cross-section area [3]. At present, the new Wagner cone stems are available in 125° and 135° which helps in recreating appropriate biomechanical parameters such as center of rotation, offset, and limb length. Uncemented Wagner cone prosthesis prevents complications in young adult patient unlike with cemented ones which are associated with complications such as pulmonary embolism, implantation syndrome, loosening, and cardiac arrest. The rate of complications in total hip replacement done in sequelae of septic hip is higher. Complications such as acetabular fracture, greater trochanter fracture, femoral shaft fracture, and calcar fracture are commonly seen [4]. In hypoplastic femur, there are higher chances of complication such as sciatic nerve palsy (5%), intraoperative femoral fractures (10%), and recurrent hip dislocation (16%) [2]. With improved implant (uncemented Wagner cone stem) design, it is possible to reduce complications during surgeries.
Case Report
A 45-year-old male patient presented to the OPD with complaints of pain in the left hip and difficulty in walking for 4 years. The patient had a history of fever and swelling over the left hip in childhood with no treatment taken for the same. The patient had no history of tuberculosis, weight loss, anorexia, morning stiffness, other joints involvement, or any history of drug abuse. The patient was not a known case of asthma, diabetes, and hypertension. The patient had no history of chronic alcohol consumption or tobacco smoking. Local examination revealed tenderness in the Scarpa’s triangle and over the greater trochanter. The movements at the hip were restricted in all planes with the presence of 1 cm of true shortening of the limb as compared to the opposite side with adduction deformity.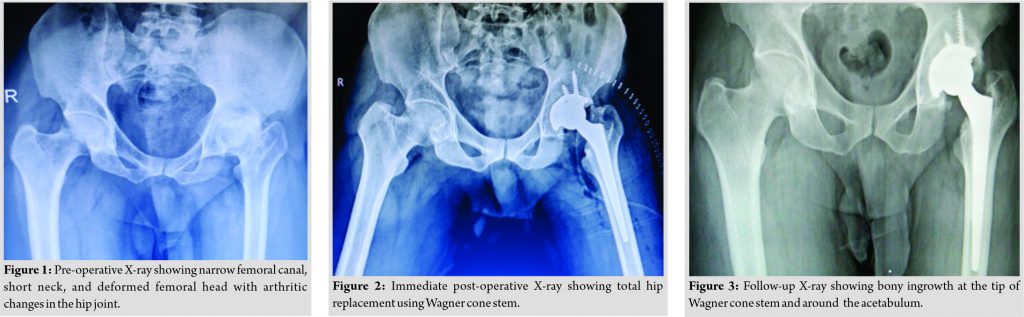
The patient was investigated radiographically with X-ray (Fig. 1) of the pelvis with both hips which was suggestive of osteoarthritis of the left hip with narrow femoral canal (Grade I Dorr), collapse of femoral head, narrow and broad neck of femur, and arthritic changes in acetabulum. The patient was initially managed with traction to cause relaxation of the contracted soft tissues. The patient was also started with physiotherapy to increase the strength in the affected muscles around the hip. As the patient’s X-ray showed hip with narrow femoral canal (champagne flute canal) (Fig. 1), templating for the hip was done and surgery was planned as total hip arthroplasty using a Wagner cone stem for the femoral component. After obtaining fitness for surgery with ESR and CRP in normal range, the patient was operated in lateral position through posterior approach. The soft-tissue dissection and the dislocation of femoral head posed difficulty due to presence of soft-tissue contracture and fibrous tissue surrounding the hip joint. After acetabulum preparation, femoral canal preparation was done using small rasps and broaches and completed with no complications. Uncemented total hip arthroplasty was done using Zimmer implant of acetabulum (Mallory head acetabulum shell 46 mm) with two self-tapping bone screws of size 6.5 mm, femoral component (uncemented Wagner cone prosthesis, 135°, size 16 with ceramic femoral head size of 28), and polyethylene liner of size 22. After implant placement, the movements at the hip joint in all planes were assessed and limb length compared for no discrepancy. Wound was closed in layers and the patient was given abduction bar to prevent dislocation postoperatively. Post-operative X-ray showed (Fig. 2) well-fixed femoral and acetabular components with proper inclination. The patient was gradually initiated with hip range of motion exercises and weight-bearing with walker started after pain relief. At present 1.5 years follow-up, the patient is comfortable with no pain and difficulty in walking. The patient has good hip range of motion. The functional outcome is good as per Harris hip score. X-ray shows bony ingrowth at the tip of femoral stem and acetabulum without loosening of implants (Fig. 3). Shorter follow-up period is the limitation of this case report.
Discussion
Unilateral hypoplastic femur is seen in osteonecrosis of femur, sequelae of septic hip arthritis, and post-traumatic arthritis of hip [1, 2]. Primary total hip replacement in hypoplastic femur is challenging due to narrow canal, soft-tissue contracture, fragility of bone, short neck, greater anteversion, and deformed head, same was observed in our case. The various treatment options for hypoplastic proximal femur include acetabular reconstruction, femoral osteotomy, total hip arthroplasty using curved stem of the 102 size Weber rotation, miniature anatomical medullary locking stem, modular prosthesis, and Wagner cone prosthesis. The use of modular prosthesis presents higher chances of failure due fracture at the modular junction [3]. Periacetabular surgery and femoral osteotomies have been recommended for patients having proximal femoral hypoplasia where the degeneration of acetabular cartilage is minimal [3]. Uncemented Wagner cone stem implant is better than other prosthesis as it reduces stress shielding effect at proximomedial aspect of femur as seen in our case. Wagner cone stem has 5° tapered stem and circular cross-section which can be put in any small femoral diameter canal and anteversion [3]. Zhen et al. [3] in their study concluded that the Wagner cone stem facilitated implantation in patients with dysplastic hip joints due to the tapered structure of the stem. The Wagner cone is suitable for patients with narrow femoral canal and gives good functional outcome. Crow et al. [5] in their study used small and straight stem and got good functional outcome. Waldstein et al. [6] had a complication during broaching, they did a femoral split from posterior aspect of femur from the tip of stem to 4–5 cm distal to femoral neck cut. In our study, as we did not have any complications while broaching as we proceed slowly while broaching. Mortazavi et al. [7] evaluated the outcome of cement less femoral reconstruction in patients with proximal femoral deformity and found that the overall mechanical failure rate was high at an average 4 years follow-up. As in our case, we used cementless Wagner cone stem due thick cortices, champagne flute canal. Yang et al. [8] in their study concluded that total hip replacement in dysplastic hip is a complex procedure requires an understanding of complex femoral and acetabular anatomy of each patient. The proper pre-operative templating, wise selection of implants, meticulous soft-tissue dissection, and surgery help in getting better outcome in patients with hypoplastic femur requiring total hip replacement.
Conclusion
Total hip replacement in hypoplastic femur with arthritis is always a challenging problem. It requires surgical expertise and proper implant selection and pre-operative planning, which prevents intraoperative and post-operative complications. Wagner cone stem is a very good option in managing this type of patients.
Clinical Message
Total hip replacement in cases of hypo plastic femur is a challenging condition as it require surgical expertise in that filed. Preoperative planning, proper implant selection helps in preventing intraoperative and post operative complications, which in turn helps in getting good outcome.
References
1. Oh KJ, Imrie S, Hwang K, Ramachandran R, Shegog M, Goodman SB. Total hip arthroplasty using the miniature anatomic medullary locking stem. Clin Orthop Relat Res 2006;447:85-91.
2. De Man FH, Haverkamp D, Van der Vis HM, Besselaar PP, Marti RK. Small stem total hip arthroplasty in hypoplasia of the femur. Clin Orthop Relat Res 2008;466:1429-37.
3. Zhen P, Liu J, Lu H, Chen H, Li X, Zhou S. Developmental hip dysplasia treated by total hip arthroplasty using a cementless Wagner cone stem in young adult patients with a small physique. BMC Musculoskelet Disord 2017;18:1-9.
4. Zhang L, Chu Y, Shao H, Bian T, Li W, Zhou Y. Cementless total hip arthroplasty for adult patients with sequelae from childhood hip infection: A medium-term follow-up study. J Arthroplast 2020;35:1885-90.
5. Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am 1979;61:15-23.
6. Waldstein W, Boettner F. A complication during femoral broaching in total hip arthroplasty: A case report. Open Orthop J 2013;7:272.
7. Mortazavi SM, Restrepo C, Kim PJ, Parvizi J, Hozack WJ Cementless femoral reconstruction in patients with proximal femoral deformity. J Arthroplasty 2011;26:354-59.
8. Yang S, Cui Q. Total hip arthroplasty in developmental dysplasia of the hip: Review of anatomy, techniques and outcomes. World J Orthoped 2012;3:42.
 |
 |
 |
 |
 |
| Dr. Neetin P Mahajan | Dr. Lalkar Laxman Gadod | Dr. Ajay S Chandanwale |
Dr. Prasanna Kumar G S |
Dr. Mrugank Narvekar |
| How to Cite This Article: Mahajan NP, Gadod LL, Chandanwale AS, Prasanna GS, Narvekar M. Primary Total Hip Replacement in a Case of Unilateral Hypo plastic Proximal Femur – A Case Report. Journal of Orthopaedic Case Reports 2021 April;11(4): 48-51 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


