
DMC is an uncommon skeletal dysplasia. There is a good prognosis for general health and survival.
Dr. Amit Kumar Yadav,
Department of Orthopaedics Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: amit_aur09@yahoo.com
Abstract
Introduction: Dyggve-Melchior-Clausen (DMC) syndrome was described in 1962 as an autosomal recessive type of spondyloepimetaphyseal dysplasia associated with mental retardation. Dymeclin (DYM) gene on chromosome 18q12.1 that encodes for DYM protein which is expressed in cartilage, bone, and brain is mutated in DMC.
Case Report: A 6 year -old male child presented with bilateral gradually progressive genu varum deformity of 4 years’ duration. There was no significant past medical and family history. A plain radiograph of his knee, pelvis, and spine shows some classical signs of skeletal dysplasia. A plain radiograph of the pelvis with both hips shows a classical semilunar, irregular lacy appearance around the iliac crest which is a pathognomonic radiological sign of this syndrome.
Conclusion: The radiographic lacy appearance of iliac crests and generalized platyspondyly with double-humped end plates are pathognomonic of DMC.
Keywords: Genu varum, Dyggve-Melchior-Clausen syndrome, spondyloepimetaphyseal dysplasia.
Dyggve-Melchior-Clausen (DMC) syndrome was described in 1962 as a rare autosomal recessive type of spondyloepimetaphyseal dysplasia associated with mental retardation [1]. Dymeclin (DYM) gene on chromosome 18q12.1 that encodes for DYM protein which is expressed in bone, cartilage, and brain is mutated in DMC [2,3]. A rare variant of DMC syndrome is Smith-McCort dysplasia which has similar bony manifestations but with the absence of mental retardation [4].
A 6 year-old male child presented with bilateral gradually progressive genu varum deformity of 4 years’ duration (Fig. 1).
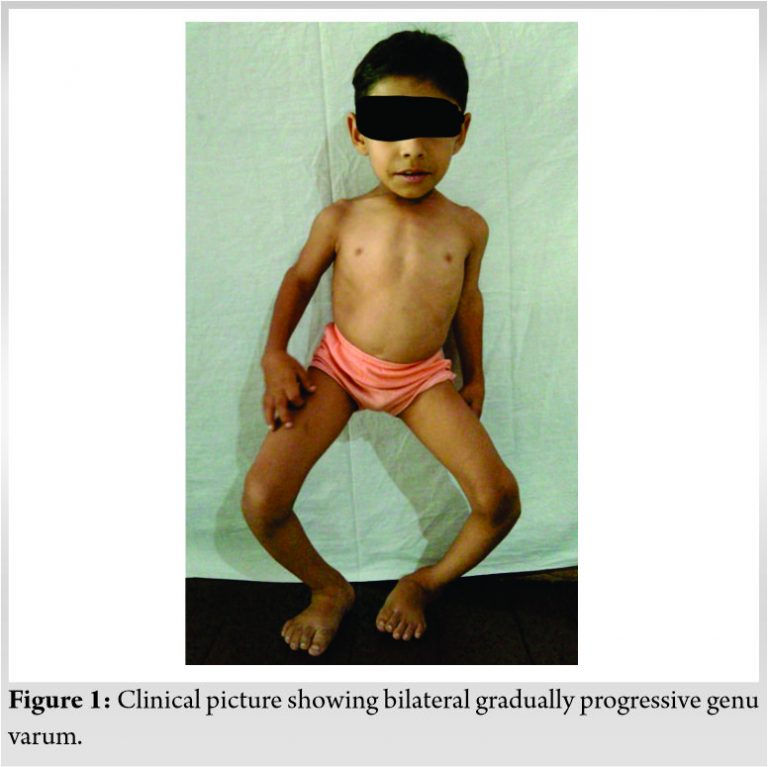
There was no significant past medical and family history which is rare for autosomal recessive inheritance. Birth history was normal term vaginal delivery with the normal physical measurement at birth. On general examination, weight was 11 kg (<3 SD), short stature (70 cm), mentally sluggish, pigeon-shaped chest, and exaggerated lumbar lordosis. Neurological examination was normal. There was no clinical sign of rickets and blood investigation for bone profile was normal. Quantitative estimation and 2D electrophoresis of glycosaminoglycan in urine were done to rule out mucopolysacridosis. A plain radiograph of his knee, pelvis, and spine shows some classical signs of skeletal dysplasia (Fig. 2). Gene testing was done to confirm a diagnosis.
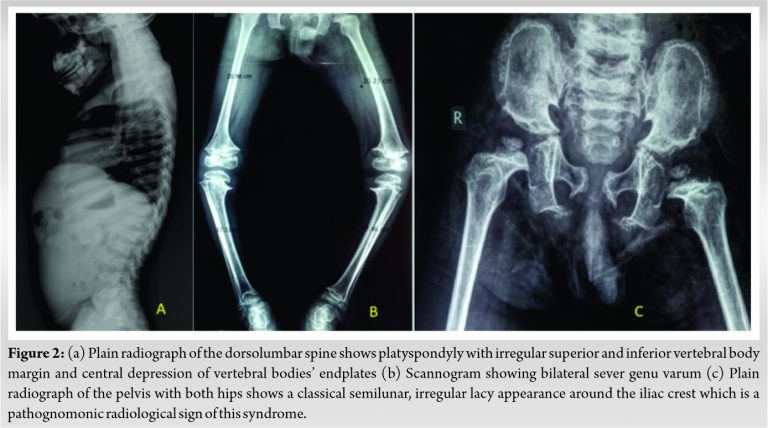
Clinical manifestations of DMC include pigeon-shaped chest, increased lumbar lordosis, broadening of the metaphysis, and brachydactyly [5]. Short neck with elevated shoulder joints, shortening of the upper extremity, and genu valgum or varum (Fig. 2b) were also present in most cases described in the literature. Rare manifestations include kyphoscoliosis, limitation of extension of joints, clinodactyly and camptodactyly of the fingers, prominent heels, flat feet or talipes equinovarus, bowing of femur, and tibia. Mild to severe mental retardation is present in all cases. The patients may also have delayed bone age, microcephaly, protruding abdomen, and generalized hirsutism. Tone, reflexes, and external genitalia are usually normal in DMC. The radiological findings include microcephaly with facial bone dysmorphism, small irregular epiphysis with often delayed ossification seen most commonly in proximal humerus and femur, and irregular metaphysis [6]. A plain radiograph of the pelvis with both hips shows a classical semilunar, irregular lacy appearance around the iliac crest which is a pathognomonic radiological sign of this syndrome (Fig. 2c) [7,8]. The lacy appearance is due to bone deposition in a wavy pattern which appears at around 3–4 years of age and persists up to adulthood. There is an asymmetric bilateral widening of the sacroiliac joint. A radiograph of the dorsolumbar spine shows platyspondyly and central depression of vertebral bodies’ endplates (Fig. 2a). These double-hump-shaped endplates with the constricted central part are also characteristic of DMC syndrome. Other features are small or short ischium, hypoplastic acetabulum, hypoplastic femoral head and neck, medial beaking of the femoral neck, delayed pubic ramus synchondrosis, wide pubic symphysis, and bilateral dislocation of hip joints, odontoid hypoplasia, and atlantoaxial instability. The radiographic lacy appearance of iliac crests and generalized platyspondyly with double-humped end plates are pathognomonic of DMC and thus act as an easy pointer to diagnosis eliminating 435 genetic skeletal dysplasia’s, directing appropriate genetic workup and counselling [9]. The closest differential diagnosis is Morquio’s disease, but absent clouding of the cornea, valvular disease, organomegaly, and the presence of typical radiology support DMC. Joint stiffness is present in DMC, unlike the hyperlaxity seen in Morquio disease. The prognosis is better in DMC related to Morquio disease. We planned the patient for guided growth with eight plates but the patient lost to follow up due to coronavirus disease 2019 [10].
DMC is an uncommon skeletal dysplasia. There is a good prognosis for general health and survival. The radiographic lacy appearance of iliac crests and generalized platyspondyly with double-humped end plates are pathognomonic of DMC.
Yadav AK, Wadia F, Gawhale S, Panchal S, Talukder P, Mokashi M. Bilateral Severe Genu Varum in Dyggve-Melchior-Clausen Syndrome – A Case Report. Journal of Orthopaedic Case Reports 2021 August;11(8): .
References
- 1.Dyggve HV, Melchior JC, Clausen J. Morquio-ullrich’s disease: An inborn error of metabolism? Arch Dis Child 1962;37:525-34. [Google Scholar | PubMed]
- 2.Thauvin-Robinet C, El Ghouzzi V, Chemaitilly W, Dagoneau N, Boute O, Viot G, et al. Homozygosity mapping of a Dyggve-Melchior-Clausen syndrome gene to chromosome 18q21.1. J Med Genet 2002;39:714-7. [Google Scholar | PubMed]
- 3.Elalaoui S, Mariam T, Ilham R, Yassamine D, Abdelaziz S. A recurrent mutation in moroccan patients with Dyggve-Melchior-Clausen syndrome: Report of a new case and review. Indian J Hum Genet 2011;17:97-9. [Google Scholar | PubMed]
- 4.Neumann LM, El Ghouzzi V, Paupe V, Weber HP, Fastnacht E, Leenen A, et al. Dyggve-Melchior-Clausen syndrome and Smith-McCort dysplasia: Clinical and molecular findings in three families supporting genetic heterogeneity in Smith-McCort dysplasia. Am J Med Genet A 2006;140:421-6. [Google Scholar | PubMed]
- 5.Aglan MS, Temtamy SA, Fateen E, Ashour AM, Eldeeb K, Hosny GA. Dyggve-Melchior-Clausen syndrome: Clinical, genetic, and radiological study of 15 Egyptian patients from nine unrelated families. J Child Orthop 2009;3:451-8. [Google Scholar | PubMed]
- 6.Beighton P. Dyggve-Melchior-Clausen syndrome. J Med Genet 1990;27:512-5. [Google Scholar | PubMed]
- 7.Nakamura K, Kurokawa T, Nagano A, Nakamura S, Taniguchi K, Hamazaki M. Dyggve-Melchior-Clausen syndrome without mental retardation (Smith-McCort dysplasia): Morphological findings in the growth plate of the iliac crest. Am J Med Genet 1997;72:11-7. [Google Scholar | PubMed]
- 8.Bayrak IK, Nural MS, Diren HB. Dyggve-Melchior-Clausen syndrome without mental retardation (Smith-McCort dysplasia). Diagn Interv Radiol 2005;11:163-5. [Google Scholar | PubMed]
- 9.Bonafe L, Cormier-Daire V, Hall C, Lachman R, Mortier G, Mundlos S, et al. Nosology and classification of genetic skeletal disorders: 2015 revision. Am J Med Genet A 2015;167:2869-92. [Google Scholar | PubMed]
- 10.Kenis V, Baindurashvili A, Melchenko E, Grill F, Al Kaissi A. Management of progressive genu varum in a patient with Dyggve-Melchior-Clausen syndrome. Ger Med Sci 2011;9:Doc25. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Enhancing Orthopedic Residents Learning: The Role of Briefing, Reverse Operative Teaching, and Debriefing
May 1, 2025 Enhancing Orthopedic Residents Learning: The Role of Briefing, Reverse Operative Teaching, and Debriefing May 23, 2018 Combined Tibial Tubercle Fracture and Patellar Tendon Avulsion: Surgical Technique and Case Report
May 23, 2018 Combined Tibial Tubercle Fracture and Patellar Tendon Avulsion: Surgical Technique and Case Report September 10, 2023 Bilateral Distal Humeral Physeal Separation-From Birth Trauma to Family Trauma
September 10, 2023 Bilateral Distal Humeral Physeal Separation-From Birth Trauma to Family Trauma December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?
December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?