
Early diagnosis of atypical Monteggia is crucial to avoid delay in treatment with adherence to the principles of surgical management in Monteggia equivalent is encouraged with early elbow mobilization.
Dr. Sanjeev Singh, Department of Orthopaedics, MGM Medical College, Kamothe, Navi-Mumbai - 410 209, Maharashtra. India. E-mail: sanjeevksingh1307@gmail.com
Abstract
Introduction: Management of Mmonteggia fractures has always been debatable; Nnumerous variants have been described in the literature since its first description in 1814. We report a new variant of classical Mmonteggia fracture in a 33-year-old male.
Case Presentation: A 33-year old male was brought to the emergency room with an alleged history of assault and was managed with an external wound. Antero-Pposterior and lateral radiographs showed segmental ulna fracture and radial head dislocation. The Ppatient was managed surgically with open reduction internal fixation with reconstruction plate for segmental ulna and closed reduction of radial head was attempted after achieving an anatomical reduction of the ulna. Close attention was paid to the early post-operative mobilization of the elbow joint with the help of a Hinged elbow brace and terminal functional outcome re re-evaluated at 6six months with a DASH score of 11 and MAYO score of 92.
Conclusion: We report a rare type 1 monteggia equivalent not described in the literature. Despite the variability of the monteggia equivalents, the principle of management remains the same. Early mobilization of the elbow is of utmost importance to avoid post-operative stiffness.
Keywords: Atypical, Equivalent, Monteggia, Segmental.
A shaft of ulna fracture accompanied with the anterior dislocation of radial head was first introduced by an Italian surgeon, Giovanni Battista Monteggia in 1814 [1]. This injury pattern was later termed Monteggia fracture-dislocation by Perrin in 1909 [2]. In 1967 Bado Classified Monteggia fracture-dislocation into four main groups [3]. Posterior interosseous nerve (PIN) palsy is a recognized complication of Monteggia fracture-dislocation with the incidence ranging from 3.1% to 31.4% [4]. The low incidence of Monteggia fracture reflects limited familiarity with their diagnosis among the emergency physicians leading to higher chances of missed diagnosis. Sound clinical evaluation and carefully assessed radiographs particularly lateral views are a must. Unnoticed radial head dislocations may remain asymptomatic for several weeks and months leading to fibrosis in the ulna notch further encumbering radial head reduction. Restricted range of motion is appreciated chiefly during flexion. The treatment in the operative room is an anatomical reduction of ulna which is usually sufficient to reduce the radial head and usually stable during pronation and supination. Radial head dislocation usually causes a tear in the annular ligament which may remain intact and connected to the lateral collateral ligament and ulna. Ulna fracture can be managed with a DCP or TENS, surgeons prefer plate over nail because anatomical reduction is a must for radial head stability.
A 33-year old male presented to the emergency unit 4 h after an injury with an alleged history of assault. Following the injury he developed severe pain, swelling in the left forearm, and restricted movement at the left elbow. The forearm was observed to be kept in a semi pronated position and in extension with an external wound measuring about 2 × 1.5 cm over the dorsum of the forearm at the proximal one-third shaft of the ulna with no signs of PIN palsy. Palpatory findings confirmed crepitations and local tenderness along the ulna with no signs of compartment syndrome, Antero-posterior, and lateral radiographs showed segmental ulna shaft fracture with anterior dislocation of the radial head (Fig. 1).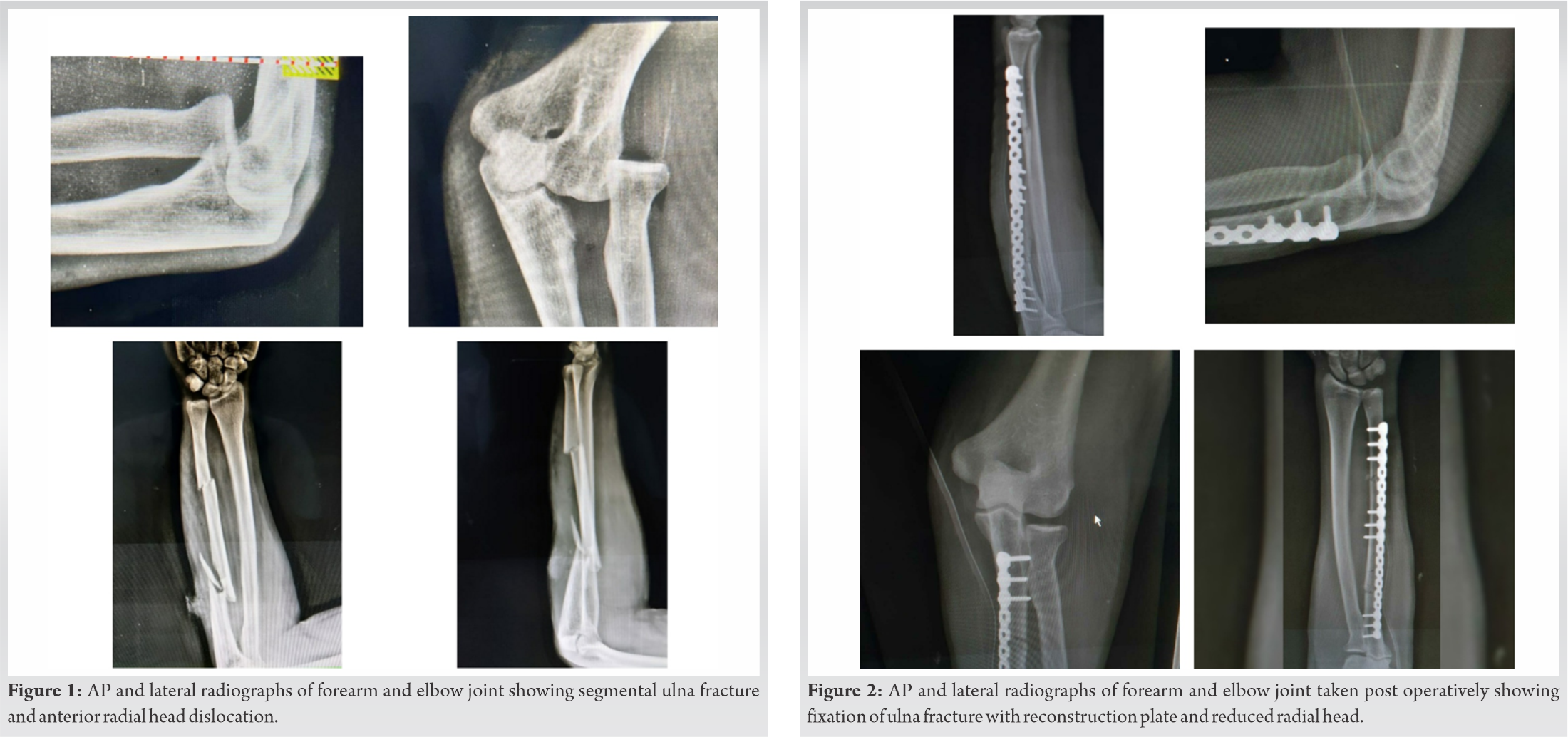
The patient was taken for surgery after an anesthetic workup. The patient was taken on the table in the lateral position and a tourniquet was applied, after appropriate anesthesia ulna was approached with the dorsal approach through the interval between the Extensor Carpi Ulnaris and Flexor Carpi Ulnaris. After Aligning the fragments with bone holding forceps, fracture stabilized and fixed with 14 Holed Reconstruction plate (3.5 nonlocking plate) (Fig. 2), radial head was observed to be reduced after anatomical reduction of segmental ulna, reduction checked under a fluoroscope and found to be stable. Above elbow plaster back slab was applied.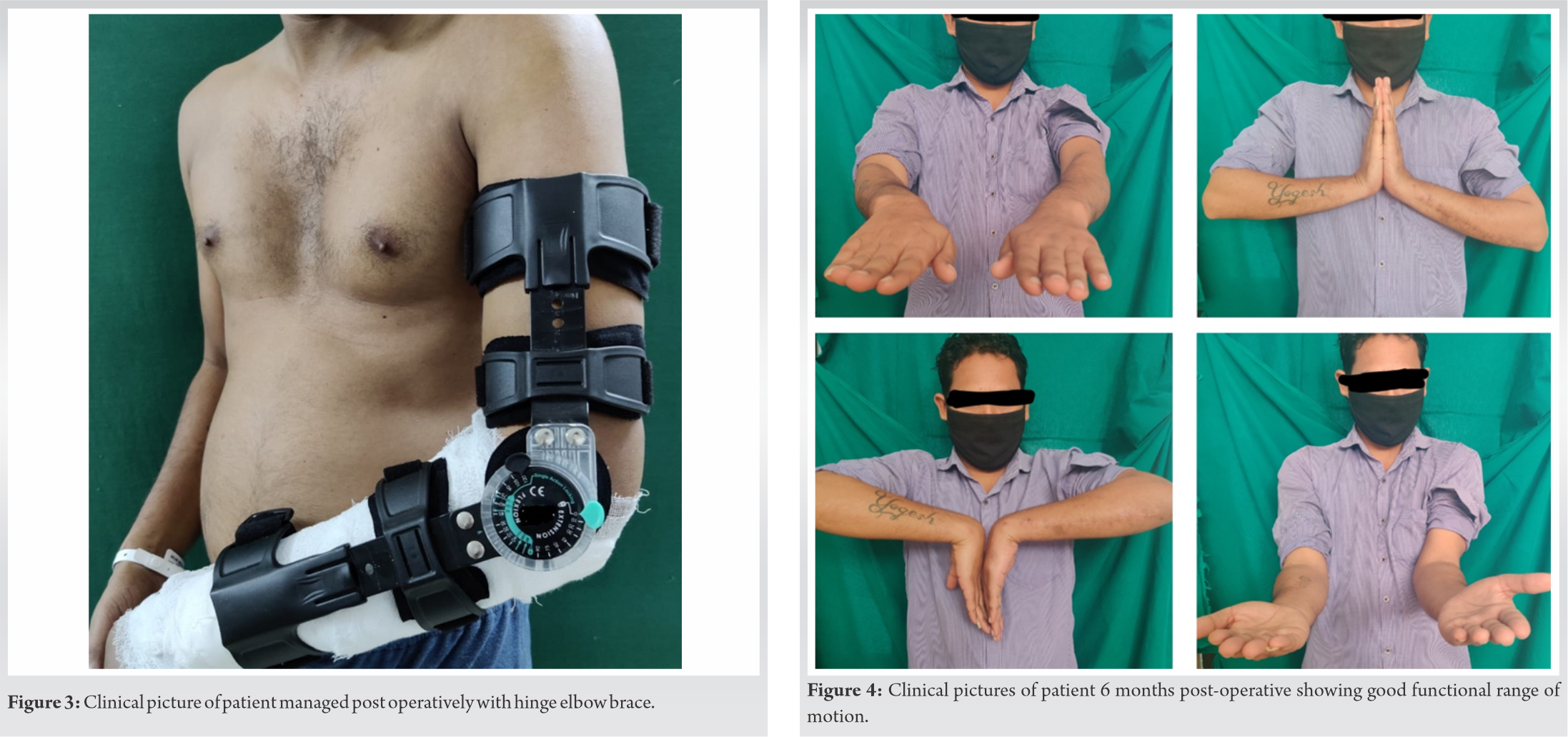 Post-operative radiographs showed an acceptable reduction of the ulna. Radio–Capitellar joint was reduced and congruent. Active assisted range of motion (flexion and extension) were initiated from Day 2 of the postoperative period with the help of a Hinged elbow brace (Fig. 3).
Post-operative radiographs showed an acceptable reduction of the ulna. Radio–Capitellar joint was reduced and congruent. Active assisted range of motion (flexion and extension) were initiated from Day 2 of the postoperative period with the help of a Hinged elbow brace (Fig. 3).
Regular follow-up at 2 weeks and 6 weekly radiographs showed gradual healing of the fracture with the union at two and half months. At 6 months follow-up appreciable DASH score of 11 and an excellent MAYO 92 score with a good functional range of motion at the wrist and elbow were achieved (Fig. 4).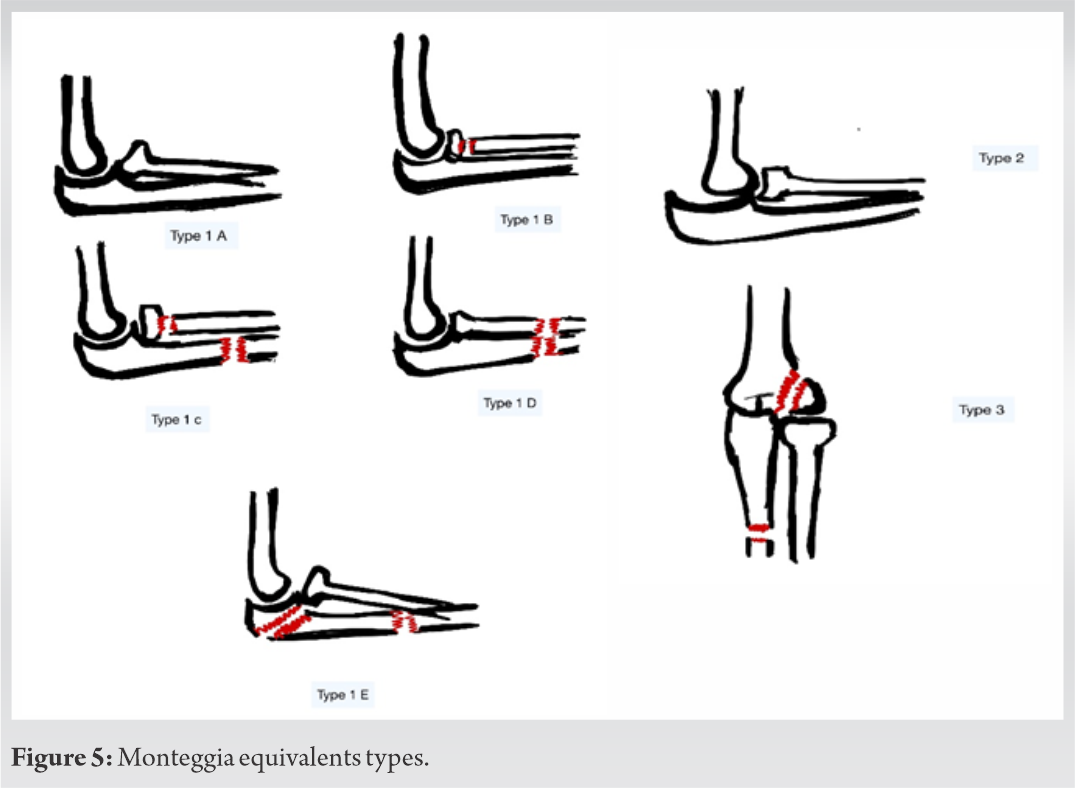
Monteggia fracture-dislocation is a rare entity among adults and children comprising <5% of all forearm fractures. Diagnosis of Monteggia injuries is often missed in the emergency units wherein due to the pain and swelling immediately after the trauma, conventional anteroposterior and lateral radiographs are difficult due to pain. Thorough clinical and radiographic interpretations play a vital role in the early diagnosis of Monteggia injuries. The treatment in the operative room after the injury is simple: anatomical reduction of the ulna is usually sufficient to reduce the radial head and produce excellent outcomes [5]. According to Bado, “fresh” Monteggia Type I and equivalent lesions should be treated by closed reduction with a supination maneuver [6]. In current practice, Open reduction with internal fixation of the ulna fracture and closed reduction of the radial head is currently the accepted treatment of choice of acute Monteggia fracture-dislocations in adults [7,8,9]. In literature, authors have attributed Monteggia fractures to extension and pronation or hyper pronation of the forearm, or direct posterior blow to raised ulna shaft as seen in nightstick fractures [10]. Radial head irreducibility is often attributed to the annular ligament which even on remaining intact or partially torn may hinder its reducibility [3]. Other causes include biceps tendon interposition or of the posterior interosseous nerve [11]. Bado and other authors proposed injuries equivalent to Monteggia fracture-dislocation commonly known as Monteggia Variants used for Monteggia type 1 and 2, no equivalents have been found for type 3 and 4.
Type 1 Monteggia Variant [5]: includes anterior dislocation of radial head commonly seen in children (pulled elbow); fracture of the ulna shaft with fracture of the proximal third or neck of the radius; fracture of the ulna diaphysis or olecranon with anterior dislocation of the radial head; Posterior dislocation of the elbow, fracture of the ulna shaft with or without proximal radius fracture; fracture of the proximal radius. With the alleged history of assault, it can be predicted that a direct blow to the ulna shaft causing fracture of the ulna at two distinct zones wherein the proximal fragment translated the force causing anterior dislocation of the radial head as seen in this case, various factors like the direction of radial head dislocation, the direction of angulation of ulnar fracture and the fracture pattern can be used to retrogradely predict the fracture mechanism as has been previously described in the literature [12]. Thus depending on the direction of radial head dislocation, fracture pattern of the ulna wherein instead of olecranon fracture a more distal fracture line as observed, our case can be related to the Monteggia variant type 1.
Segmental ulna shaft fractures can be managed with different modalities including closed manipulation and intramedullary titanium elastic nailing/ Rush nailing or traditionally with open reduction and internal fixation with non-locking-plate after achieving satisfactory radio-capitellar joint stability. However, intramedullary nailing with Titanium elastic nailing system of ulna shaft demands for immobilization at the elbow joint for four to 6 weeks.
Monteggia equivalent injuries are commonly observed in pediatric age group.
Lokesh et al. in 2018 [13], described a similar pattern of fracture-dislocation in a 47-year-old, however, due to concerns with the instability of the radial head, opted to hold the radial head temporarily with K-wires, fixed the ulna fracture with a flexible nail, and prevented elbow range of motion for 5 weeks and got the suboptimal outcome. Givon et al. in 1997 [14] reviewed retrospectively 34 cases with Monteggia type 1 equivalent injury using motion score for elbow joint and observed better results in children compared to adults. Makram Zrig et al. in 2011 reported an usual case of monteggia equivalent in a 6-year-old female with fracture of ulna diaphysis and fracture of neck of radius without radial head dislocation managed with manual traction and casting, observed full flexion and extension and near-normal pronation and supination at 10 months follow-up [15]. Traditionally, plating of the forearm fracture has shown to give excellent results and allows early mobilization [16]. In a present report with acceptable reduction of the ulna and radio-capitellar joint using reconstruction plate and closed manipulation respectively along with early mobilization using Hinged elbow brace and regular follow up with X-ray at 2 weeks were performed to ensure radial head position, the patient showed excellent mayo and DASH score. The MAYO score was observed to be 92 with a near-normal range of motion at the elbow and wrist joint. Even in the rare variants, surgical principles of treatment of Monteggia fractures remain the same, where reduction and stabilization of the ulna fracture should be sufficient to maintain radial stability with favorable outcomes [17].
Monteggia equivalent type 1 variant includes anterior radial head dislocation along with olecranon fracture and diaphyseal ulna fracture, our case closely resembles this variant. As far as the knowledge and research of the authors is concerned, segmental comminuted ulna fracture with radial head dislocation has not been described in any variant or literature and only one similar case has been reported. Thorough operative planning is mandatory as it shall affect the functional outcome of the wrist and elbow joint.
We report a new type 1 monteggia equivalent not described in the literature. Despite the variability of the monteggia equivalents, the principle of management remains the same. Early mobilization of the elbow is of utmost importance to avoid post-operative stiffness.
Early diagnosis of atypical Monteggia is crucial to avoid delay in treatment. Adherence to the principles of surgical management in Monteggia equivalent is encouraged and early elbow mobilization.
References
- 1.Rehim SA, Maynard MA, Sebastin SJ, Chung KC. Monteggia fracture-dislocations: A historical review. J Hand Surg Am 2014;39:1384-94. [Google Scholar | PubMed]
- 2.Agarwal A, Pawar I. Neglected Type I monteggia fracture dislocation in adult. J Clin Diagn Res 2017;11:RD01-2. [Google Scholar | PubMed]
- 3.Delpont M, Louahem D, Cottalorda J. Monteggia injuries. Orthop Traumatol Surg Res 2018;104:S113-20. [Google Scholar | PubMed]
- 4.Li H, Cai QX, Shen PQ, Chen T, Zhang ZM, Zhao L. Posterior interosseous nerve entrapment after monteggia fracture-dislocation in children. Chin J Traumatol 2013;16:131-5. [Google Scholar | PubMed]
- 5.Letts M, Locht R, Wiens J. Monteggia fracture-dislocations in children. J Bone Joint Surg Br 1985;67:724-7. [Google Scholar | PubMed]
- 6.Bado JL. The monteggia lesion. Clin Orthop Relat Res 1967;50:71-86. [Google Scholar | PubMed]
- 7.Eathiraju S, Mudgal CS, Jupiter JB. Monteggia fracture-dislocations. Hand Clin 2007;23:165-77. [Google Scholar | PubMed]
- 8.Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-24. [Google Scholar | PubMed]
- 9.Ring D. Monteggia fractures. Orthop Clin North Am 2013;44:59-66. [Google Scholar | PubMed]
- 10.Ravish VN, Raju B, Hadi SA, Bharadwaj V. An atypical type of monteggia equivalent: A case report. Int J Case Rep Orthop 2020;2:18-20. [Google Scholar | PubMed]
- 11.Armstrong RD, McLaren AC. Biceps tendon blocks reduction of the isolated radial head dislocation. Orthop Rev 1987;16:104-8. [Google Scholar | PubMed]
- 12.Bhandari N, Jindal P. Monteggia lesion in a child: Variant of a Bado Type-IV lesion. A case report. J Bone Joint Surg Am 1996;78:1252-5. [Google Scholar | PubMed]
- 13.Gupta L, Rathore LP. An atypical type of monteggia equivalent: A case report. Int J Orthop Sci 2018;4:1037-9. [Google Scholar | PubMed]
- 14.Givon U, Pritsch M, Levy O, Yosepovich A, Amit Y, Horoszowski H. Monteggia and equivalent lesions. A study of 41 cases. Clin Orthop Relat Res 1997;337:208-15. [Google Scholar | PubMed]
- 15.Zrig M, Mnif H, Koubaa M, Bannour S, Amara K, Abid A. An unusual monteggia Type I equivalent fracture: A case report. Arch Orthop Trauma Surg 2011;131:973-5. [Google Scholar | PubMed]
- 16.Stern PJ, Drury WJ. Complications of plate fixation forearm fractures.Clin Orthop Relat Res 1983;175:25-9. [Google Scholar | PubMed]
- 17.ElKhouly A, Fairhurst J, Aarvold A. The MonteggiaFracture: Literature review and report of a new variant. J Orthop Case Rep 2018;8:78-81. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2022 An Uncommon Finding of Posterior Cruciate Ligament Intrasubstance Cyst: A Case Report and Review of Literature
March 10, 2022 An Uncommon Finding of Posterior Cruciate Ligament Intrasubstance Cyst: A Case Report and Review of Literature August 1, 2025 Chronic Syndesmotic Instability Associated with a Complex Lesion of the Posterior Inferior Tibiofibular Ligament: Review, Case Report, and Surgical Report
August 1, 2025 Chronic Syndesmotic Instability Associated with a Complex Lesion of the Posterior Inferior Tibiofibular Ligament: Review, Case Report, and Surgical Report April 1, 2026 Reviewers Acknowledgement & Photo Gallery April 2026
April 1, 2026 Reviewers Acknowledgement & Photo Gallery April 2026 October 1, 2024 Bicondylar Tibial Plateau Fracture in Below-Knee Amputation: A Rare Injury Case Report
October 1, 2024 Bicondylar Tibial Plateau Fracture in Below-Knee Amputation: A Rare Injury Case Report