
Autologous bone grafting in press fit technique seems to be advantageous to treat large bone cysts to restore a biological and stable footprint for rotator cuff healing and repair.
Dr. Aurélien Traverso,
Department of Orthopaedics and Trauma Surgery, EHC Morges, Morges, Switzerland. E-mail: auremt@gmail.com
Background: About 20–25% of all rotator cuff tears are associated with footprint bone cysts. Large cysts (>10 mm2) are rare but can be problematic for anchor fixation and rotator cuff repair. So far treatment of footprint bone cysts was described using large or several anchors, cement, or compaction grafting mostly with allograft bone being biologically inferior to restore bone stock compared to autologous grafts.
Methods/Results: We report about a 57-year-old manual laborer with persistent pain and loss of shoulder function (subjective shoulder value [SSV] 50%). Magnetic resonance imaging showed a high-grade partial supraspinatus tendon tear (>50%) associated with a large supraspinatus footprint bone cyst (10 mm × 11 mm × 17 mm). An efficient setup in lateral position for arthroscopic autologous press-fit grafting from the iliac crest is described for single-stage arthroscopic rotator cuff repair. Improved fixation was achieved using a buddy anchor interference-fit technique.
Conclusion: The clinical follow-up after 12 months showed an excellent outcome (SSV >90%, DASH-Score 14 points, and Constant-Score 87 points) with dynamic ultrasound and radiographs confirming tendon and bone stock restoration.
Keywords: Footprint bone cyst, arthroscopic filling, iliac crest autologous grafting, anchor, rotator cuff repair.
Rotator cuff tears are often associated with bone cysts at the greater tuberosity [1, 2]. It is assumed that these cysts occur by direct contact of the bone with synovial fluid [3]. In most cases, these cysts are small and have no consequence for arthroscopic treatment. In the case of large bone cysts, rotator cuff repair can be compromised since suture anchor fixation depends on bone stock and bone quality [4, 5]. In the past, different arthroscopic techniques for bone grafting of cystic defects were published. Synthetic grafting was used for the augmentation of the cyst cavity [6]. Two-stage procedures with bone grafting followed by rotator cuff repair 3 months later were also described [7]. One way of a single-stage procedure is to use allograft, which is transferred into the cyst cavity by compaction grafting with a cannula system. Anchors were placed at a distance from the graft or directly into it [8]. An additional anchor was placed into the native bone for better fixation [9]. Kim et al. described arthroscopic single-stage allograft cylinder press-fit bone grafting of a large bone cyst with rotator cuff repair [10]. This is the first description of an efficient arthroscopic set-up and workflow for single-stage autologous footprint grafting for rotator cuff repair with improved fixation by combined bone press-fit and anchor interference-fit. It offers the advantage of a single-stage procedure with a fully biologic, osteogenic, and osteoinductive footprint restoration.
A 57-year-old manual laborer presented with persisting pain in his right shoulder for about 6–12 months with no improvement by continuous physiotherapy (>3 months) and subacromial injections. He also noticed a deterioration of active shoulder function, especially pain and weakness of abduction and flexion. The subjective shoulder value (SSV) was 50%, the DASH-Score 57 points, and the Constant-Score 23 points. Magnet resonance imaging (MRI) showed a high-grade partial tear (>50%) of the supraspinatus tendon associated with a large bone cyst (MRI: 10 cm × 11 cm × 17 cm) at the supraspinatus footprint (Fig. 1). The patient was positioned and draped in a lateral position with 5 kg skin traction on the arm in 45° abduction. An additional window was draped for access to the ipsilateral iliac crest (Fig. 2).
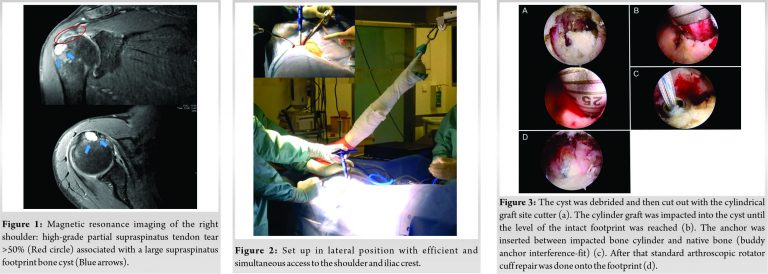
Standard glenohumeral and subacromial arthroscopy in the lateral position was performed. The bursal-sided high-grade partial thickness tear (>50%) was evaluated with a probe and completed with a diathermy device (Wand, Arthrocare). The adjacent footprint was gently probed with a chondropick which entered the cyst without much pressure. A portal at the lateral boarder of the acromion was created for perpendicular access. The cyst was visualized further and debrided with a curette and shaver. It was then measured and a depth of 17 mm and a diameter of 10 mm was recorded. The cyst was then cut out with the cylindrical graft site cutter (10 mm) to a depth of 18 mm (Fig. 3a). Simultaneously an assistant injected 20 ml Marcain with Adrenaline (1:100.000) over the marked iliac crest. A 3 cm skin incision was made over the iliac crest which was then exposed by the assistant. The iliac crest was gently deroofed with an osteotome by a thin cortical layer. Three donor sites on the iliac crest were used to harvest a single autologous bone cylinder of 22 mm height and 10 mm diameter with the Osteochondral-Autograft-Transfer-System (OATS) harvester (Arthrex). Three donor sites were used since the crest narrowed down from 12 mm width to <10 mm width after about 8 mm depth. Therefore, three cylinders of at least 10 mm width were harvested over each other for a single cylinder of 22 mm height. The cylinder graft was then impacted into the cyst until the level of the intact footprint was reached (Fig. 3b). Through the same portal, a 5.5 mm metal anchor (titanium) was inserted at the joint-sided interface between impacted bone cylinder and native bone (buddy anchor interference-fit) (Fig. 3c). Good fixation could be confirmed by strong pull on the suture ends. We then proceeded with standard arthroscopic rotator cuff repair onto the footprint (Fig. 3d). At 1 year follow-up, the patient was pain-free with no functional limitation and back to manual work. Jobe’s test was pain-free negative with strong abduction against resistance (Fig. 4). The SSV was >90%, the DASH score 23 (1 year), and the Constant-Score 87, showing a major improvement in contrast to the preoperative values.
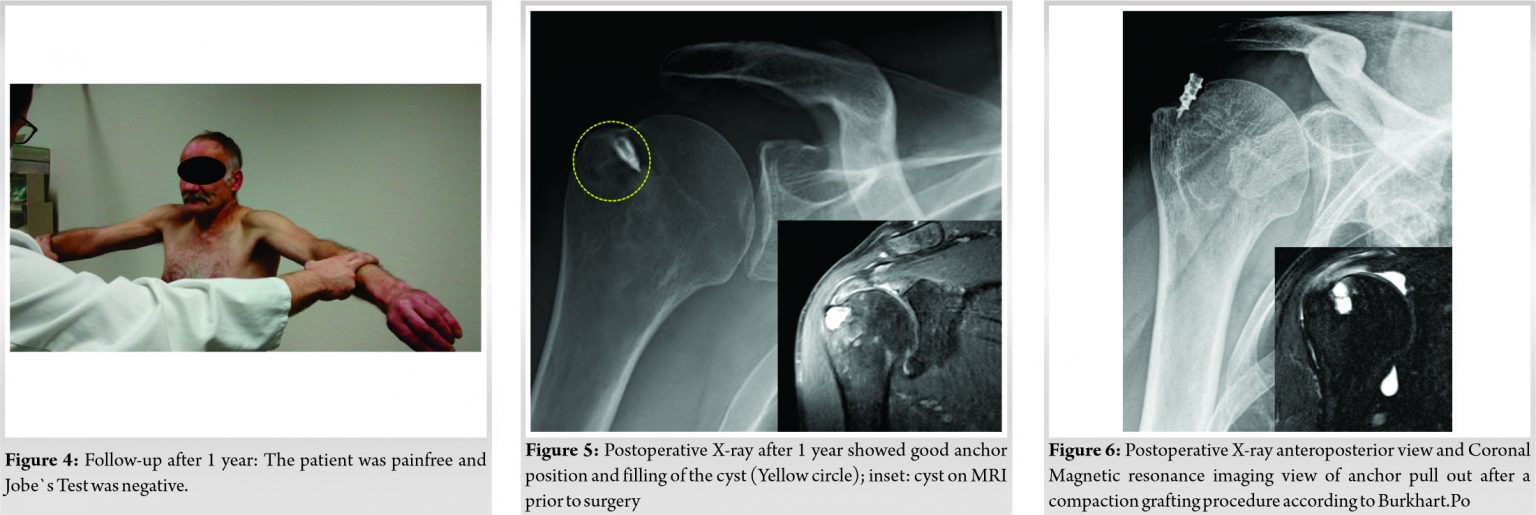
Postoperative X-rays showed good anchor position and filling of the cyst at 3 months (Fig. 5) and 1 year. Dynamic sonography of the shoulder was carried out at 1 year by a trained and certified musculoskeletal sonographer showing complete attachment of the supraspinatus tendon with comparable echo-homogeneity and thickness to the contralateral shoulder.
Large bone cysts of the proximal humerus at the rotator cuff footprint can compromise anchor fixation for rotator cuff repair. There are different arthroscopic techniques to manage bone loss and anchor fixation associated with these cysts. Synthetic grafts or fillers used in the past contain polylactic acid and polyglycolic acid with calcium sulfate [6, 8]. They degrade after a certain time [11]. Instead of synthetic grafts, allogenic cancellous compaction grafting or allogenic cylindrical grafting can be used to refill the cyst cavity [9, 10, 8]. They provide better stabilization than synthetic grafts but do not offer the advantages of autologous bone grafts with living cells and inductive factors. Burkhart and Klein used the OATS technique to refill the cyst cavity with allogenic irradiated cancellous bone chips [9]. The graft is compacted and the suture anchor placed in the center of the grafted area. In most cases, a second anchor has to be placed next to the first anchor for sufficient fixation. The end result is a cyst filled with impacted allogenic bone and often two large bone anchors, one required as a suture anchor and the second to secure fixation of the suture anchor. In such cases, the footprint surface area of the non-biologic anchor-graft complex can extend over more than 10 mm2 offering <50% of the supraspinatus footprint surface area for supraspinatus repair onto a biologic bony bed for ongrowth of the tendon. In our experience, the impaction grafting technique with chips bears a risk of anchor pull-out and failure. We previously used the exact technique with allogenic bone chips described by Burkhart and Klein [9] with one large 5.5 mm metal anchor for a large bone cyst and supraspinatus tear (Fig. 6). The construct failed 3 months after surgery due to loss of anchor fixation with pull-out of the anchor into the subacromial space (Fig. 6). This is the first article to describe an efficient set-up and technique for arthroscopic autologous iliac crest cylinder press-fit with buddy anchor interference-fit for rotator cuff repair in lateral position. The advantages are immediate press-fit stability and restoration of the bone stock with osteogenic and osteoinductive bone and provision of a larger biological surface area for tendon ongrowth. No synthetic material such as bone fillers and non-viable allogenic bone as well as less anchors are required resulting in reduction of implant cost making up for the equipment to harvest the cylinders. Finally, the lateral set-up allows for simultaneous arthroscopy and graft harvest at the iliac crest minimizing operating time.
In our case arthroscopic autologous press-fit grafting provided immediate stability of anchor fixation with the advantage of bone stock restoration with an increased bio-surface for tendon ongrowth. The cannulated cylindrical instruments are ideal for arthroscopic use and the set up in the lateral position provided efficient and simultaneous access to the shoulder and iliac crest.
Large bone cysts at the rotator cuff insertion foot-print can compromise arthroscopic repair and anchor stability and lead to failure with the need for revision due to displaced anchors. The presented autologous press-fit buddy anchor technique provides biological and mechanical advantages for successful repair.
References
- 1.Pearsall AW, Bonsell S, Heitman RJ, Helms CA, Osbahr D, Speer KP. Radiographic findings associated with symptomatic rotator cuff tears. J Shoulder Elbow Surg 2003;12:122-7. [Google Scholar]
- 2.Suluova F, Kanatli U, Ozturk BY, Esen E, Bolukbasi S. Humeral Head cysts: Association with rotator cuff tears and age. Eur J Orthop Surg Traumatol 2014;24:733-9. [Google Scholar]
- 3.Ruotolo C, Fow JE, Nottage WM. The supraspinatus footprint: An anatomic study of the supraspinatus insertion. Arthroscopy 2004;20:246-9. [Google Scholar]
- 4.Caniggia M, Maniscalco P, Pagliantini L, Bocchi L. Titanium anchors for the repair of rotator cuff tears: Preliminary report of a surgical technique. J Orthop Trauma 1995;9:312-7. [Google Scholar]
- 5.Denard PJ, Burkhart SS. Techniques for managing poor quality tissue and bone during arthroscopic rotator cuff repair. Arthroscopy 2011;27:1409-21. [Google Scholar]
- 6.Agrawal V, Stinson M. Arthroscopic grafting of greater tuberosity cyst and rotator cuff repair. Arthroscopy 2007;23:904. [Google Scholar]
- 7.Burkhart SS. Current concepts: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90. [Google Scholar]
- 8.Kim KC, Rhee KJ, Shin HD, Kim YM. Arthroscopic footprint reconstruction of a bone cyst-associated rotator cuff tear. Knee Surg Sports Traumatol Arthrosc 2007;15:1486-8 [Google Scholar]
- 9.Burkhart SS, Klein JR. Arthroscopic repair of rotator cuff tears associated with large bone cysts of the proximal humerus: Compaction bone grafting technique. Arthroscopy 2005;21:1149. [Google Scholar]
- 10.Gerber C, Schneeberger AG, Beck M, Schlegel U. Mechanical strength of repairs of the rotator cuff. J Bone Joint Surg Br 1994;76:371-80. [Google Scholar]
- 11.Athanasiou KA, Niederauer GG, Agrawal CM, Landsman AS. Applications of biodegradable lactides and glycolides in podiatry. Clin Podiatr Med Surg 1995;12:475-95. [Google Scholar]






