
In the setting of a floating lower extremity, we recommend urgent surgical intervention and the utilization of a percutaneous schanz pin in the proximal femur with gentle manipulation for reduction.
Dr. James Satalich, Department of Orthopaedic Surgery, Virginia Commonwealth University Health System, 1200 East Broad Street, 9th Floor Box 980153, Richmond, Virginia. E-mail: James.Satalich@vcuhealth.org
IntroductionSurgical management of isolated acetabular fracture dislocations, femoral shaft fractures, and tibial shaft fractures are well-documented, but there is limited literature on the acute management of these injuries when they occur concomitantly in the same patient on the ipsilateral extremity. We present a case of the acute treatment of a 33-year-old patient with a right ipsilateral floating hip and knee injury secondary to a motor vehicle accident. We offer a unique surgical technique for the urgent management of this rare combined injury.
Case PresentationA 33-year-old female presented to our trauma center with an ipsilateral acute posterior wall fracture dislocation, femoral head impaction fracture, femoral shaft fracture, and tibial shaft fracture. After a failed hip reduction attempt in the emergency department, she was urgently brought to the operating room for further management. She underwent percutaneous-assisted schanz pin reduction of the hip, intramedullary nail fixation of the femur and tibia, and dynamic fluoroscopic examination of the hip under anesthesia.
ConclusionSuccessful management of the rare combined floating hip and knee injury requires urgent intervention. The reduction of the hip dislocation is difficult due to the associated injuries. We recommend urgent surgical intervention and the utilization of a percutaneous schanz pin in the proximal femur with gentle manipulation. In most cases, this can effectively reduce the hip without a formal open approach.
KeywordsFloating hip, floating knee, hip dislocation, hip fracture dislocation.
Floating joint fractures are orthopedic skeletal injuries involving disruption of bone above and below a joint [1]. They are predominantly due to high energy trauma secondary to motor vehicle accidents, or falls from height, but may occur secondary to low energy trauma in the elderly [2, 3]. Surgical management of isolated acetabular dislocation, femoral shaft fractures, or tibial shaft fractures is well-documented in the literature, but there is a paucity of literature on the acute management and immediate stabilization of these injuries when they are associated together on the ipsilateral extremity. This is due in part secondary to the rarity of this injury, with floating hips having an incidence of one in 10,000 fractures [4].
Due to the nature of this trauma and associated long bone injuries, the reduction of the hip in the trauma bay is extremely difficult. Furthermore, floating knee injuries can be associated with highly morbid injuries to the head, chest, and abdomen, thus aggressive stabilization may help reduce complications in this patient population [5]. If hip reduction must be delayed, developing an order of operations is especially important due to the risk of complications including avascular necrosis of the femoral head (AVN), and sciatic nerve palsy in up to 26–35% of floating hip injuries [6]. At this time, there is no surgical technique documented in the literature on how to treat this acute injury.
We present the unique case of the acute treatment of a 33-year-old patient with the right ipsilateral floating hip and knee injuries secondary to a motor vehicle accident and offer an operative technique not described in the literature.
A 33-year-old female, with a medical history of schizophrenia and bipolar disorder, presented to our trauma center after being an unrestrained driver in a motor vehicle crash going approximately 50 miles/h. Her accident was a high impact mechanism.
In the trauma bay, the patient complained of the right hip and leg pain and was found to have associated shortening and deformity of the extremity. There was a 2 cm × 1 cm open laceration over the distal tibia with exposed bone fracture fragments. The patient was intubated for airway protection and radiographs were obtained of the right hip, femur, and lower leg demonstrating a right hip fracture dislocation with associated right femoral and tibial shaft fractures (Fig. 1-3).
Computed tomography (CT) scan of the pelvis further delineated the posterosuperior hip dislocation with associated fractures of the posterior wall of the acetabulum and femoral head (Fig. 4).
Attempts in the emergency department to obtain a closed reduction of the hip dislocation were unsuccessful due to difficulty posed by her femur and tibia fractures. To reduce the hip and minimize the risk of developing AVN, she was taken urgently to the operating room for surgical management. In the operating room, the patient was placed supine on a radiolucent table with a small bump underneath the right buttock. Given the nature of her hip injury, priority was given to the reduction of the hip dislocation. A 5 mm Schanz pin was placed percutaneously along the axis of the femoral neck (Fig. 5).
Traction and gentle rotation were applied to reduce the femoral head back into the acetabulum (Fig. 6) and an inferior infrafoveal femoral head impaction fracture was confirmed.
Next, the open tibia fracture was debrided, closed primarily and both the tibia and femoral shaft fractures were treated with intramedullary nails (Fig. 7-9).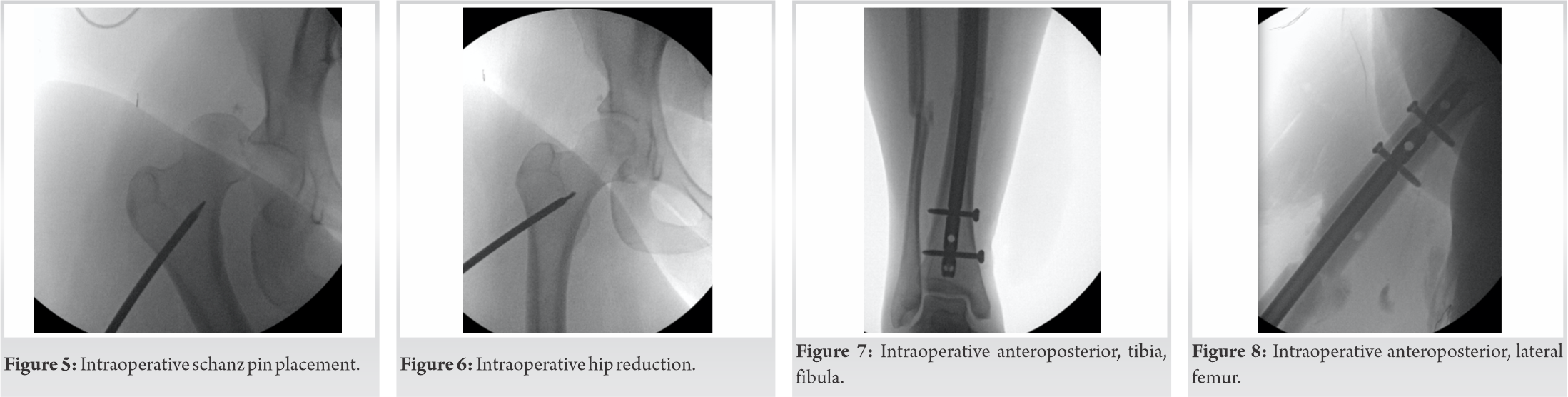
Finally, a fluoroscopic dynamic examination under anesthesia, as described by Moed et al., was performed to assess the stability of the posterior wall acetabulum fracture [7].
The posterior wall of the acetabulum and hip joint was found to be stable in 90° of flexion with internal rotation, adduction and axial loading. The post-operative pelvic CT scan demonstrated a concentric hip reduction with a known femoral head fragment in the inferior portion of the hip joint (Fig. 10).
The patient was made toe-touch weight-bearing on the right lower extremity and discharged from the inpatient rehabilitation unit on post-operative day 16. The patient returned to the emergency department approximately 6 weeks later for suture removal, and it was discovered that she was placing full weight on her right lower extremity. Radiographs obtained during this encounter demonstrated maintenance of hip joint congruency and healing femoral and tibial fractures (Fig. 11-14).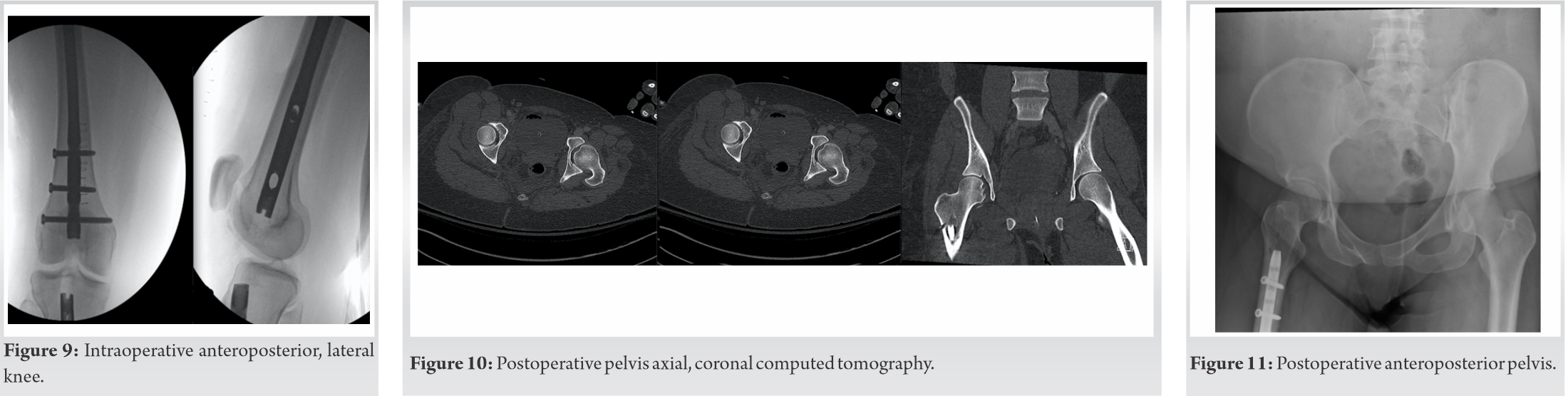

Despite being given an appointment for follow-up in our orthopedic outpatient center, she was not seen in our clinic again.
The management of isolated acetabular dislocation, femoral shaft fractures, or tibial shaft fractures is well documented. There are limited treatment recommendations for the unique situation when a patient presents with all three injuries on the ipsilateral limb. Several studies have advocated for the stabilization of femoral shaft fractures before the reduction of acetabular fractures, but they did not feature cases of hip dislocations [8, 9]. There must be a plan for immediate stabilization to reduce the hip and minimize the risk of complications. Kellam and Ostrum meta-analysis of avascular necrosis after traumatic hip dislocations found that “time to reduction” of >12 h was associated with a significantly higher risk of AVN than reductions performed in <12 h [10]. If reducing the hip is not feasible on arrival in the trauma bay, we advise surgical management. Due to the rare nature of this injury and the lack of surgical treatment options described in the literature, we recommend this specific operative technique.
Placement of a 5 mm schanz pin into the proximal femur, as described in the paper, allows for gentle and controlled reduction of the femoral head into the acetabulum. Given the difficulty in controlling the proximal femur due to the long bone injuries, the schanz pin allows for traction, rotation, and easy manipulation of the proximal femur for femoral head reduction. This subsequently allows for further fluoroscopic assessment of the hip and treatment of any additional fractures involving the joint.
This technique has not been documented in the literature and offers surgeons an alternative treatment method in this rare and acute injury.
In the acute management of a patient with a dislocated hip, femoral shaft fracture, and tibial shaft fracture, immediate treatment must be initiated to reduce the native hip and minimize the risk of AVN and other complications. This injury is extremely rare and there are limited surgical treatment recommendations in the literature. If presented with this rare scenario and the hip is non-reducible in the trauma bay, we recommend urgent operative intervention utilizing a percutaneous schanz pin in the proximal femur for controlled reduction of the femoral head and subsequent treatment of the long bone injuries per standard and accepted practice.
When presented with a patient with an ipsilateral dislocated hip, femoral shaft fracture, and tibial shaft fracture and the hip is not reducible in the emergency department, treatment recommendations in the literature are sparse. We are recommending the surgical treatment above, one that has not been described in the literature.
References
- 1.Ng AB, Soong VK, Maguire MP, Hopgood P, Shepard GJ. Concomitant ipsilateral floating hip and floating knee injuries: A unique injury and review of the literature. Int J Clin Pract 2007;61:1585-7. [Google Scholar]
- 2.Mohamed SO, Ju W, Qin Y, Qi B. The term “floating” used in traumatic orthopedics. Medicine (Baltimore) 2019;98:e14497. [Google Scholar]
- 3.Kumar CY, Nalini KB, Nagaraj P, Jawali A. Ipsilateral floating hip and floating knee-a rare entity. J Orthop Case Rep 2013;3:3-6. [Google Scholar]
- 4.Rajasekaran RB, Jayaramaraju D, Palanisami DR, Perumal R, Shanmuganathan R. Ipsilateral acetabular fracture with displaced femoral head and femoral shaft fracture: A complex floating hip injury. Case Rep Orthop 2018;2018:4937472. [Google Scholar]
- 5.Rollo G, Falzarano G, Ronga M, Bisaccia M, Grubor P, Erasmo R, et al. Challenges in the management of floating knee injuries: Results of treatment and outcomes of 224 consecutive cases in 10 years. Injury 2019;50:S30-8. [Google Scholar]
- 6.Tiedeken NC, Saldanha V, Handal J, Raphael J. The irreducible floating hip: A unique presentation of a rare injury. J Surg Case Rep 2013;2013:rjt075. [Google Scholar]
- 7.Moed BR, Ajibade DA, Israel H. Computed tomography as a predictor of hip stability status in posterior wall fractures of the acetabulum. J Orthop Trauma 2009;23:7-15. [Google Scholar]
- 8.Burd TA, Hughes MS, Anglen JO. The floating hip: Complications and outcomes. J Trauma 2008;64:442-8. [Google Scholar]
- 9.Liebergall M, Mosheiff R, Safran O, Peyser A, Segal D. The floating hip injury: Patterns of injury. Injury 2002;33:717-22. [Google Scholar]
- 10.Kellam P, Ostrum RF. Systematic review and meta-analysis of avascular necrosis and posttraumatic arthritis after traumatic hip dislocation. J Orthop Trauma 2016;30:10-6. [Google Scholar]





