
Performing an arthroscopic AC joint reconstruction with a looped allograft and hook plate fixation can successfully restore the dislocation.
Dr. James Satalich, Department of Orthopaedic Surgery, Virginia Commonwealth University Hospital, 1250 E. Marshall Street, Richmond, Virginia 23219. E-mail: james.satalich@vcuhealth.org
Abstract
Introduction: Acromioclavicular Joint (ACJ) dislocations can lead to increased pain and disability. On failure of conservative management, surgical intervention is often recommended. At present, there is no gold standard surgical technique to treat this pathology. The current surgical options include coracoclavicular screw, hook plate (HP), endobutton coracoclavicular fixation, ligament reconstruction, and among others. Unfortunately, all these techniques have been reported to have increased complications such as recurrent dislocation, impingement, and among others.
Case Report: A 41-year-old healthy male presented to the clinic with a symptomatic chronic right Grade 3 ACJ dislocation. He failed conservative treatment, including NSAID’s, rest, and physical therapy. We agreed to pursue an arthroscopic assisted ACJ reconstruction with allograft and joint fixation with a HP. Using a combined technique, we performed an arthroscopic-assisted ACJ reconstruction with an allograft and supplemental HP for additional fixation. This case report details the unique technique. Using this technique, the patient had improved pain and ACJ stability long-term. After 6 months, the HP was removed and the patient continued to remain asymptomatic and without instability.
Conclusion: An arthroscopic-assisted ACJ reconstruction and HP fixation provide orthopedic surgeons a novel technique for the treatment of an ACJ dislocation. Further prospective studies are still recommended for further evaluation.
Keywords: Acromioclavicular joint dislocation, hook plate, arthroscopy.
The acromioclavicular joint (ACJ) serves as the primary connection between the axillary skeleton and the upper extremity and is a common site of dislocation. The incidence is 9.2 per /1000 person-years (highest in the 20 and 30-year-old range) [1] and occurs 5 times more frequently in males than females. The Rockwood Classification System consists of six types of ACJ injuries with unique qualities and degrees of injury to the ligaments and connective tissue within the joint capsule [2]. It is widely considered that Types IIIb, IV, and VI necessitate surgical reconstruction of the joint to avoid chronic pain and instability [2,3]. Surgery remains an option for Types IIIa and V though supportive data isare lacking regarding optimal surgical technique [2,4]. The current surgical options include coracoclavicular screw, hook plate (HP), endobutton coracoclavicular fixation, ligament reconstruction, and among many others. There have been multiple reported complications with each isolated procedure, those including impingement with the HP hook plate, recurrent dislocation using the endobutton, and among others. [9]. To prevent increased complications, this case offers a novel approach utilizing arthroscopic assistance for an open HP Hook Plate technique (HP) fixation with an allograft lasso for reduction and fixation.
A 41-year-old healthy male who presented to the clinic with a symptomatic chronic right Grade 3 ACJ dislocation (Fig. 1).
He failed conservative treatment, including NSAID’s, rest, and physical therapy. His pain was located over her ACJ and worsened with increased activity. Due to his continued symptoms along with failed conservative treatment, surgical intervention was recommended. We agreed to pursue an arthroscopic-assisted ACJ reconstruction with allograft and joint fixation with a HP hook plate. We agreed that the HP hook plate will be removed at 6 months due to long- term complications such as impingement, irritation, and among others. In the operating room, a standard posterior arthroscopic portal was established. Arthroscope was inserted into the glenohumeral joint. A second portal was established in the anterior aspect of the shoulder under direct visualization. Supraspinatus, infraspinatus, and teres minor were intact. At this time, ArthroCare wand was then used to release all soft tissues underlying the coracoid. This was then debrided back and completed with the arthroscopic shaver. We were able to outline the coracoid back to its base, exposing the undersurface of it. At this time, using direct visualization, we established a second anterolateral portal. Two cannulas were placed. The first was in the first anterior portal and second was in the second anterolateral portal. At this time, intraoperative fluoro was brought in. A curvilinear incision centered over the clavicle was then made. Dissection was carried down exposing the superior surfaces. Soft tissue was elevated both anterior posterior, which was in the main portion of the clavicle. Then, using fluoroscopic assistance, we were able to place a switching stick into the clavicle and lateral to the coracoid. This was dilated over. FiberStick suture was then inserted and the suture was retrieved out for graft passage. We then placed the switching stick posterior to the clavicle and medial to the coracoid. This was again confirmed under intraoperative fluoro. We were able to retrieve out Tiger stick suture passer. We then were able to shuttle in the posterior tib allograft nicely having the graft present on the undersurface of the coracoid (Fig. 2).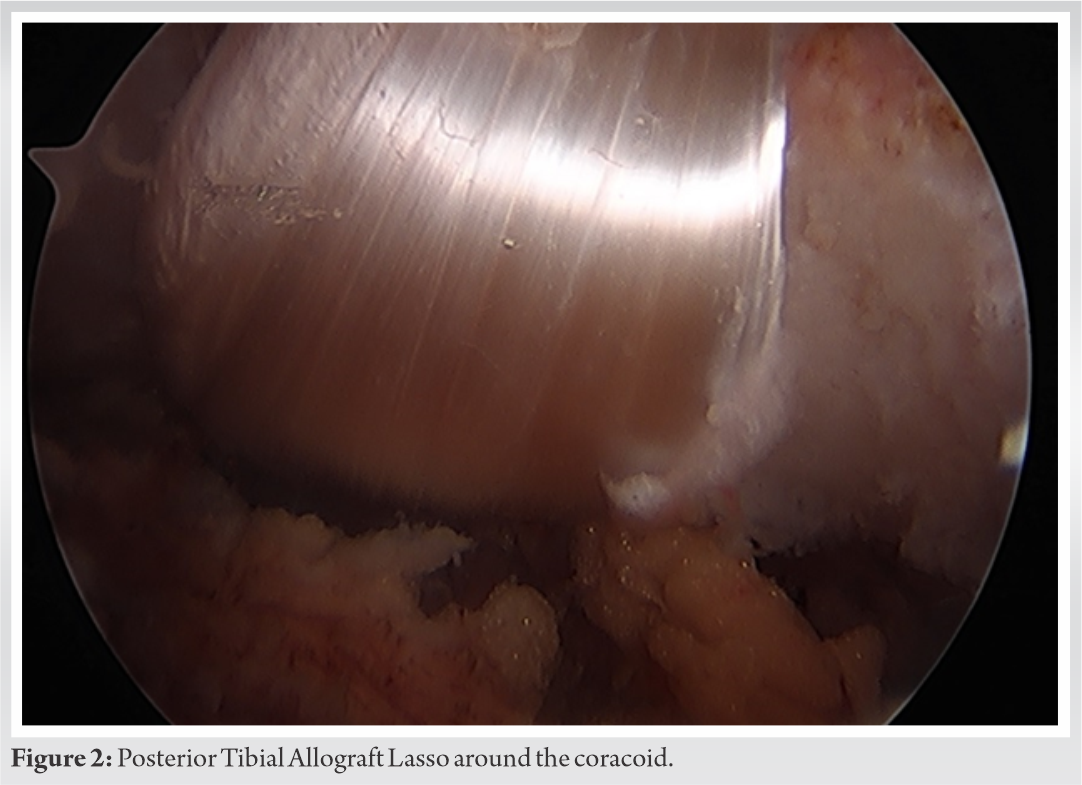
Next, we proceed with the distal clavicle excision. The distal end of the clavicle was exposed with electrocautery. Based upon pre-operative imaging, it was felt that 10 mm resection was indicated. The amount of resection was marked. This was confirmed to be appropriate on intraoperative fluoro. Oscillating TPS saw was then use to perform resection. The degenerative distal clavicle was removed. Following resection, we then under fluoroscopic evaluation confirmed that a 15 mm 7-hole HP hook plate was appropriate size . This helped reduce the clavicle nicely down appropriately. We then held the reduction with a ball-tip guide pusher. The graft was then crossed over in a crossing fashion and this was tied to itself using #2 FiberWire in a figure-of-eight fashion. The clavicle HP hook plate was then positioned appropriately, overlying the graft that was just tied. This acts as an adjuvant to ensure the graft position is stable. Three bicortical screws were placed medially. One locking screw was placed laterally. Fluoroscopic evaluation showed appropriate reduction of the ACJAC joint with good length and position of the hardware. Post operatively, the patient denied any increased pain or instability. X-rays showed a well reduced AC Joint (Fig. 3). 
At the 6-month post-operative mark, due to some superficial irritation from the plate, we surgically removed the HP hook plate and the AC Joint remained well reduced. Now 2 years out from surgery, there has been no reported complications in her outcomes.
Unfortunately, currently, there is no consensus that has been reached for a premier surgical technique for ACJ reconstruction. Instead, the large body of techniques, both open and arthroscopic, possesses pros and cons which require surgical decision-making in choosing the appropriate management of the injury [6]. Arthroscopic procedures for ACJ fixation have become popular among physicians and patients alike due to being minimally invasive and helpful in diagnosing and treating any concomitant intra-articular pathology during the procedure. However, arthroscopic suture implants may fail to maintain reduction and stabilization in all planes, and cause irritability to movement [6]. This is seen in the technique utilizing endobutton with tight rope fixation, as some studies have shown elevated loss-of-reduction rates due to horizontal translation and instability [5,8]. In the literature, there have been reports with up to a 27.1% complication rates, one including hardware failure and loss of reduction leading to pain and instability [9] . HP Hook plate fixation provides rigid fixation and a well reduced ACJAC joint but comes with reported complications. Those include increased reports of impingement, rotator cuff lesions, and bony erosion [5]. There haves been reports that up to 12% of cases with only HP hook plate reduction resulted in joint dislocation post operatively. There have also been reports of up to 37.5% of patients developed post-operative impingement [9,10] . Therefore, due to the diverse outcomes in the literature in all surgical techniques, further research and novel ideas are needed to treat ACJAC joint reconstructions. This case introduces a novel technique using a combination of arthroscopy, ligament reconstruction using a lasso technique, and temporary HP hook plate fixation. Performing an arthroscopy allows the surgeon to evaluate the joint, minimizes the additional open incisions and soft tissue damage, decreases the infection risk, and ensures precise graft position and stability. This provides the ultimate stability of the ACJAC joint with the combination of both ligament and plate reduction techniques. To prevent overloading and provide stress shielding of the graft in the acute setting, the HPhook plate is utilized by achieving rigid fixation of the ACJAC joint. After the acute setting, the HPhook plate can be removed and in this case the ACJAC joint remains well reduced.
This case report provides orthopaedic surgeons with a novel technique for ACJAC joint reconstruction that utilizes arthroscopic-assisted ligament reconstruction along with HP hook plate fixation. The goal of this technique is to provide a stable ACJAC joint without the complications that are associated when only performing the isolated ligament reconstruction or HP hook plate reduction.
This case educates both surgeons and patients that there is a novel surgical technique that has good patient outcomes in the treatment of ACJAC joint dislocations with minimal complications.
References
- 1.Pallis M, Cameron KL, Svoboda SJ, Owens BD. Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med 2012;40:2072-7. [Google Scholar | PubMed]
- 2.Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the rockwood classification for acromioclavicular joint injuries. Arthroscopy 2014;30:271-8. [Google Scholar | PubMed]
- 3.Frank RM, Cotter EJ, Leroux TS, Romeo AA. Acromioclavicular joint injuries: Evidence-based treatment. J Am Acad Orthop Surg 2019;27:e775-88. [Google Scholar | PubMed]
- 4.Petri M, Warth RJ, Greenspoon JA, Horan MP, Abrams RF, Kokmeyer D, et al. Clinical results after conservative management for grade III acromioclavicular joint injuries: Does eventual surgery affect overall outcomes? Arthroscopy 2016;32:740-6. [Google Scholar | PubMed]
- 5.Wang C, Meng JH, Zhang YW, Shi MM. Suture button versus hook plate for acute unstable acromioclavicular joint dislocation: A meta-analysis. Am J Sports Med 2020;48:1023-30. [Google Scholar | PubMed]
- 6.Gowd AK, Liu JN, Cabarcas BC, Cvetanovich GL, Garcia GH, Manderle BJ, et al. Current concepts in the operative management of acromioclavicular dislocations: A systematic review and meta-analysis of operative techniques. Am J Sports Med 2019;47:2745-58. [Google Scholar | PubMed]
- 7.Woodmass JM, Esposito JG, Ono Y, Nelson AA, Boorman RS, Thornton GM, et al. Complications following arthroscopic fixation of acromioclavicular separations: A systematic review of the literature. Open Access J Sports Med 2015;6:97-107. [Google Scholar | PubMed]
- 8.Hann C, Kraus N, Minkus M, Maziak N, Scheibel M. Combined arthroscopically assisted coraco-and acromioclavicular stabilization of acute high-grade acromioclavicular joint separations. Knee Surg Sports Traumatol Arthrosc 2018;26:212-20. [Google Scholar | PubMed]
- 9.Lee S, Bedi A. Shoulder acromioclavicular joint reconstruction options and outcomes. Curr Rev Musculoskelet Med 2016;9:368-77. [Google Scholar | PubMed]
- 10.Lin HY, Wong PK, Ho WP, Chuang TY, Liao YS, Wong CC. Clavicular hook plate may induce subacromial shoulder impingement and rotator cuff lesion-dynamic sonographic evaluation. J Orthop Surg 2014;9:6. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation
August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report
July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report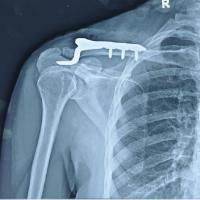 February 1, 2025 A Rare Complication of Hook Plate Fixation for Lateral Clavicle Fractures: Salvage Management with K-Wire Fixation
February 1, 2025 A Rare Complication of Hook Plate Fixation for Lateral Clavicle Fractures: Salvage Management with K-Wire Fixation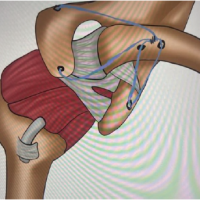 November 1, 2024 Pediatric AC Joint Fracture Dislocation: Arthroscopy-assisted Reduction and Internal Bracing
November 1, 2024 Pediatric AC Joint Fracture Dislocation: Arthroscopy-assisted Reduction and Internal Bracing