
Good reconstruction and stabilization of distal ulna stump are important for good functional outcome.
Dr. Abhineet Verma, Sri Aurbindo Medical College and Post Graduate Institute, Indore, Madhya Pradesh, India. E-mail: sunnyv_20@yahoo.co.in
IntroductionAmong the benign primary bone tumors, Giant cell tumor (GCT) accounts for about 3% to –5%. It is a locally aggressive tumor with maximum incidence between 20 to and 40 years of age. The sites where GCT is most commonly seen are distal femur, and proximal tibia followed by distal end radius. Distal end of ulna is a rare site with an incidence of only 0.45% to –3.2%.
Case ReportWe report a case of a 32- year- old male with (GCT) giant cell tumor of the left distal ulna. We managed the patient with en bloc resection of distal ulna along with reconstruction of distal radio ulnar joint (DRUJ) and triangular fibro cartilage complex (TFCC) using proximal fibula graft and palmaris longus graft. DRUJ was stabiliszed with a k- wire.
ConclusionAfter 1 year of follow- up, patient showed good results in terms of range of movements of the wrist joint with no evidence of recurrence.
KeywordsGiant cell tumor, Distal ulna, Distal radio-ulnar joint, Proximal fibular graft, Palmaris longus graft.
Giant-cell tumor (GCT) is a rare tumor of the bone which is benign in nature and locally invasive. It has an incidence of about 3–5% among all primary bone tumors [1]. The age group in which it is commonly prevalent is 20–40 years. It usually presents in the metaphysis of long bones and can extend up to the epiphysis. Distal femur and proximal tibia followed by distal end of radius are the most common sites involved [2]. Among all the sites of occurrence of GCTs, the distal end of ulna is extremely rare, which accounts for only 0.45–3.2% [3]. Malignant transformation of GCTs is rare, however, when present in the wrist joint approximately 12% of these can convert to malignant tumors.
The treatment of GCT of distal ulna is a challenging procedure due to its close proximity with distal radio ulnar joint (DRUJ) and carpal bones.
A 32-year-old Indian male presented with pain and swelling over his ulnar aspect of the left distal forearm for 20 days. Patient had history of trauma due to fall from bike 20 days back following which he developed pain and swelling over left distal forearm. Conservative management with B/E slab and analgesics was given in a private clinic. There was no history of any constitutional signs or symptoms. The family, occupational, and histories were not significant. The general physical and systemic examinations were normal.
On local examination, there was an oval swelling of 3 × 2 cm in the left distal end of the ulna over dorsomedial aspect. The skin over the swelling was normal with no overlying scar, sinus, or prominent veins. There was no local rise of temperature. The swelling was tender and consistency was firm. There was no adherence to the overlying skin but the swelling was fixed to the underlying bone. Active and passive range of motion of the left wrist joint was diminished compared with the contralateral side. There was no distal neurovascular deficit.
Plain radiograph of wrist showed a lytic lesion involving left distal ulna with expansion and ballooning of cortex with pathological fracture without any periosteal reaction. (Fig. 1) Computed tomograms showed expansile osteolytic lesion seen in lower end of ulna measuring approximately 30 × 21 × 26 mm size with patchy cortical breach extending up to articular surface of the wrist (Fig. 2).
A diagnosis of GCT was made clinically. Biopsy was done to confirm the diagnosis.
Patient was treated with en bloc resection with reconstruction of distal ulna with fibular graft and DRUJ stabilization with palmaris longus graft and k-wire.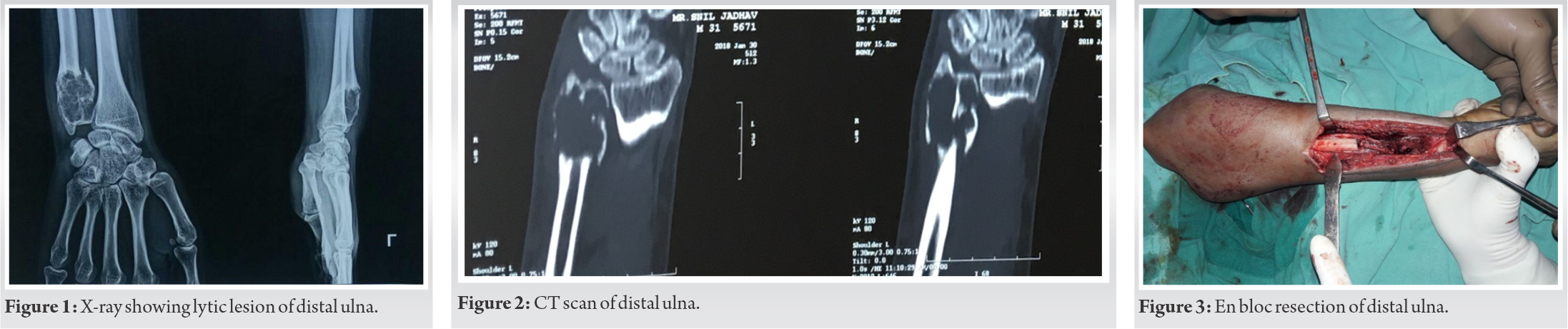
Through a 12 cm longitudinal incision made over dorsomedial aspect of distal ulna, en bloc resection of distal ulna of 8 cm with 2 cm safe margin was done (Fig. 3). Proximal fibular cortical graft from ipsilateral side was taken and fixed to distal ulna stump with a 7-hole DCP. Palmaris longus tendon was harvested and used as a tendon graft for the reconstruction of the triangular fibro cartilage complex (TFCC) and DRUJ as described by Adams and Berger in the treatment of chronic DRUJ instability. This construct was stabilized with a k-wire across the fibular graft and distal radius (Fig. 4). An above elbow cast with a window for dressing of the incision site was given and limb elevation was advised. Suture removal was done after POD 12 with removal of cast after 4 weeks and follow-up was taken at 3 months, 6 months, and 1 year. Following removal of the cast, physiotherapy was started. He started gradually regaining his strength and movements following physiotherapy. After 1 year, sound union of the graft was noted with good functional range of movements at wrist and forearm with excellent hand grip and no evidence of carpal instability or recurrence of the tumor (Fig. 5-7).
GCT is a rare primary benign bone tumor. It commonly occurs between the age group of 20–40 years. Primary GCT of distal end of ulna is a rare site for occurrence of this tumor with incidence of 0.45–3.2%. Being a rare site, the treatment for GCT of distal ulna is a challenging procedure. The treatment is directed toward complete removal of the involved part with safe margins and reconstruction and stabilization of distal ulnar stump and DRUJ to avoid recurrence and preservation of joint function.
Various methods have been described for GCT of distal end ulna. A study by Cooney et al. showed excellent results in six out of eight patients that underwent en bloc resection of distal ulna without reconstructive procedure for the osseous defect [4]. On the contrary, many authors have documented poor functional results following en bloc resection of distal ulna without DRUJ reconstruction due to reasons like pain and restriction of movements [5].
The Darrach’s procedure done for the degenerative conditions which involve resection of distal ulna is not comparable to resection of distal ulna in case of tumors for various reasons [6].
In young patients with high functional demand, there is a need for anatomical reconstruction and stabilization of distal ulnar stump and DRUJ. Different techniques have been suggested for reconstruction of distal ulna and DRUJ following en bloc resection of distal ulna for primary tumors [7].
Lasso tenodesis of ulnar stump with palmaris longus graft was reported by Gainor in two cases of GCT of distal ulna [8]. Goldner and Hayes were first to describe ECU tenodesis to stabilize the ulnar stump in 1979 based on their experience in 225 patients [9]. Ulnar buttress arthroplasty following en bloc resection has been described by Hashizume using larger iliac bone graft and using screw and k-wire to attain buttress against axial loading [10].
From the literature review, it can be understood that reconstruction of DRUJ along with stabilization of the ulnar stump is important in any functionally demanding individual, following en bloc resection of the distal ulna. In our technique, proximal fibula graft was used as it is more anatomically similar to the distal ulna. We had replaced the fibular graft, for entire length of the ulna resected. Proximally, a 7-holed narrow DCP was used to stabilize the fibular graft with the ulnar stump. Furthermore, in our technique, DRUJ and TFCC were reconstructed with Palmaris longus graft using the technique, similar to the one described by Adams and Berger for DRUJ reconstruction in chronic DRUJ instability [11].
Our case, a 32-year-old functionally demanding male with GCT of distal ulna treated using this new technique of reconstruction of the entire length of excised distal ulna, DRUJ and TFCC using proximal fibula, Palmaris tendon graft, k-wires, and dynamic compression plate showed excellent radiological and functional results.
GCT of distal ulna is a very rare occurrence. Being a rare site, the treatment for GCT of distal ulna is a challenging procedure. Keeping this in view, our treatment is directed toward complete removal of the involved part with safe margins and reconstruction and stabilization of distal ulnar stump and DRUJ to avoid recurrence and preserve good joint function.
References
- 1.McDonald DJ, Sim FH, McLeod RA, Dahlin DC. Giant-cell tumor of bone. J Bone Joint Surg Am 1986;68:235-42. [Google Scholar]
- 2.Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar]
- 3.Goldenberg RR, Campbell CJ, Bonfiglio M. Giant-cell tumor of bone. An analysis of two hundred and eighteen cases. J Bone Joint Surg Am 1970;52:619-64. [Google Scholar]
- 4.Cooney WP, Damron TA, Sim FH, Linscheid RL. En bloc resection of tumors of the distal end of the ulna. J Bone Joint Surg Am 1997;79:406-12. [Google Scholar]
- 5.Bieber EJ, Linscheid RL, Dobyns JH, Beckenbaugh RD. Failed distal ulna resections. J Hand Surg Am 1988;13:193-200. [Google Scholar]
- 6.Noble J, Arafa M. Stabilisation of distal ulna after excessive Darrach’s procedure. Hand 1983;15:70-2. [Google Scholar]
- 7.Kayias EH, Drosos GI, Anagnostopoulou GA. Resection of the distal ulna for tumours and stabilisation of the stump. A case report and literature review. Acta Orthop Belg 2006;72:484-91. [Google Scholar]
- 8.Gainor BJ. Lasso stabilization of the distal ulna after tumor resection: A report of two cases. J Hand Surg Am 1995;20:324-6. [Google Scholar]
- 9.Goldner JL, Hayes MG. Stabilization of the remaining ulna using one half of the extensor carpi ulnaris tendon after resection of the distal ulna. Orthop Trans 1979;3:330-31. [Google Scholar]
- 10.Hashizume H, Kawai A, Nishida K, Sasaki K, Inoue H. Ulnar buttress arthroplasty for reconstruction after resection of the distal ulna for giant cell tumour. J Hand Surg Br 1996;21:213-5. [Google Scholar]
- 11.Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg Am 2002;27:243-51. [Google Scholar]





