
First rib fracture cases should always be examined and investigated to exclude vascular, neural and lung damage.
Dr. Nareshkumar Satyanarayn Dhaniwala, Department of Orthopedics, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences (Deemed to be University), Sawangi Meghe, Wardha - 442 001, Maharashtra, India. E-mail: nsdhaniwala@gmail.com
IntroductionFirst rib fracture is a very uncommon injury due to protection provided to it by clavicle. In isolation, it may be associated with neurovascular injury rarely but as part of poly trauma the first rib fracture may be associated with vascular injury in significant number of cases. There is definite role of computed tomography scan thorax in diagnosis of this fracture which can be missed on X-ray chest. Management includes early diagnosis of associated life-threatening complications and its prompt treatment.
Case ReportA case of poly trauma associated with right first rib fracture with subclavian artery thrombosis resulting in gross ischemia of the right upper limb and fractures in the right upper limb and right lower limb long bones is reported. The patient developed signs of ischemia and lung complications 24 h later. Subclavian artery damage was diagnosed on Doppler ultrasound and angiography. The case was managed by surgical repair of subclavian artery damage and stabilization of fractures.
ConclusionThe case is reported to highlight association of first rib fracture with life-threatening complication of subclavian artery laceration causing extensive swelling around shoulder, ischemia to the right upper limb, lung damage, and problem of its detection and management.
KeywordsFirst rib fracture, life-threatening injuries, subclavian artery, thrombosis.
First rib fracture is a very uncommon injury, due to protection provided to it by clavicle. As an isolated fracture it may be associated with neurovascular injury in 3% cases and as part of polytrauma it may be associated with vascular injury in more than 24% cases [1]. Neurovascular complications may occur due to damage to subclavian vein, subclavian artery or both along with damage to brachial plexus cords leading to variable amount of weakness, ischemia, or both. First rib fractures are considered indicators of increased morbidity and mortality in major trauma. Intra thoracic and extra thoracic injuries are more likely with first rib fracture than other rib fractures. This fracture is taken as an important predictor of injury severity and poly trauma independent of mechanism of injury, age, and gender. There is an association between head, cervical spine, chest, liver and pelvic injuries, and first rib fracture [2]. First rib is relatively broad and lies in a protected position needing high energy trauma to cause its fracture. Posteriorly directed trauma to upper thorax or shoulder, direct blow to sternum, and direct trauma causing fracture clavicle are the common modes of injury [1, 3]. A strong sudden contraction of scalenus anterior and stress fractures are other described mechanisms of injuries [4, 5, 6]. Fracture first rib may not be seen on X-ray chest always hence there is a role of chest computed tomography (CT) scan in patients having major blunt trauma to chest [7, 8]. With increased detection of first rib fracture due to CT scan, one requires detailed evaluation to exclude life-threatening injuries associated with it. Herein a case of right first rib fracture along with subclavian artery laceration and thrombosis leading to ischemia of the right upper limb and fractures in multiple long bones is reported to highlight the problem of associated life-threatening injuries and its management.
A 28-year-old male driving a motor cycle collided against the back side of a turning three-wheeler auto rickshaw and fell down on road with great force sustaining open injuries to right thigh, right leg and closed injury to right forearm and right wrist. He was brought to the nearby emergency department of tertiary care hospital where fast intravenous fluids were given after primary assessment. The patient was under alcoholic influence and in severe hypovolemic shock. There were 12 cm and 10 cm long oblique deep lacerated wounds on his right thigh and right leg, respectively. His extremities were cold, more on the right side and there was no pulsation of right posterior tibial artery and dorsalis pedis. The patient had equal breathing on both sides of chest and no clinical evidence of any spinal or left sided limb injury. X-rays of the limbs showed comminuted fractures of the lower shaft right femur extending into knee, comminuted fracture of right tibia fibula, displaced comminuted fracture of both bone right forearm, fracture lower end of right radius and fracture of head and neck of right second metacarpal (Fig. 1-4).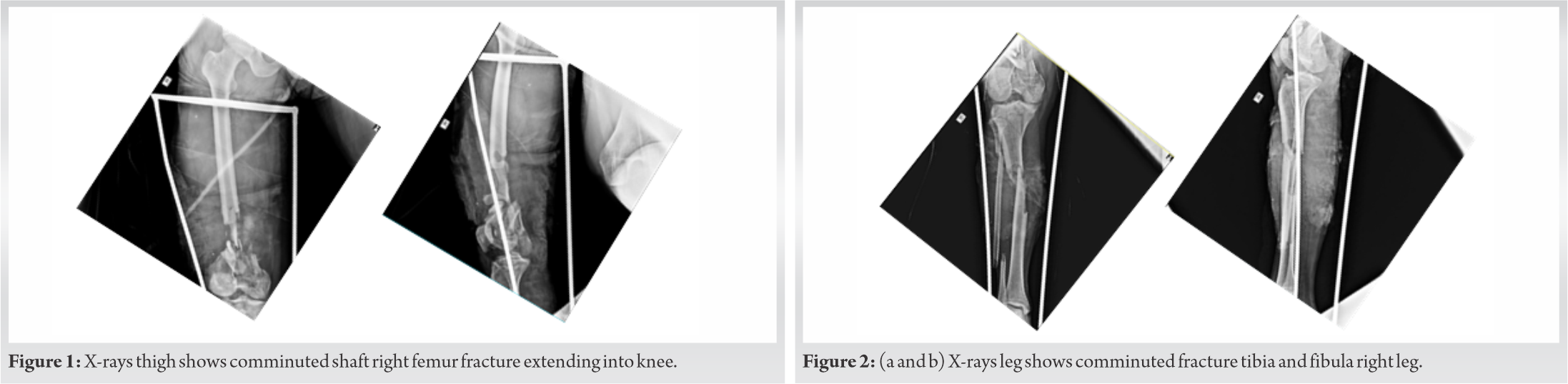
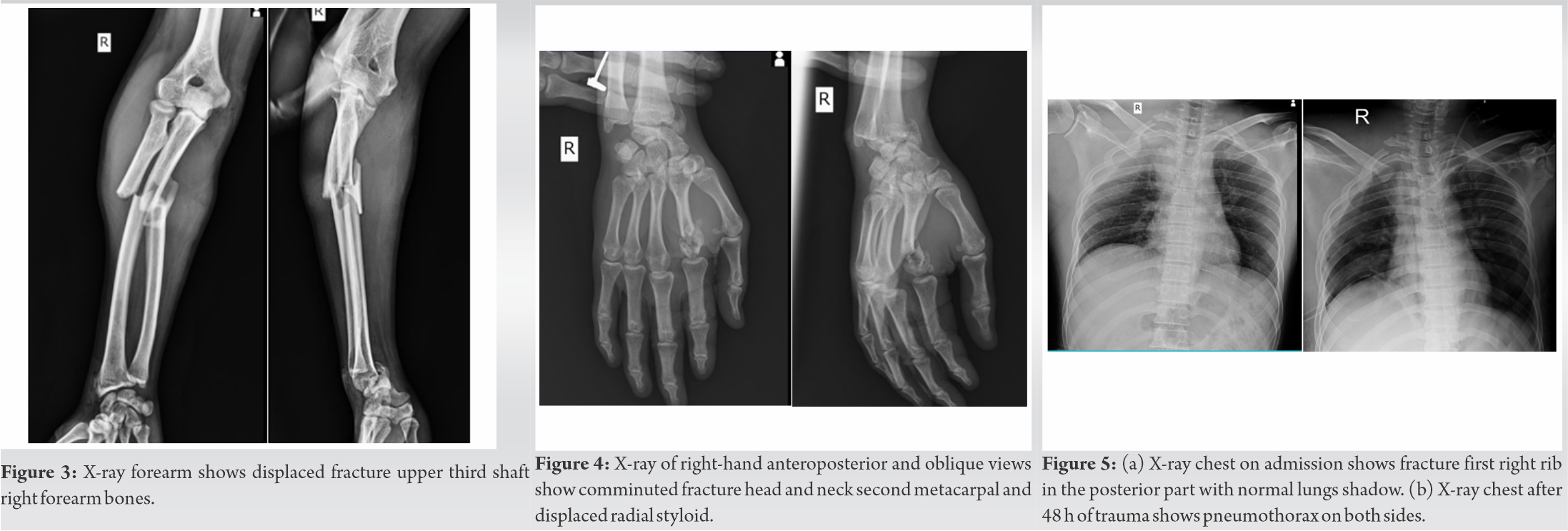
The patient was resuscitated and stabilized. The lower limbs wounds were debrided and the fractures in femur and tibia fibula were stabilized with long external fixator spanning across the knee. Right upper limb was splinted in above elbow slab. The chest X-ray showed displaced fracture of first right rib posteriorly near the neck of the rib (Fig. 5). As the blood pressure of the patient was fluctuating despite adequate blood and fluids infusion, he needed continuous vasopressor drugs and oxygen inhalation. 24 h after trauma the right upper limb of the patient was noted to be cold and cyanosed with decreased sensation till mid right arm. Doppler study showed no flow from distal axillary artery and moderate to gross edema/hematoma around subclavian vessel. High Resolution CT scan of thorax showed mix density collection in right pleural space with sub segmental atelectasis of medial, anterior, lateral basal segment of the right lower lobe of lung and the presence of pneumothorax on left side, besides fracture of posterior part of first rib on the right side and fracture spinous process of C5, C6, and C7 vertebrae (Fig. 6). CT right upper limb angiogram was done soon after which showed thrombotic occlusion of 2nd and 3rd part of subclavian artery and axillary artery with reformation of distal axillary artery and brachial artery along with occlusion of distal brachial artery, radial artery, and ulnar artery. Meanwhile, the patient had developed huge subcutaneous swelling in right chest, axillary, and right shoulder area. The air entry was also noted to be decreased. His right upper limb circulation did not improve and the limb remained cold, insensitive, and darker in appearance indicating slow developing gangrene. Closed embolectomy was attempted, but it improved the blood flow temporarily only. Closed intramedullary nailing of ulna was done to prevent abnormal mobility of the forearm bones. The patient was referred urgently to higher center for vascular intervention. The patient was operated in emergency. The thrombus in subclavian artery was removed and the laceration of 2.5 cm × 1.0 cm was repaired. This helped in arresting the gangrene progression in the right upper limb and stabilized his general condition. He needed amputation only till wrist level. His long bones fractures were stabilized further as per standard treatment protocol.
First rib fractures have been classified as posterior, lateral or anterior depending on its location and as nondisplaced, minimal displaced, or displaced. Serious vascular injuries are seen when the fracture is near posterior part of rib and significantly displaced. Vascular injury can occur due to a violent lever mechanism in which posterior portion of the rib is displaced downwards and anterior part forced upward, thus pinching the content of the thoracic outlet against the clavicle [9]. Isolated first rib fracture results rarely in major vascular injury although with fracture displacement its incidence increases [1]. Gupta et al. noted vascular injury in 24% of cases when first rib fracture was associated with head, thoracic, abdominal, and long bone trauma [1]. The most common site of fracture is at the subclavian sulcus and neck of the first rib posteriorly. On chest X-ray widened mediastinum, upper limb pulse deficit, posteriorly displaced first rib fracture, subclavian grove fracture anteriorly, brachial plexus injury, and expending hematoma are considered as indicators for subclavian artery and aortic arch arteriography [1]. Philips et al. described 45 patients with 49 first rib fracture who underwent angiography and noted serious vascular injuries in 14% cases of which five had posterior injuries and one had lateral fracture and one had anterior fracture. All these cases had displaced fractures of the first rib. He noted brachial plexus injury only in association with vascular injury and managed majority of first rib fracture cases (78%) without arteriography [9]. Delayed subclavian artery rupture has also been reported secondary to traumatic first rib fracture [10]. CT scan of chest as the primary mode of imaging in major trauma cases detects higher number of first rib fractures than chest X-ray [8]. Traumatic brain injuries, cardiac injuries, brachial plexus injuries, and cervical spine injuries have been noted in various studies [11, 12, 13]. These studies highlight that there is a need to be more alert while dealing with patients who have first rib fractures. The reported case is having fractures of the right first rib with fractures in the right upper limb and lower limb long bones. His chest did not show any obvious abnormality and fracture rib was seen on X-ray chest only. He developed ischemia in the right upper limb slowly along with swelling around the chest and his lung function started deteriorating gradually. He developed pneumothorax first on the left side and then on the right side. Inter costal drainage underwater seal was done for pneumothorax. Doppler ultrasound followed by the right upper limb angiography clinched the diagnosis of subclavian artery laceration and thrombosis which was repaired by the vascular surgeon stopping the further progression of the condition and saving the patient. Better perfusion of the right upper limb limited the extent of gangrene up to hand only. The patient could be saved only because of diagnosis and prompt repair of subclavian artery laceration without which he would have succumbed to his injuries. The above case highlights the complications of subclavian artery damage associated with ischemia to the limb, vertebral damage at C5, C6, and C7 spinous process, multiple bone fractures and subcutaneous expanding hematoma in chest and shoulder region along with lung damage and pneumothorax. The combination of these injuries is life-threatening and can cause prolonged morbidity and early mortality as noted in many such studies [12, 13]. The gradual development of vascular and lung complications might be missed if proper and regular evaluation of the patient is not done. Repeated X-ray of the chest and or CT scan is necessary for early detection of complications. First rib fractures may also be associated with head injury, cervical spine injury, and abdominal injury with liver damage. Its diagnosis can be made on chest X-ray but in many cases, patients may have intra thoracic complications and fracture may be missed on X-ray chest. Hence, CT scan of chest should be done [10, 13].
Fracture right rib along with multiple fractures in the right upper and lower limb long bones in a young male following blunt trauma upper chest is reported to highlight associated subclavian artery thrombosis leading to the right upper limb ischemia, lung complications, role of angiography, and prompt surgical intervention.
First rib fracture, an uncommon injury should be evaluated clinically and by imaging to detect associated life-threatening complications for early diagnosis and prompt treatment to avoid prolonged morbidity and early mortality.
References
- 1.Gupta A, Jamshidi M, Rubin JR. Traumatic first rib fracture: Is angiography necessary? A review of 730 cases. Cardiovasc Surg 1997;5:48-53. [Google Scholar]
- 2.Sammy IA, Chatha H, Lecky F, Bouamra O, Fragoso-Iñiguez M, Sattout A, et al. Are first rib fractures a marker for other life-threatening injuries in patients with major trauma? A cohort study of patients on the UK Trauma Audit and Research Network database. Emerg Med J 2017;34:205-11. [Google Scholar]
- 3.Woodring JH, Fried AM, Hatfield DR, Stevens RK, Todd EP. Fractures of first and second ribs: Predictive value for arterial and bronchial injury. Am J Roentgenol 1982;138:211-5. [Google Scholar]
- 4.Sinha S, Mummidi SK, Londhe S, Campbell AC. Isolated fracture of the first rib without associated injuries: A case report. Emerg Med J 2001;18:315. [Google Scholar]
- 5.Atin J, Yashwant ST, Masood H, Vijay J. First rib fractures: Not always a hallmark of severe trauma-a report of three cases. Chinese J Traumatol 2013;16:251-3. [Google Scholar]
- 6.Qureshi T, Mander BJ, Wishart GC. Isolated bilateral first rib fractures-an unusual sequel of whiplash injury. Injury 1998;29:397-8. [Google Scholar]
- 7.Kea B, Gamarallage R, Vairamuthu H, Fortman J, Lunney K, Hendey GW, et al. What is the clinical significance of chest CT when the chest X-ray result is normal in patients with blunt trauma? Am J Emerg Med 2013;31:1268-73. [Google Scholar]
- 8.Traub M, Stevenson M, McEvoy S, Briggs G, Lo SK, Leibman S, et al. The use of chest computed tomography versus chest X-ray in patients with major blunt trauma. Injury 2007;38:43-7. [Google Scholar]
- 9.Phillips EH, Rogers WF, Gaspar MR. First rib fractures: Incidence of vascular injury and indications for angiography. Surgery 1981;89:42-7. [Google Scholar]
- 10.Tennyson C, Karunaratne D, McLaughlin KE, Hasan R, Grant SW. Delayed subclavian artery rupture secondary to a traumatic first rib fracture. Trauma Case Reports 2018;16:1. [Google Scholar]
- 11.Fermanis GG, Deane SA, Fitzgerald PM. The significance of first and second rib fractures. Aust N Zeal J Surg 1985;55:383-6. [Google Scholar]
- 12.Poole GV Jr., Myers RT. Morbidity and mortality rates in major blunt trauma to the upper chest. Ann Surg 1981;193:70. [Google Scholar]
- 13.Richardson JD, McElvein RB, Trinkle JK. First rib fracture: A hallmark of severe trauma. Ann Surg 1975;181:251. [Google Scholar]








