
Downsloping owhto- prevents patella baja and improves outcomes in hto.
Dr. Mohammad Tauseef Khan,
Department of Orthopaedics Surgery, Rajawadi Hospital, Mumbai, Maharashtra. India. E-mail: tauseefkhan2513@gmail.com
Abstract
Introduction: Opening-wedge high tibial osteotomy (OWHTO) is a widely used procedure to improve knee function, decrease knee pain and delay arthroplasty in unicompartmental knee osteoarthritis in young patients. However, faulty technique can lead to patella baja and maltracking of extensor mechanism- leading to poor outcome. Modified biplanar downsloping OWHTO – where tibial tuberosity (TT) remains attached to proximal osteotomy fragment prevents patella baja by preventing TT to slide down during opening of osteotomy. Biplanar osteotomy also prevents rotation of distal tibial fragment. Biplanar along with downsloping osteotomy both factors combined prevents patella baja and change in quadriceps vector angle and hence patellar tracking is not altered leading to a better functional result.
Case Report: A 20 years male patient with right knee pain while walking for 2 years. Knee inspection shows varus deformity and varus thurst gait. No evidence of ligamentous laxity and meniscal injury. He was treated with modified biplanar downsloping OWHTO. Overall 12 patients were operated between 2018 and 2020 with same technique in a similar profile of patients.
Conclusion: Outcome of OWHTO can be improved and untoward complications such as patella baja which invariably occurs when TT remains attached to distal osteotomy fragment or when osteotomy passes above TT. This can be easily avoided with this downsloping OWHTO technique to give a better outcome in all 12 cases.
Keywords: Opening-wedge high tibial osteotomy, downsloping owhto, upsloping owhto, patella baja, descending owhto, ascending owhto.
High tibial osteotomy (HTO) involves shifting of weight-bearing mechanical axis from medial degenerated knee compartment to lateral uninvolved knee compartment, essentially shifting mechanical axis to Fujisawa’s point, i.e., 62% from the medial edge of medial femoral condyle toward lateral condyle [1].
HTO is often done for
- Isolated Medial compartment osteoarthritis to improve knee pain and function
- In association with chronic ligament insufficiency (acl or pcl deficient knee) where a change in slope helps to correct sagittal plane laxity [2]
- Root repairs [3]
- Meniscal transplantation
- As an adjunct is cartilage restoration and regeneration surgeries [4].
Twenty years old adult having right knee pain while walking for 2 years.
Local examination:
- Rom–full and free
- No crepitus
- No effusion
- Varus of 11 degrees
- Varus thurst gait while walking
- Mcmurray and Lachmann’s test–negative
- No ligamentous laxity.
Surgical technique
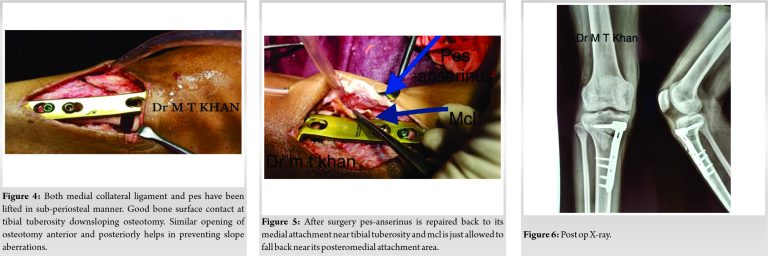
Straight vertical incision of 10 cm, starting proximally from joint line and directed downwards just medial to tibial tuberosity (TT) is taken. Such incision can be used and extended upwards, should total knee replacement be required in the future. Next complete subperiosteal dissection is carried out by lifting periosteum, pes-anserinus and distal superficial medial collateral ligament (MCL) in one sheet, (Fig. 4). Releasing distal part of superficial MCL from its posteromedial tibial attachment to just above the osteotomy site is important to decrease the intra-compartmental pressure in medial knee compartment [5,6]. If distal superficial MCL remains attached to distal tibial osteotomy fragment then medial joint intracompartmental pressure can actually increase [5] and inspite of having appropriate valgus, patient may still have severe pain and progression of knee arthritis as intra-compartmental pressure actually increases. Next, continue dissection posteriorly in sub-periosteal manner so that the whole neurovascular bundle falls posteriorly along with the soft tissue sleeve and I insert one complete surgical mop between bone and soft tissue sleave. K-wire is passed from medial tibial metaphysis about 4 cm below the joint line -directed upwards and laterally toward the proximal end of the proximal tibiofibular joint (Fig. 2).
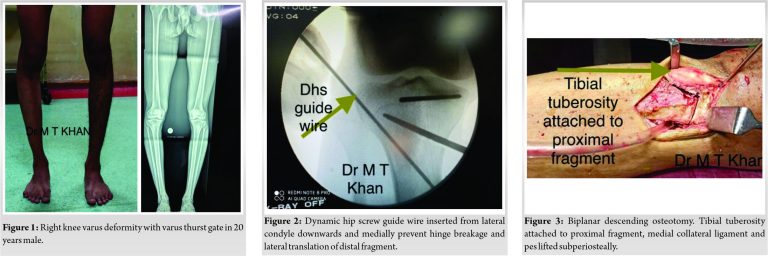
Before osteotomy is begun, two large dynamic hip screw guide wire is passed from lateral tibial condyle, starting from joint line directed downwards medially and into the medial cortex, this wire prevents osteotomy blade from making through and through cut into the lateral cortex and thereby breaking the lateral hinge and lateral translation of distal fragment (Fig. 2). Once the posterior cortex is broken then osteotomy can be opened either by stacking multiple osteotomes or using an opening device where clockwise screwing will sequentially open the osteotomy and mechanical axis deviation to Fugisawa point [1] can be manually checked using cautery wire or using alignment checking rod under c-arm guidance. Fixation is done using fixed angle medial tibial pre-contoured locking plate (Figs. 4 and 6). Bone graft is not used if medial cortex opening is <13 mm [7,8].
Conventionally open wedge medial HTO was a uniplanar osteotomy directed laterally and upwards toward proximal tibiofibular joint passing above the TT. This did help to give appropriate valgus but had following complications- (1) since osteotomy was above TT hence patella baja was common and depending upon the magnitude of patella baja, patellar tracking mechanics were altered (2). If by chance lateral hinge was broken during the opening of osteotomy then distal fragment would invariably go into rotation [9], lateral and posterior translation. Hence changes in slope [2], delayed union and non-union was common.
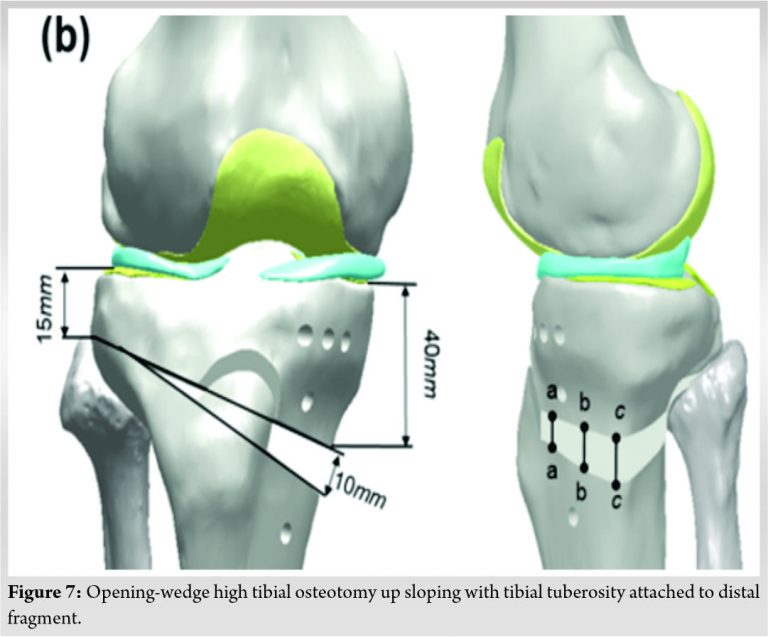
Then, came biplanar osteotomy for open wedge medial HTO but traditionally its was upsloping or ascending osteotomy (Fig. 7) where frontal or coronal plane osteotomy was directed upwards in an L shaped manner from primary osteotomy and TT remained attached to distal tibial fragment. Hence, biplanar osteotomy did solve problem’s of rotation and translation especially posterior translation of distal tibial fragment should u have hinge fracture, but it did not solve the problem of patella baja. Hence, novel new technique of downsloping or descending osteotomy in which the TT ostetomy was directed downwards in L shaped manner from primary osteotomy and hence TT continued to be attached to proximal osteotomy fragment which took care of patella baja as when u open the osteotomy the relationship of TT to the joint line does not change as it remains attached to proximal osteotomy fragment [10,11]. Essentially downsloping TT osteotomy in opening-wedge high tibial osteotomy (OWHTO) maintains patellar tracking mechanics.
Biplanar owhto with TT attached to proximal osteotomy fragment (downsloping biplanar osteotomy) effectively prevents patella baja in all cases and prevents changes in the patellar tracking mechanism. Biplanar osteotomy also helps in increased surface area for healing and prevents rotation of distal fragment as well.
Conventional biplanar upsloping (here TT remain attached to distal fragment) aka ascending OWHTO and uniplanar OWHTO osteotomy where osteotomy line passes above the TT often lead to patella baja. This can be easily prevented by this downsloping OWHTO aka descending OWHTO to improve functional outcome of OWHTO.
References
- 1.Fujisawa Y, Mashuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am 1979;10:585-608. [Google Scholar | PubMed]
- 2.Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 2004;32:376-82. [Google Scholar | PubMed]
- 3.Lee DW, Lee SH, Kim JG. Outcomes of medial meniscal posterior root repair during proximal tibial osteotomy: Is root repair beneficial? Arthroscopy 2020;36:2466-75. [Google Scholar | PubMed]
- 4.Song JS, Hong KT, Kong CG, Kim NM, Jung JY, Park HS, et al. High tibial osteotomy with human umbilical cord blood-derived mesenchymal stem cells implantation for knee cartilage regeneration. World J Stem Cells 2020;12:514-26. [Google Scholar | PubMed]
- 5.Van Egmond N, Hannink G, Janssen D, Vrancken AC, Verdonschot N, van Kampen A. Relaxation of the MCL after an open-wedge high tibial osteotomy results in decreasing contact pressures of the knee over time. Knee Surg Sports Traumatol Arthrosc 2017;25:800-7. [Google Scholar | PubMed]
- 6.Seo SS, Kim CW, Seo JH, Kim DH, Lee CR. Does superficial medial collateral ligament release in open-wedge high tibial osteotomy for varus osteoarthritic knees increase valgus laxity? Am J Sports Med 2016;44:908-15. [Google Scholar | PubMed]
- 7.Han JH, Kim HJ, Song JG, Yang JH, Bhandare NN, Fernandez AR, et al. Is bone grafting necessary in owhto? A meta-analysis of radiological outcomes. Knee Surg Relat Res 2015;27:207-20. [Google Scholar | PubMed]
- 8.Zorzi AR, da Silva HG, Muszkat C, Marques LC, Cliquet A Jr., de Miranda JB. Opening-wedge high tibial osteotomy with and without bone graft. Artif Organs 2011;35:301-7. [Google Scholar | PubMed]
- 9.Suero EM, Hawi N, Westphal R, Sabbagh Y, Citak M, Wahl FM, et al. The effect of distal tibial rotation during high tibial osteotomy on the contact pressures in the knee and ankle joints. Knee Surg Sports Traumatol Arthrosc 2017;25:299-305. [Google Scholar | PubMed]
- 10.Gooi SG, Chan CX, Tan MK, Lim AK, Satkunanantham K, Hui JH. Patella height changes post high tibial osteotomy. Indian J Orthop 2017;51:545-51. [Google Scholar | PubMed]
- 11.Krause M, Drenck TC, Korthaus A, Preiss A, Frosch KH, Akoto R. Patella height is not altered by descending medial open-wedge high tibial osteotomy (HTO) compared to ascending HTO. Knee Surg Sports Traumatol Arthrosc 2018;26:1859-66. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2022 Scapula Abscess Secondary to Shoulder Tuberculosis: Case Report with Review of Literature
June 10, 2022 Scapula Abscess Secondary to Shoulder Tuberculosis: Case Report with Review of Literature December 1, 2024 Metacarpophalangeal Joint Dislocations Two Cases, Two Stories
December 1, 2024 Metacarpophalangeal Joint Dislocations Two Cases, Two Stories April 1, 2025 Clinicoradiological Outcome of Variable Angle Volar Locking Plate in the Management of Distal Radius Fractures
April 1, 2025 Clinicoradiological Outcome of Variable Angle Volar Locking Plate in the Management of Distal Radius Fractures March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report
March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report