
Some symptomatic cases of adiponecrosis due to mass effect or pain may require surgical en bloc excision for adequate relief.
Dr. Shlok Patel, Department of Orthopedics, B. J Medical College, Ahmedabad, Gujarat, India. E-mail: pshlok27@gmail.com
Abstract
Introduction: Fat necrosis can occur in any area rich in fatty tissue. It occurs due to aseptic saponification of the fat by lipases. The most common site of it is the breast.
Case Presentation: This article reports the case of a 43-year-old woman that came into the orthopedic outpatient department with a history of two masses, one on each buttock. The patient had a history of surgical excision of adiponecrotic mass from the right knee a year back. All the three masses appeared around the same time. Ultrasonography was done to surgically excise the left gluteal mass. The histopathology of the excised mass then confirmed subcutaneous fat necrosis.
Discussion and Conclusion: Fat necrosis can also be found in the knee and buttocks, and that too without any definite etiology. Imaging and biopsy can help with the diagnosis. It is necessary to familiarize oneself with adiponecrosis so as to differentiate it from other grave conditions that it mimics, such as cancer.
Keywords: Fat necrosis, adiponecrosis, saponification, buttock, lipomatous tumor.
Fat necrosis is a benign condition that can affect any area rich in fatty tissue, most commonly the breast. The major contributor to fat necrosis is aseptic saponification of fat, caused primarily by blood and tissue lipases. Common causes of fat necrosis are trauma, surgery, or radiotherapy [1,2]. Acute pancreatitis can also lead to fat necrosis, typically in the peripancreatic retroperitoneum, omentum, and/or mesenteric root. Saponification due to pancreatitis may be related to fat necrosis in retroperitoneum or distant subcutaneous, periarticular, or marrow fat [3]. We report a case of a patient presenting with fat necrosis in three sites (knee and both buttocks) concurrently. Not much literature is available supporting such an unusual presentation.
A 43-year-old woman presented with a complaint of progressive increase in difficulty sitting due to swellings on each buttock. She has a history of a similar swelling on the right knee, which was diagnosed as fat necrosis histopathologically after excision of the mass 1 year ago. She complained about the gluteal swellings only 15 days back due to the embarrassing site of the lump and because she started facing discomfort while sitting. On further inquiry, she reported that both the knee and gluteal swellings appeared at the same time 3 years back and have been growing since. She has no history of any trauma, surgery, fever, or abdominal pain. On examination, both gluteal masses were non-warm, non-tender, and approximately 8 cm × 5.5 cm in size. The lumps were firm and fixed with the skin, but were mobile over the deeper tissues. Ultrasonography of both gluteal masses was done. It showed mixed echogenic heterogeneous fatty tissue in the gluteal region in subcutaneous planes, which suggested fat necrosis-inflammation more likely over lipomatous tumor. The left gluteal mass was then excised through an incision made directly over the lump (Fig. 1).
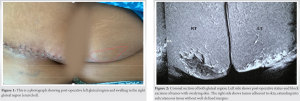
The lump was found adhered to the skin. The lump was removed along with the adherent skin and histopathological investigation was done, which supported a diagnosis of subcutaneous fat necrosis. Blood reports of the patient were normal except for slight anemia. There was no evidence of a prior attack of pancreatitis. After left mass excision, magnetic resonance imaging (MRI) was done to supplement the diagnosis (Fig. 2, 3). A fairly well-circumscribed oval abnormal signal intensity area in the skin and subcutaneous soft tissue was seen in the posterior right gluteal region. The lesion measured 7.3 × 2.4 × 4.9 cm in size (RL × depth × height) and showed low signal on T1w, T2w, and STIR sequences indicative of necrosis. Mild surrounding edema was seen around the lesion. The patient is scheduled for excision of the mass from the right gluteal region after 2 months.
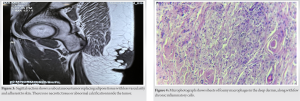
The most probable diagnosis for our patient is fat necrosis. What’s striking is that, subcutaneous fat necrosis appeared simultaneously at three sites with no apparent history of trauma, surgery, or pancreatitis. In 70% of cases, the cause of fat necrosis is unknown or unclear. Necrosis occurs when adipocytes become inflamed and die of hypoxia. Regions of fat necrosis feel like a round, firm lump, and there may also be dimpling, bruising, or changes in color of nearby skin [2]. The patient’s histopathology report showed skin and underlying tissue with mixed inflammatory cell infiltrate (Fig. 4) of histiocytes, lymphocytes, and plasma cells. Lipid laden foamy histiocytes and multinucleated foreign body type giant cells were seen. Loculated necrotic fat surrounded by dense fibrous tissue was also visible. Ultrasound of fat necrosis usually shows areas of peripheral hyperechogenicity and central areas of hypoechogenicity. There have been cases of mixed presentation of traumatic fat necrosis, such as hypoechogenicity and isoechogenicity. On MRI, it is commonly seen as hyperintensity in both T1-and T2-weighted images [4]. Our radiographic findings resonate in a similar manner. Surgical excision is the standard of care for any large lump or diagnosis of uncertainty. Smaller adiponecrotic areas can be managed conservatively through symptomatic palliation. For large traumatic fat necrosis, wide local excision with flap cover can be done, as was with our case [4]. One of the etiologies of subcutaneous fat necrosis, presenting as painless or painful nodules over legs, trunk, or buttocks, is pancreatitis or pancreatic carcinoma [5,6]. Pancreatic panniculitis is a rare clinical finding of pancreatic disease and is found in 2–3% of patients [7]. However, our patient does not have signs and symptoms pointing toward a pancreatic etiology. In addition, the amylase and lipase levels are within normal range. Hence, we can term the case to be of idiopathic origin after methodically eliminating all the other possible etiologies. The differential diagnoses that we considered were lipomatous tumors and inflammatory pseudotumors, which were eliminated through histopathology.
Although breast is a common site of adiponecrosis, it can also be found in the region of knee and buttocks without any clear etiology. Post-operative excisional biopsy can help in confirming diagnosis of the same. It is important to rule out malignancy and other tumors before reaching the diagnosis of fat necrosis.
There is little awareness regarding cutaneous panniculitis among clinicians, which may be due to its self-limiting nature. Presentation of fat necrosis as a large mass is atypical and may confuse the diagnostician [8]. Subcutaneous fat necrosis is a rare entity, which needs to be confirmed by a tissue biopsy to eliminate all the other possible subcutaneous lesions. It can mimic a lot of grave conditions including cancer and hence it is necessary to familiarize oneself with it [9,10].
References
- 1.Vasei N, Shishegar A, Ghalkhani F, Darvishi M. Fat necrosis in the Breast: A systematic review of clinical. Lipids Health Dis 2019;18:139. [Google Scholar | PubMed]
- 2.Fat Necrosis and Oil Cysts: Causes and Treatment; 2022. Available from: https://www.medicalnewstoday.com/articles/319517 [Last accessed on 22 Jul 2022]. [Google Scholar | PubMed]
- 3.Smith J, Arnoletti J, Varadarajulu S, Morgan D. Post-pancreatitis fat necrosis mimicking carcinomatosis. Radiol Case Rep 2008;3:192. [Google Scholar | PubMed]
- 4.Jayabal P, Arumugam S. A rare differential diagnosis of gluteal mass. J Orthop Dis Traumatol 2021;4:12. [Google Scholar | PubMed]
- 5.Hughes SH, Apisarnthanarax P, Mullins F. subcutaneous fat necrosis associated with pancreatic disease. Arch Dermatol 1975;111:506. [Google Scholar | PubMed]
- 6.Bruno CM, Pricoco GS, Bellinvia S, Amaradio MD, Cantone D, Polosa R. Necrotizing panniculitis as an uncommon manifestation of acute pancreatitis. Eur J Case Rep Internal Med 2017;4:000540. [Google Scholar | PubMed]
- 7.Laureano A, Mestre T, Ricardo L, Rodrigues AM, Cardoso J. Pancreatic panniculitis a cutaneous manifestation of acute pancreatitis. J Dermatol Case Rep 2014;8:35-7. [Google Scholar | PubMed]
- 8.Hanif Z, Ahmad M. Subcutaneous fat necrosis presenting as a large mass. Eur J Emerg Med 2006;13:106-7. [Google Scholar | PubMed]
- 9.Herzberger EH, Aviner S, Cherniavsky E. Posttraumatic fat necrosis presented as cellulitis of the leg. Case Rep Pediatr 2012;2012:672397. [Google Scholar | PubMed]
- 10.Shellagi N, Rodrigues G. Traumatic panniculitis of the right thigh: A case report. Oman Med J 2011;26:436-7. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Chronic Saphenous Nerve Entrapment Neuropathy after Closed Blunt Trauma: A Case Report
September 1, 2025 Chronic Saphenous Nerve Entrapment Neuropathy after Closed Blunt Trauma: A Case Report July 10, 2022 Morel-Lavallee Lesion Associated with Subtrochanteric Femur Fracture in a Young Female Resulting in Extensive Soft-Tissue Necrosis and Hypertrophic Non-union Managed with Staged Surgeries and Exchange Nailing: A Rare Injury Pattern and Review of Literature
July 10, 2022 Morel-Lavallee Lesion Associated with Subtrochanteric Femur Fracture in a Young Female Resulting in Extensive Soft-Tissue Necrosis and Hypertrophic Non-union Managed with Staged Surgeries and Exchange Nailing: A Rare Injury Pattern and Review of Literature July 10, 2018 A Case Report: Bilateral Patella Stress Fractures in a Collegiate Gymnast
July 10, 2018 A Case Report: Bilateral Patella Stress Fractures in a Collegiate Gymnast February 10, 2024 Percutaneous Tenotomy for Chronic Tennis Elbow: A Minimally Invasive Technique with Better Outcomes – A Case Series
February 10, 2024 Percutaneous Tenotomy for Chronic Tennis Elbow: A Minimally Invasive Technique with Better Outcomes – A Case Series