
Reconstruction of the intercalary bone defects with bone cement - plate hybrid construct in cases of distant solitary metastasis of diaphyseal bone remains a viable option in patients with shorter life expectancy or cost constraints.
Dr. Tarun Goyal, Department of Orthopaedics, All India Insti-tute of Medical Sciences, Bathinda, Punjab, India. E-mail: goyal.tarun@gmail.com
Introduction: Late metastasis and recurrences after 10 years of curative treatment is a known biological behavior of renal cell carcinoma (RCC) and a long follow-up is required for the detection of metastasis. Late solitary bony metastasis is very rare. No case of a late solitary metastasis of distal femur, treated with wide local excision and reconstruction, is available in the literature. We present a case of solitary metastatic lesion of distal femur 12 years after radical nephrectomy for renal cell carcinoma in a 64-year-old male.
Case Report:The patient presented to us with swelling in the right distal thigh for three years with a history of radical nephrectomy for RCC 12-years back. The lesion was not re-sponding to local radiotherapy, and chemotherapy in the form of oral pazopanib, taken before orthopedic consultation. After core biopsy, the tumor was managed by intercalary wide local excision and reconstruction using a cement block and a lateral locking plate. Post-operatively, the histopathology report confirmed the diagnosis to be a clear cell tumor, consistent with metastatic RCC. The patient is independently mobile and tumor-free 2 years after the surgery.
Conclusion:Wide resection and reconstruction of the skeletal defect remains the mainstay of the management of metastatic solitary lesion. We have presented a unique case of distal fem-oral solitary metastatic deposit from a primary RCC 12 years post radical nephrectomy treat-ed by intercalary resection and reconstruction with bone cement-plate hybrid construct.
Keywords: Renal cell carcinoma, metastasis, femur, wide local excision, intercalary resection.
Renal cell carcinoma (RCC) is the most common malignancy of kidneys in adults and ac-counts for 2-3% of all cancers worldwide [1]. Almost one-third of the patients present with metastatic disease and another 20-30% develop recurrence or metastasis after nephrectomy [2]. Majority of metastasis present in the first few years after the treatment of RCC. Late me-tastasis and recurrences after ten years of curative treatment, though rare, is a known biologi-cal behavior of RCC. It may be seen in up to 11% of these patients [3]. A long-term follow-up is required in these patients for surveillance of these metastases. The majority of these late metastases are solitary, and surgical excision carries a good prognosis. The most common site of these delayed metastases is the lung followed by the kidneys. Late metastasis to the central nervous system and gastrointestinal system has also been reported [4, 5]. Late metastasis to the musculoskeletal system is rarely reported in the literature. Here, we report a unique case of a 64-years-old male, presenting 12 years after a right radical nephrectomy for primary RCC with a solitary metastatic lesion in the right distal third of femoral diaphysis. This is a very rare skeletal site of metastasis and has not been reported be-fore. A unique technique of reconstruction using intercalary resection and knee joint preservation with a cement block augmented with a plate and screw construct was carried out.
A 64-year-old male presented to us with the complaint of swelling in the right distal thigh for the last three years. It was gradually increasing in size with occasional dull aching pain. He had a right-sided radical nephrectomy for RCC 12-years back. On examination, the swelling was in the anteromedial aspect of right distal thigh, firm to bony hard in consistency, globu-lar, immobile and deep to the muscle plane. It measured 7 × 10 cm and the range of motion of the knee joint was unaffected. 
The pre-operative radiograph showed an eccentric lytic lesion in the distal femur with moth-eaten appearance and involvement of surrounding soft tissue (Fig. 1). Magnetic resonance imaging revealed a well-circumscribed mass in the distal femur, 11 × 4 × 5 cm in dimensions, iso-intense on T1 weighted image and hyper-intense on T2 weighted image. It was located 25 cm from the tip of the greater trochanter and 5 cm proximal to articular surface laterally and 3 cm medially (Fig. 2).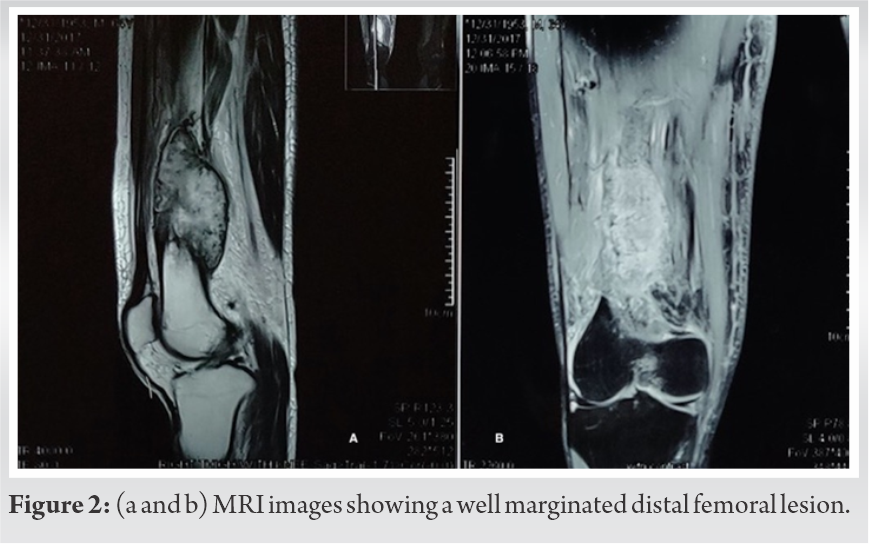 PET scan showed no other lesions in the body (Fig. 3). There was no vascular encasement by the tumor on CT angiogram.
PET scan showed no other lesions in the body (Fig. 3). There was no vascular encasement by the tumor on CT angiogram. 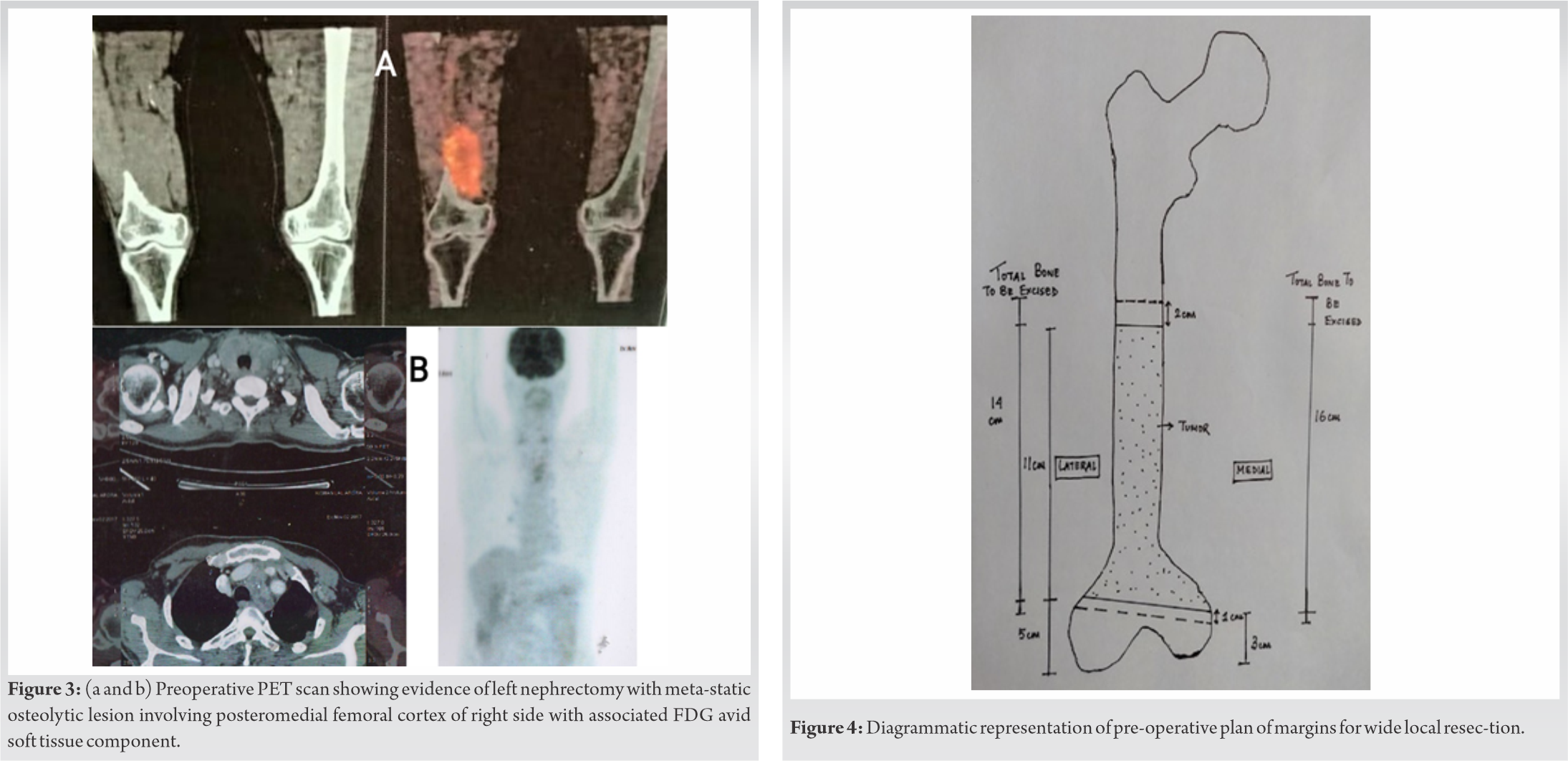
Core biopsy confirmed the diagnosis of metastatic clear cell RCC. He had received local ra-diotherapy 1-year back and was started on oral Pazopanib before orthopedic consultation was sought, but the tumor showed no regression in its size. Pre-operative planning for resection of the tumor with the reconstruction of the intercalary defect with bone cement was done and exact margins of resection were decided (Fig. 4). Exposure was achieved by anterior midline approach and a plane was developed between the tumor and the vastus intermedius muscle. Wide local excision of the tumor with its intact capsule, along with the cuff of surrounding vastus intermedius muscle was carried out (Fig. 5). There was no breach of the tumor capsule during excision. The intercalary defect of 16 cms was filled up with Simplex P bone cement (Stryker, USA) after keeping two intra-medullary 4.5 mm Steinmann pin medially. Laterally, it was supported by a 13-hole titanium locking plate before cement was set. Post-operative plain radiograph was done (Fig. 1). The excised segment of bone including the muscle cover measured about 16.5 × 7 × 5 cm. Intra-operative frozen section samples from bony and soft tissue margins were clear of any tumor cells.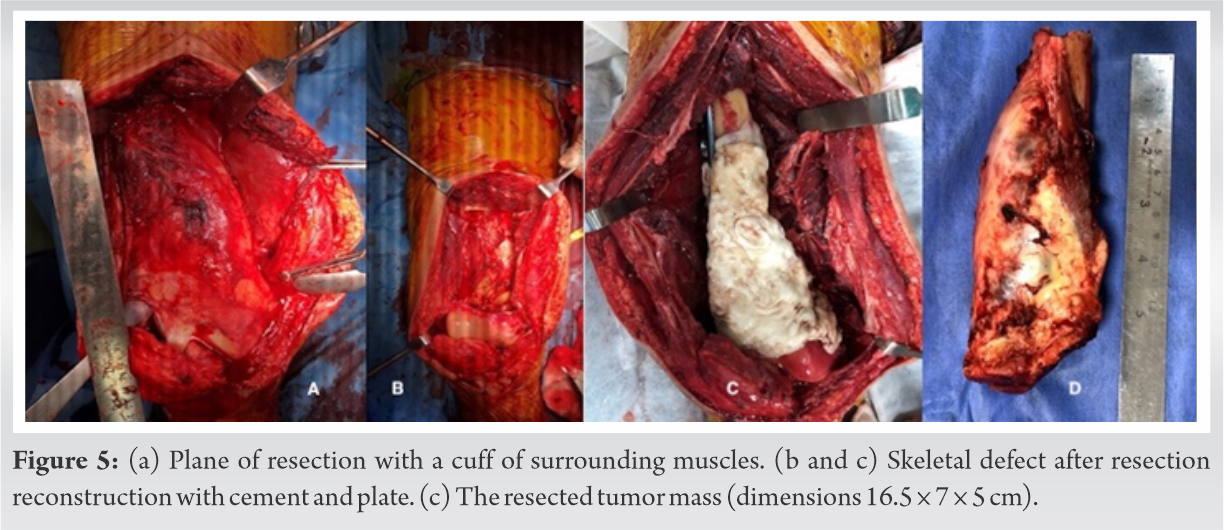
Post-operatively, the histopathology report confirmed the diagnosis to be metastatic clear cell tumor of the right distal femur, consistent with metastatic RCC (Fig. 6). The patient was al-lowed weight-bearing as tolerated from the first post-operative day and knee range of motion exercises were started within limits of pain. At 2 years follow-up the patient walks without support, with knee flexion up to 120 degrees without any complaints or complications (Fig. 7).
The patient was al-lowed weight-bearing as tolerated from the first post-operative day and knee range of motion exercises were started within limits of pain. At 2 years follow-up the patient walks without support, with knee flexion up to 120 degrees without any complaints or complications (Fig. 7). 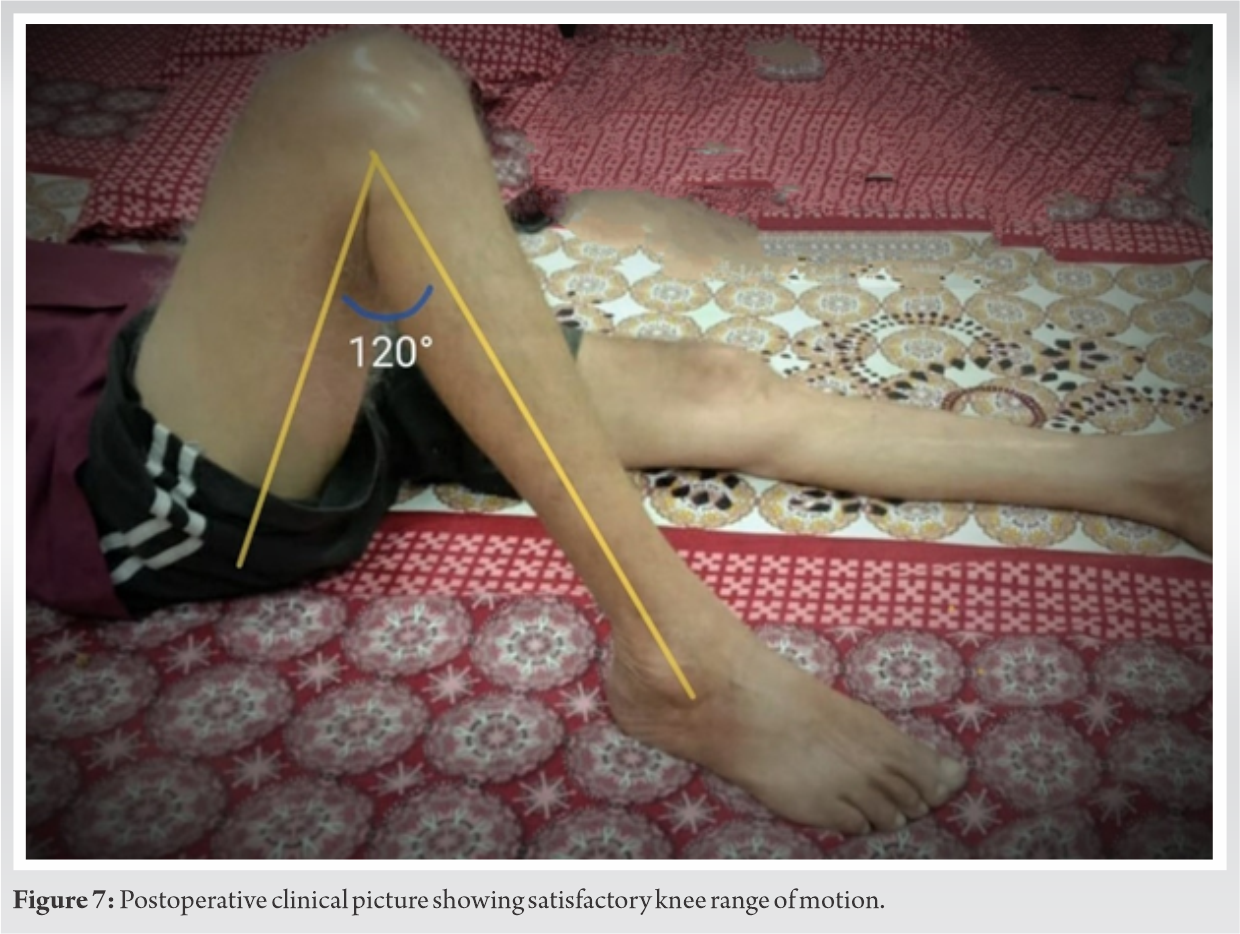 A follow-up PET scan did not show any active lesion in the body (Fig. 8).
A follow-up PET scan did not show any active lesion in the body (Fig. 8).
These late metastases present a unique diagnostic dilemma, and a primary bone tumor or me-tastasis from any other site, has to be ruled out at this age. This includes a planned biopsy from the lesion. Our patient was treated with intercalary excision, because it was located away from the knee joint and thus, salvage of the native knee joint was possible. Reconstruction options with salvage of knee joint included bone transport, allograft reconstruction, bone grafting, or custom-made metallic spacer. Primary cement spacers for intercalary reconstruction have been described by Puri et al. [6]. This proved early mobility to the patient which was crucial in a patient of this age. The rehabilitation period was very short as this patient was allowed weight bearing within limits of pain within 24 h after the surgery and has been walking independently since then. The cost of the treatment is also lesser than the other mentioned treatments. Allografts will carry a risk of resorption, infection or fracture. Bone transport takes a longer period of time and may have failed considering that this patient was elderly, was on immunotherapy, and had received chemotherapy and local radiotherapy in the past. These spacers can be easily revised to a vascularized fibular graft or a custom-made in-tercalary prosthesis in the future if needed. RCC responds poorly to radiotherapy, chemotherapy, and immunotherapy. These modalities have been used in the treatment of metastatic RCC but the response rate is poor making sur-gical excision treatment of choice wherever possible [7]. Surgical excision of a solitary me-tastasis in RCC may provide five-year survival rates of 35-60% [7]. Factors improving sur-vival after excision of bone metastasis are a solitary metastatic disease, younger age at presentation, tumor-free resection margins, absence of a pathological fracture, histology grade, and longer time from nephrectomy to bone metastases [8]. Fuchs et al. [7] studied 60 patients with solitary metastatic RCC of which 13 patients were managed by wide local re-section, 20 by intralesional resection and local stabilization and 27 patients received no surgical treatment. The 1-, 3-, and 5-year survival rates were 83%, 45%, and 23%, respectively. Patients treated with intralesional resection and intramedullary stabilization had a higher incidence of local disease progression. Hence, the wide local resection remains the choice of surgical management for disease control. Pazopanib is an oral angiogenesis inhibitor acting on vascular endothelial growth factor receptor, platelet-derived growth factor receptor and tyrosine kinase receptor. It has shown to improve progression-free survival [9]. However, our case did not show any good clinical response with pazopanib in terms of containment and regression of the lesion. Bony metastasis is relatively common in primary metastatic RCC and may be seen in 35% of these patients [10]. Swanson et al. studied 947 patients with RCC, and found skeletal metastasis in 26.7 % of patients, mostly involving spine, pelvis and proximal femur [10]. It is generally associated with widespread metastasis and isolated skeletal metastasis is uncommon [9]. It is also very rarely seen as an isolated late metastasis. Miyao et al. [3] studied the pattern of delayed metastasis in 470 patients who had undergone curative treatment of RCC. In this series, 30 patients (6.4%) developed a late metastasis. Only six sites of bony involvement were found of which only one was treated surgically. A case of metastatic lesion of tibia and ankle from primary RCC 1-year post nephrectomy managed surgically by above-knee ampu-tation has been described before [11]. Late metastasis of an RCC in soft tissues of the thigh has also been reported [12]. Rare cases of skeletal muscle metastasis from RCC have also been reported [13, 14, 15, 16].
After a thorough literature search, distal femoral solitary metastatic deposit from primary RCC 12 years post radical nephrectomy remains a rare entity to the best of our knowledge. Thus, the uniqueness of our case lies in firstly the site being distal femur around 4.9 cm above the articular surface, secondly, the time of presentation which is 12 years post nephrectomy for primary RCC. Moreover, the technique employed for the surgical management of the tumor by resection and reconstruction of the intercalary defect with cement block is also quite uncommon. Although there were no signs of loosening of the cement spacer in this case, one should be careful to look for radiolucency around the cement bone junction and pain while following up these cases. The choice of this reconstruction technique is justified by the benefit of immediate stability, early mobilization and cost-effectiveness. Moreover, looking at the poor prognosis and life expectancy of metastatic RCC this reconstruction technique may be a viable option. The post-operative histopathological diagnosis was metastatic clear cell variety of RCC. The histological section revealed infiltrative tumor cells, arranged in diffuse large sheets showing scattered pleomorphic large cells with abundant clear cytoplasm, prominent nucleoli, and round nucleus. Atypical mitotic figures indicating a highly proliferative tumor with prominent multiple small-caliber blood vessels and diffuse areas of necrosis with hemorrhages were also well marked (Fig. 6).
Usually, patients with metastatic solitary lesion from primary RCC have longer survival, hence wide local resection and reconstruction of the skeletal defect remains the mainstay of management to prevent local disease progression and further complications. Intercalary re-section and reconstruction with bone cement- plate hybrid construct is an easy, safe and eco-nomical method of reconstruction for metaphysio-diaphyseal tumors where joint salvage is the aim.
Solitary bony metastatic deposit of Renal Cell carcinoma, 12 years after radical ne-phrectomy remains a rare entity. Wide local resection remains the mainstay of management, improving the long-term survival. Reconstruction of the intercalary bone defects with bone cement – plate hybrid con-struct remains a viable option in cases where the life expectancy is relatively short or when the patient cannot afford a prosthesis construct.
Bone cement – plate hybrid construct restores the limb function and improves the quality of living.
References
- 1.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108. [Google Scholar]
- 2.Kozlowski JM. Management of distant solitary recurrence in the patient with renal cancer. Contralateral kidney and other sites. Urol Clin North Am 1994;21:601-24. [Google Scholar]
- 3.Miyao N, Naito S, Ozono S, Shinohara N, Masumori N, Igarashi T, et al. Late recurrence of renal cell carcinoma: Retrospective and collaborative study of the Japanese society of renal cancer. Urology 2011;77:379-84. [Google Scholar]
- 4.Sugasawa H, Ichikura T, Ono S, Tsujimoto H, Hiraki S, Sakamoto N, et al. Isolated gastric metastasis from renal cell carcinoma 19 years after radical nephrectomy. Int J Clin Oncol 2010;15:196-200. [Google Scholar]
- 5.Choi WH, Koh YC, Song SW, Roh HG, Lim SD. Extremely delayed brain metastasis from renal cell carcinoma. brain tumor res treat. Korean Brain Tumor Soc 2013;1:99. [Google Scholar]
- 6.Puri A, Gulia A, Pruthi M, Koushik S. Primary cement spacers: A cost-effective, durable limb salvage option for knee tumors. Knee 2012;19:320-3. [Google Scholar]
- 7.Fuchs B, Trousdale RT, Rock MG. Solitary bony metastasis from renal cell carcinoma: Significance of surgical treatment. Clin Orthop Relat Res 2005;431:187-92. [Google Scholar]
- 8.Santoni M, Conti A, Procopio G, Porta C, Ibrahim T, Barni S, et al. Bone metastases in patients with metastatic renal cell carcinoma: Are they always associated with poor prognosis? J Exp Clin Cancer Res 2015;34:10. [Google Scholar]
- 9.Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J Clin Oncol 2010;28:1061-8. [Google Scholar]
- 10.Swanson DA, Orovan WL, Johnson DE, Giacco G. Osseous metastases secondary to renal cell carcinoma. Urology 1981;18:556-61. [Google Scholar]
- 11.Shankar K, Kumar D, Kumar KV, Premlata C. Renal cell carcinoma with unusual skeletal metastasis to tibia and ankle: A case report and review of literature. J Clin Diagn Res 2016;10:XD01-2. [Google Scholar]
- 12.Chawla A, Mishra D, Bansal R, Chundru M. Rare sites of delayed metastasis in renal cell carcinoma. BMJ Case Rep 2013;2013:bcr2013009971. [Google Scholar]
- 13.Merimsky O, Levine T, Chaitchik S. Recurrent solitary metastasis of renal cell carcinoma in skeletal muscles. Tumori 1990;76:407-9. [Google Scholar]
- 14.Chen CK, Chiou HJ, Chou YH, Tiu CM, Wu HT, Ma S, et al. Sonographic findings in skeletal muscle metastasis from renal cell carcinoma. J Ultrasound Med 2005;24:1419-23. [Google Scholar]
- 15.Di Tonno F, Rigon R, Capizzi G, Bucca D, Di Pietro R, Zennari R. Solitary metastasis in the gluteus maximus from renal cell carcinoma 12 years after nephrectomy: Case report. Scand J Urol Nephrol 1993;27:143-4. [Google Scholar]
- 16.Salman R, Sebaaly MG, Asmar K, Nasserdine M, Bannoura S, Khoury NJ. Rare skeletal muscle metastasis from renal cell carcinoma: Case report and review of the literature. CEN case reports. NLM (Medline) 2018;7:316-9. [Google Scholar]






