
Osteoid osteoma very rarely occurs in the talus, but should be a differential in a child presenting with ankle pain in the absence of history of trauma.
Dr. Satvik N Pai, Department of Orthopaedic Surgery, Sri Ramachandra Medical College and Research Institute, Chennai - 600 116, Tamil Nadu, India. E-mail: satvik.pai@gmail.com
Introduction:Osteoid osteoma is a benign, bone forming tumor which accounts for nearly 10% of all benign bone tumors. The foot is very rarely involved, with only around 2% of osteoid osteomas being reported to occur in bones of the foot. Osteoid osteoma of the talus could present as symptoms mimicking monoarticular arthritis of the ankle. We present a case of osteoid osteoma occurring in the neck of talus, presenting such a diagnostic dilemma.
Case Report:A 13-year-old male child had complaints of pain and swelling in his right ankle since 1 year. The pain was predominantly aggravated at night and partially relieved by non-steroidal anti-inflammatory drugs. On examination, we found a diffuse, ill-defined, and soft swelling over the anteromedial aspect of the right ankle, which was anterior and inferior to the medial malleolus. The movements at the ankle joint were restricted and painful. Lateral radiograph of ankle revealed a solitary, osteolytic, and circular lesion involving the neck of the talus. Computed tomography (CT) scan showed a well-defined, lucent, and intramedullary lesion with a sclerotic rim in the neck of talus. The child was diagnosed to have osteoid osteoma of the neck of talus. We performed percutaneous CT-guided radiofrequency ablation (RFA) of the lesion. The child had complete relief of pain after the procedure. The child was followed up for 3 years and had no complaints of pain.
Conclusion:Osteoid osteoma very rarely occurs in the talus. It can present as monoarticular arthritis involving the ankle joint and requires a high degree of suspicion to be identified. A CT scan remains the most accurate investigation to confirm the diagnosis. We found percutaneous CT-guided RFA to have yielded good outcome without recurrence.
Keywords:Osteoid osteoma, ankle arthritis, talus, radiofrequency ablation.
Osteoid osteoma is a benign, bone forming tumor which accounts for nearly 10% of all benign bone tumors [1]. The most common bones to be involved are femur and tibia. The foot is very rarely involved, with only around 2% of osteoid osteoma reported to occur in bones of the foot [2]. While osteoid osteoma occurring in long bones are usually intracortical, those present in the foot are of cancellous or subperiosteal subtypes. Osteoid osteoma involving the talus could present as symptoms mimicking monoarticular arthritis of the ankle [3], thus often delaying the accurate diagnosis. We present a case of osteoid osteoma occurring in the neck of talus, presenting such a diagnostic dilemma.
A 13-year-old male child had complaints of pain and swelling in his right ankle since 1 year. The pain was insidious in onset, had a dull aching character, and was non-radiating. The pain has increased in intensity over the past 1 year. The pain was predominantly aggravated at night and partially relieved by non-steroidal anti-inflammatory drugs (NSAIDs). They had noticed a diffuse swelling of his right ankle since about a year, which had gradually progressed in size over the past 6 months. The child did not have any other joint pain. He did not have any history of fever, weight loss, or loss of appetite. There was no history of trauma either. He was able to carry out his day-to-day activities; however, the pain had disturbed his sleep. He was known to have a seizure disorder and was on antiepileptic medications. His developmental milestones were appropriate for age and had no significant family history. On examination, we found a diffuse, ill-defined, and soft swelling over the anteromedial aspect of the right ankle, which was anterior and inferior to the medial malleolus. There was no local warmth; however, there was tenderness present in the region of the swelling. The skin in the region appeared normal. The range of movements at the ankle joint was restricted, with the child only able to do 20° of dorsiflexion, while he was able to do 40° of plantar flexion. The movements were associated with pain. The patient had full range of inversion and eversion at the subtalar joint and was not associated with pain.
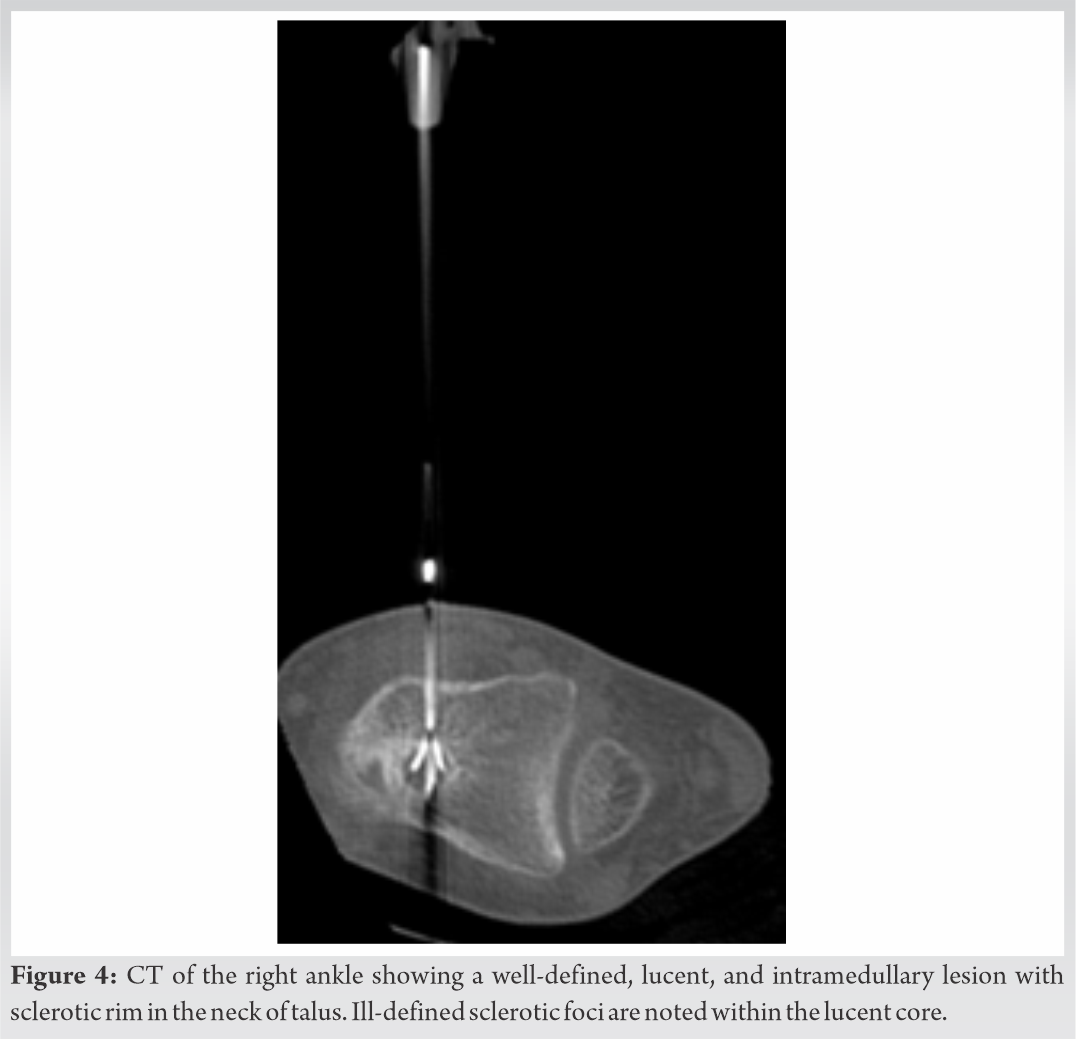
While the anteroposterior radiograph of the ankle appeared normal, the lateral radiograph of ankle (Fig. 1) revealed a solitary, osteolytic, and circular lesion involving the neck of the talus. The lesions had a homogenous matrix and a sclerotic rim, with a narrow zone of transition. Periosteal reaction was absent and soft-tissue appeared normal. The other bones and joints in the region appeared normal. Magnetic resonance imaging (MRI) (Fig. 2) showed a small T2 hyperintense lesion involving the dorsal aspect of the neck of talus, with diffuse bone marrow edema surrounding it. Computed tomography (CT) scan of the right ankle (Fig. 3) showed a well-defined, lucent, and intramedullary lesion with sclerotic rim in the neck of talus. It measured 9 × 7 × 8 mm in dimensions. Ill-defined sclerotic foci were noted within the lucent core. No obvious extraosseous extension was visible. The features were suggestive of osteoid osteoma. 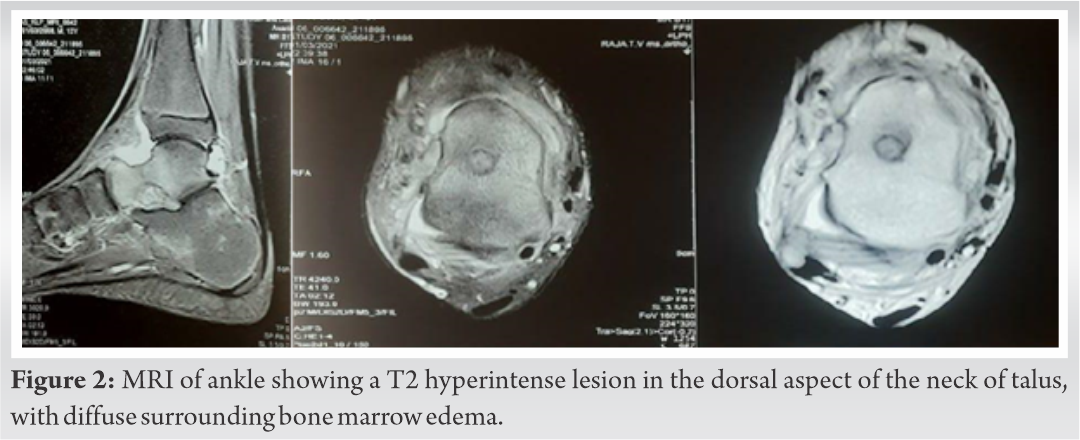 Blood investigations revealed a marginally elevated C-reactive protein and erythrocyte sedimentation rate, while the total count was within normal limits. The child was diagnosed to have osteoid osteoma in the neck of the talus. We performed radiofrequency ablation (RFA) of the lesion. Under CT guidance, the lesion was identified, and a 1 mm K-wire was drilled into the lesion. The electrode probe was then introduced into the lesion (Fig. 4). Ablation was done using radio waves for 6 min with the probe tip temperature set to 90°C. The child had complete resolution of pain after the procedure. The child was followed up for 3 years and was not found to have any complaints of pain.
Blood investigations revealed a marginally elevated C-reactive protein and erythrocyte sedimentation rate, while the total count was within normal limits. The child was diagnosed to have osteoid osteoma in the neck of the talus. We performed radiofrequency ablation (RFA) of the lesion. Under CT guidance, the lesion was identified, and a 1 mm K-wire was drilled into the lesion. The electrode probe was then introduced into the lesion (Fig. 4). Ablation was done using radio waves for 6 min with the probe tip temperature set to 90°C. The child had complete resolution of pain after the procedure. The child was followed up for 3 years and was not found to have any complaints of pain.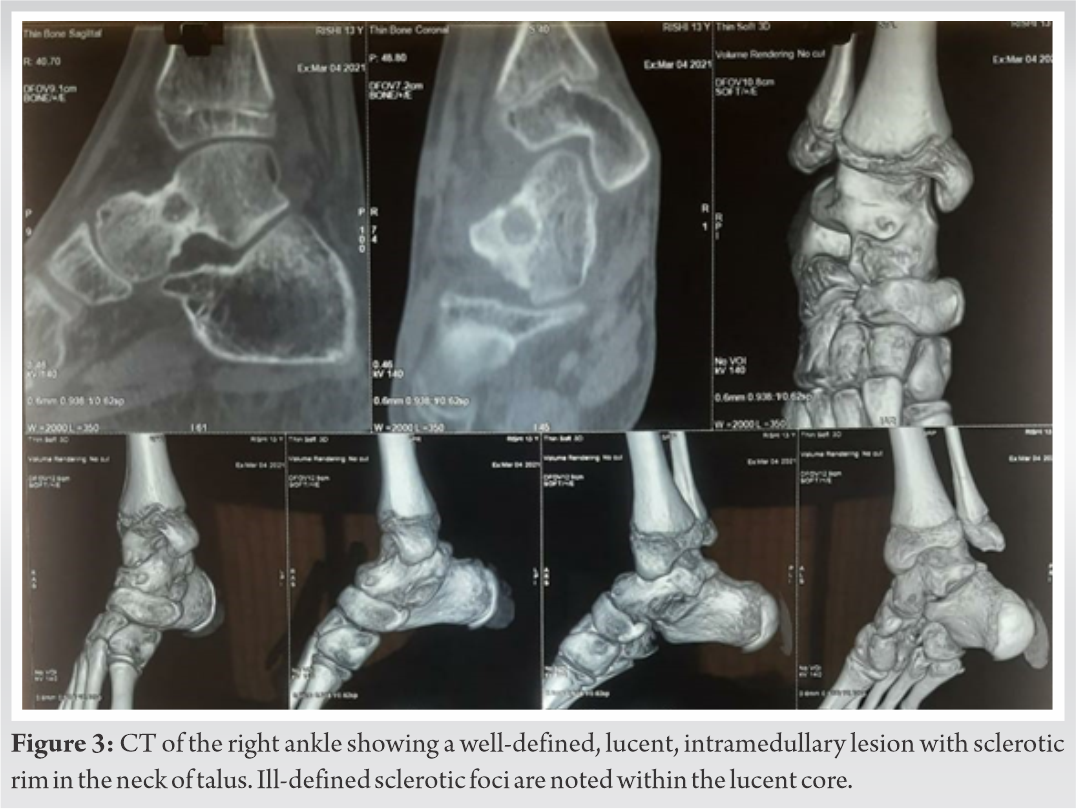
Osteoid osteoma involving the talus is extremely rare, with diversity of symptoms often leading to a delay in diagnosis. The classical symptom of nocturnal pain and relief with NSAIDs is reported to occur only in half the cases [4]. Swelling is postulated to occur due to the increased blood supply to the tumor resulting from prostaglandin release within the nidus. The mean age for osteoid osteoma in the foot is 12 years [4]. If a tumor is located close to a joint, like in our case, it can present with pain in the joint, joint effusion, or restriction of joint movements. On radiographs, it appears as small, round, and radiolucent nidus with surrounding sclerosis. A differential diagnosis of osteomyelitis, osteoblastoma and stress fracture have to be considered. The size of lesion being <1.5 cm in size ruled out osteoblastoma. Absence of a sinus tract, involucrum, or sequestrum helped to rule out osteomyelitis. Cortices were found to be intact, ruling out stress fracture. CT scan is the investigation of choice [2]. It classically shows a lucent nidus surrounded by sclerotic reactive bone. A central sclerotic dot may be present, described as a target shaped nidus [5]. MRI is less accurate than a CT due to bone marrow edema often masking the features of the tumor, it is helpful in the evaluation of cancellous lesions. In our case as well, the patient presented to us with a radiograph and an MRI already having been done at an outside center, due to which a definitive diagnosis could not be established. The CT scan showed typical features of osteoid osteoma, thereby confirming the diagnosis. Various treatment modalities are present for osteoid osteoma. Conservative management with NSAIDs is an option, with resolution of symptoms reported to occur at approximately 33 months [6]. However, the adverse impacts of long-term NSAID use, and high rate of recurrence following discontinuation of NSAIDs makes it less favorable. Historically, surgical excision-open en bloc resection was the most widely practiced procedure for cure. However, intraoperative visualization of the nidus is often difficult, and therefore, curative surgery can often lead to excessive bone removal, perioperative morbidity and may necessitate bone grafting procedures [7]. Arthroscopic excision has been found to be a less invasive alterative to open excision for management of osteoid osteoma in the talus [8, 9]. In recent times, RFA has been adopted as the standard treatment for osteoid osteoma, with more than 95% success rates [10]. Percutaneous CT-guided RFA of osteoid osteoma in talus has very scarce published literature; however, early results have shown similar results as elsewhere in appendicular skeleton [11]. The only major drawback of radiofrequency remains the lack of tissue for histological confirmation of diagnosis. Success of treatment has been assessed primarily in terms of resolution of pain [12] as radiological evidence of nidus remains post appropriate RFA as well.
Osteoid osteoma very rarely occurs in the talus. It can present as monoarticular arthritis involving the ankle joint and requires a high degree of suspicion to be identified. A computed tomography scan remains the most accurate investigation to confirm the diagnosis. We found percutaneous CT-guided RFA to have yielded good outcome without recurrence.
Osteoid osteoma very rarely occurs in the talus, but should be a differential in a child presenting with ankle pain in the absence of history of trauma. CT scan is the investigation of choice to confirm the diagnosis. Percutaneous CT-guided radiofrequency ablation is the most suitable procedure for osteoid osteoma of the talus.
References
- 1.Jordan RW, Koç T, Chapman AW, Taylor HP. Osteoid osteoma of the foot and ankle-A systematic review. Foot Ankle Surg 2015;21:228-34. [Google Scholar]
- 2.Dookie AL, Joseph RM. Osteoid Osteoma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537279 [Last accessed on 2020 Aug 08]. [Google Scholar]
- 3.Khan JA, Vaidya S, Devkota P, Acharya BM, Pradhan NM, Shrestha S. Subperiosteal osteoid osteoma of the neck of talus. JNMA J Nepal Med Assoc 2009;48:58-61. [Google Scholar]
- 4.Papachristos IV, Michelarakis J. Riddles in the diagnosis and treatment of osteoid osteoma in child foot: A concisive study. Foot Ankle Surg 2016;22:97-102. [Google Scholar]
- 5.Lewis VO, Morris CD, Parsons TW. Malignant and benign bone tumors that you are likely to see. Instr Course Lect 2013;62:535-49. [Google Scholar]
- 6.Atesok KI, Alman BA, Schemitsch EH, Peyser A, Mankin H. Osteoid osteoma and osteoblastoma. J Am Acad Orthop Surg 2011;19:678-89. [Google Scholar]
- 7.Singh DK, Katyan A, Kumar N, Nigam K, Jaiswal B, Misra RN. CT-guided radiofrequency ablation of osteoid osteoma: Established concepts and new ideas. Br J Radiol 2020;93:20200266. [Google Scholar]
- 8.Ge SM, Marwan Y, Addar A, Algarni N, Chaytor R, Turcotte RE. Arthroscopic management of osteoid Osteoma of the ankle joint: A systematic review of the literature. J Foot Ankle Surg 2019;58:550-4. [Google Scholar]
- 9.Hetsroni I, Nyska M, Edelshtein E, Mann G, Palmanovich E. Arthroscopic excision of osteoid osteoma of the talus. Arthrosc Tech 2017;6:e839-43. [Google Scholar]
- 10.Gebauer B, Collettini F, Bruger C, Schaser KD, Melcher I, Tunn PU, et al. Radiofrequency ablation of osteoid osteomas: Analgesia and patient satisfaction in long-term follow-up. Rofo 2013;184:959-66. [Google Scholar]
- 11.Daniilidis K, Martinelli N, Gosheger G, Hoell S, Henrichs M, Vogt B, et al. Percutaneous CT-guided radio-frequency ablation of osteoid osteoma of the foot and ankle. Arch Orthop Trauma Surg 2012;132:1707-10. [Google Scholar]
- 12.Tanrıverdi B, Salık AE, Çetingök H, Edipoğlu E, Bilgili MG, Güven K, et al. Multidisciplinary approach in the treatment of osteoid osteoma with radiofrequency ablation. Joint Dis Relat Surg 2020;31:255-9. [Google Scholar]


