
This case report highlights an uncommon scenario of neglected glass shard in the knee joint and arthroscopy is an effective minimally invasive modality to retrieve such foreign bodies, particularly from hidden areas of the joint with least soft-tissue damage.
Dr. Sameer Panchal, Department of Orthopaedics, Sir HN Reliance Hospital and Research Centre, Mumbai - 400 004, Maharashtra, India. Email: panchalsameer1992@gmail.com
Abstract
Introduction: Knee joint is not an uncommon site for penetrating injuries and a spacious articulation to accommodate foreign body. Extensive literature is available on removal of loose bodies and metallic foreign bodies from the knee joint with sparse documentation of unusual intruders.
Case Presentation: We report an atypical case of neglected glass fragment retrieved from the knee joint of 26-year-old male by arthroscopy, who presented to us 14 months after the index injury, in view of sudden onset excruciating pain following bike ride.
Conclusion: Arthroscopy is the preferred minimally invasive modality for removal of foreign bodies from the knee joint, particularly from deeper and remote areas of knee joint. Appropriate pre-operative radiological imaging aids in better understanding of the anatomical location, improves surgical orientation, and shortens the duration of surgery. A high degree of suspicion and a meticulous history taking is important to reach the appropriate diagnosis.
Keywords: Knee joint, glass shard, foreign body, arthroscopy.
Foreign bodies are not uncommon in tibiofemoral articulation. Loose bodies are the most frequent free-floating body retrieved form the knee joint in background of persistent knee pain and locking episodes. Although exact incidence of loose bodies in knee joint is not known, one of the reports quantifies at around 24.3% [1]. External foreign bodies such as metallic piece, bullets, and glass shards are more exceptional and are particularly found following penetrating trauma. We report a case of 26-year-old male who sustained penetrating trauma to the right knee due to direct impact on glass door. The most of the glass fragment was removed after the index trauma, but unknowingly a piece of glass was left behind that was the reason for persistent pain with which the patient presented to us.
A 26-year-old male accountant by profession presented to our outpatient department with complaints of sudden onset right knee. The pain started after a motor bike ride 2 weeks back and while he reported some relief with anti-inflammatory drugs, the pain kept recurring, and got precipitated with any deep flexion activity including stair climbing. He also reported locking episodes. Further detailed history revealed that the patient sustained penetrating trauma to the right knee 14 months back. Glass shard pierced anterolateral aspect of the knee due to direct impact over the glass door. Patient was immediately taken to local hospital and penetrated glass shard was removed under sedation. As per the patient, local wound exploration was meticulously executed and primary closure performed following thorough wash and debridement. The wound healed by primary intention and patient was able to resume activities of daily within 2 weeks. The only radiological investigation done at the time was the X-rays and they were reported to be not suggestive of bony injury. 6 months after the index injury patient still had a sense of feeling something inside the joint and experienced pain during ground level activities. Patient visited again in view of the complaints and re-exploration was performed from the previous scar. A small glass piece was retrieved anew from the deeper extra-articular tissue as evident from the history narrated by the patient. No further investigations were advised. Patient was assured regarding complete removal of the glass fragment and was sent home. Patient was absolutely fine till few days back he experienced sudden onset excruciating pain in the right knee after bike ride. With this background, patient came to us with apparently normal looking knee and healed scar of around 5 cm over anterolateral aspect of the right knee. Clinical examination was not suggestive of any significant ligamentous injury. Tenderness was elicited over deep flexion. Radiographs done at this time did raise a suspicion of possible foreign body in notch area (Fig. 1). Computed tomography (CT scan) was advised with suspicion of remnant glass shard inside the joint and delineate the topographic location with respect to the joint. CT scan revealed hyperdense foreign body within the joint measuring approximately 15*6 mm situated anterior to lower one-third of anterior cruciate ligament (ACL) (Fig. 2). Patient was posted for arthroscopic retrieval of the foreign body after anesthetic evaluation and was also consented for a possible open exploration.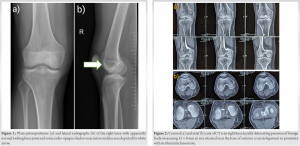
Standard arthroscopic knee portals were taken. Synovial fluid expressed from the portals was collected and sent for culture and sensitivity. A dry scopy without fluid irrigation was performed with the anxiety of migration of intra-articular foreign body. Once the foreign body location was identified, the irrigation pump was switched on and joint was thoroughly irrigated. Shiny glass shard was now clearly visualized near the base of ACL (tibial attachment site) (Fig. 3a). The particle was not freely mobile and was retrieved calmly with the help of grabber measuring roughly around 1.5 cm with jagged edges (Fig. 4a and b). There was minimal fibrosis over distal part of ACL which was debrided using a motorized shaver post removal of the glass piece (Fig. 3b and 3c). To our surprise, fortunately, the rest of the joint was pristine with healthy medial and lateral compartments (Fig. 3d). Thorough lavage was given and portals were closed with monocryl 3-0. Patient was put on rehabilitation immediately from next day. Final culture reports were negative of any growth.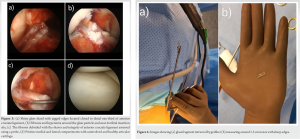
Postoperatively patient reported complete resolution of the symptoms and regained the entire range of movement. He was discharged next day with standard post-operative care instructions. Histopathological analysis of retrieved piece confirmed that it was glass and there was no fibrosis or any accompanying softy tissue foreign body reaction.
The highlight of this case report is retrieval of neglected glass shard through arthroscopy which is currently the accepted modality for foreign body removal with exceptions in rare circumstances. The key lesson learnt from this case report is importance of meticulous history taking, clinical assessment, and need for relevant imaging and careful interoperation of the radiographs. Inappropriate pre-operative evaluation by radiological imaging has led to three surgeries for complete removal of the penetrated glass fragment with detrimental socioeconomic impact. While not seen in this case, a sharp foreign body has the potential to damage the chondral surface with detrimental consequences.
The literature mentions about different kind of foreign bodies retrieved from the knee joint, commonly with antecedent trauma history – needle, bullet [2], palm tree thorn [3], pencil-lead [4], and mercury thermometer [5]. Radiolucent foreign bodies classically glass particle has increased likelihood of being missed on standard radiographs. There are hardly such interesting cases with similar background reported in the literature pertaining to diagnosis and management of foreign body in the knee joint. One such case highlighted an uncommon injury where the glass foreign body initially extra-articular migrated within the joint over period of years and was retrieved arthroscopically in an extracapsular location through a vent in the posterior capsule [6]. Another novel report demonstrated arthroscopic glass body removal from knee joint without history of any preceding trauma or scars/entry wounds on knee [7]. Interestingly, in this report, middle-aged patient with history of osteoarthritis received intra-articular injection for pain relief and these glass foreign bodies retrieved during arthroscopy originated from glass vials broken while withdrawing medication for intra-articular injection in the knee joint. Another curious case documented arthroscopic retrieval of glass foreign body which was misdiagnosed as ACL avulsion fracture on plain radiographs without preceding history of trauma [8].
Foreign body within a joint can potentially be an orthopedic crisis which requires urgent extraction. The consequences would be serious if left alone or neglected; hence, prompt removal is mandatory [9]. The authors were pleasantly surprised by the fact that structures within the knee joint including menisci, articular cartilage, ACL, and PCL were intact with no evidence of synovitis. There were mild fibrosis and hyperemia near the base of ACL where the glass shard was found. Mobile and sharp foreign bodies are known to cause chondral damage and ligament injuries. A fascinating report documented incomplete ACL tear with around 20% fibers affected sustained due to glass foreign body in a 13-year-old adolescent boy and emphasized on the fact that swift removal of such intruders would avoid serious articular damage [10]. The authors extensively reviewed the literature and found some interesting case reports where glass body was retrieved as a foreign body form the knee joint, which has been arranged in a tabulated format (Table 1).
This case report highlights the basic fact that even in the background of penetrating trauma, chances of buried foreign body are high particularly with radiolucent structures like glass fragment. Arthroscopy is the preferred treatment of choice for removal of such intruders in most of the situations. Meticulous wound exploration and appropriate radiological imaging are essentials to certain in-toto removal of the foreign body and avoid repetitive surgery.
Neglected foreign bodies are not uncommon within the knee joint. Timely removal of these bodies is extremely crucial for maintenance of milieu interior of the joint and prevent further inflammatory reaction and soft-tissue injury. Arthroscopy can be a preferred surgical modality for retrieval of these foreign bodies with minimal soft tissue damage particularly from inaccessible areas within the joint.
References
- 1.Mahmood A, Shivarathre DG, Howard K, Parkinson RW. Incidence of loose bodies and baker’s cysts in the arthritic knee. JOJ Orthop Orthoplast Surg 2018;2:555576. [Google Scholar | PubMed]
- 2.Haspl M, Bojanic I, Pecina M. Arthroscopic removal retrieval of metal foreign bodies the knee joint after war wounds. Injury 1996;27:177-9. [Google Scholar | PubMed]
- 3.Kahn B. Foreign body (palm thorn) in knee joint. Clin Orthop Relat Res 1978;135:104-6. [Google Scholar | PubMed]
- 4.Lee BI, Choi HS, Kim JB, Min KD. Arthroscopic retrieval of a very rare penetrating foreign body of the knee. Arthroscopy 2004;20:1071-4. [Google Scholar | PubMed]
- 5.Theodorou SD, Vlachos P, Vamvasakis E. Knee joint injury by mercury from a broken thermometer: Case report and review of the literature. Clin Orthop Relat Res 1981;160:159-62. [Google Scholar | PubMed]
- 6.Devgan A, Mudgal KC. An unusual case of foreign body knee that spontaneously migrated inside and out of the joint: Arthroscopic removal. Knee Surg Sports Traumatol Arthrosc 2007;15:758-60. [Google Scholar | PubMed]
- 7.Hafez MA, Al-Dars AM. Glass foreign bodies inside the knee joint following intra-articular injection. Am J Case Rep 2012;13:238-40. [Google Scholar | PubMed]
- 8.Sharma S, Rampurada A, Rees AJ. A glass foreign body in the knee joint mistaken for ACL avulsion: An unusual case. Knee Surg Sports Traumatol Arthrosc 2007;15:766-8. [Google Scholar | PubMed]
- 9.Atamanov IA, Marchenkova NM, Golovkin SI, Kukushkin II. Foreign bodies in the knee joint in children. Vestn Khir Im I I Grek 1980;125:84-7. [Google Scholar | PubMed]
- 10.Shishir SM, Harsh KA, Kanagasabai R, Gnanadoss JJ. An unusual case of partial Anterior Cruciate ligament (ACL) tear secondary to a glass foreign body in an adolescent knee joint. J Orthop Case Rep 2016;6:13-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes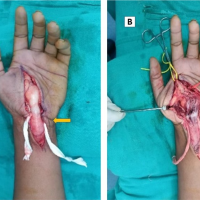 February 10, 2024 Fibrolipomatous Hamartoma Over the Left Forearm and Palm
February 10, 2024 Fibrolipomatous Hamartoma Over the Left Forearm and Palm October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report
October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report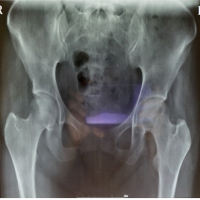 January 10, 2023 Biological Therapy for Avascular Necrosis of Femoral Head – A Case Report
January 10, 2023 Biological Therapy for Avascular Necrosis of Femoral Head – A Case Report