
The lessor trochanter of the femur can develop fatigue fractures with repetitive stress.
Dr. Yoshiaki Miyake, Department of Bone and Joint Surgery, Kawasaki Medical School, 577 Matsushima, Kurashiki 701-0192, Japan. E-mail: miyakeyoshiakimiyake@yahoo.co.jp
Abstract
Introduction: An avulsion fracture of the lesser trochanter of the femur in adults is rare and should be differentiated from neoplastic lesions. We present a rare case of avulsion fracture of the lesser trochanter of the femur with prodromal symptoms in an adult.
Case Report: A right-handed 40-year-old man with gradual-onset left hip joint pain resulting from baseball pitching consulted a neighborhood doctor. X-ray images did not show any obvious anomalies; however, the pain persisted. Two months after the onset of pain, he stumbled when getting into a car, and the pain worsened. He was then brought into our hospital’s emergency unit, and an avulsion fracture of the lesser trochanter of the left femur was detected. Due to mild displacement (<20 mm) and no neoplastic lesions by gadolinium-enhanced magnetic resonance imaging and the technetium scintigraphy, he was managed conservatively. During the final follow-up, 1 year after the onset of symptoms, non-union of the lesser trochanteric fracture was noticed. However, there were no pain and no limited range of motion at the hip joint; therefore, he had no problems with daily activities and sports.
Conclusion: The avulsion fracture of the lesser trochanter of the femur in our patient may have been caused by repeated flexion, adduction, and internal rotation of the hip joint during baseball pitching. Although bone union was not achieved, his condition was managed successfully using conservative treatment. Our experience offers a few key learning points to manage such rare fracture occurrences in adults and suggests that conservative treatment is often sufficient for mild displacement (<20 mm) of the fracture.
Keywords: Lesser trochanter of the femur, avulsion fracture, baseball.
Avulsion fracture around the pelvis and hip joint before epiphyseal line closure is a characteristic sports-related injury during bone growth. The most common sites of such fractures are the anterior superior iliac spine, anterior inferior iliac spine, and ischial tuberosity. The incidence of an avulsion fracture of the lesser trochanter of the femur is low (≤1% of avulsion fracture around the entire pelvis and hip joint) [1]. Furthermore, avulsion fracture after bone maturation is very rare. In this study, along with a literature review, we report a case of a middle-aged man who had prodromal symptoms following a stress avulsion fracture of the lesser trochanter of the femur that occurred while playing baseball.
The patient was a 40-year-old man (height, 178 cm; weight, 74 kg; and handedness, right-handed). He had no history of diseases that could cause bone fragility or any history of malignant tumors. He played baseball only a few times a year for recreational purposes. He had a gradual onset of pain in his left hip joint after throwing a ball as a baseball pitcher. When he consulted a neighborhood doctor, X-ray images (Fig. 1) did not show any obvious anomalies. However, the pain persisted even after a month. Therefore, he was referred to our department. The range of passive motion of the hip joint was as follows: right flexion, 120°; left flexion, 100°; right abduction, 30°; left abduction, 30°; right adduction, 15°; left adduction, 15°; right internal rotation, 10°; left internal rotation, 10°; right external rotation, 40°; and left external rotation, 40°. He experienced pain during deep flexion of the left hip joint. However, the results of Patrick test and FADIR test were both negative. In addition, X-ray images (Fig. 2) did not show obvious anomalies. 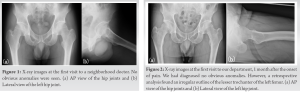 Three weeks after his first visit to our department, magnetic resonance imaging (MRI) of the lesser trochanter of the femur showed low-intensity signals on T1-weighted images and high-intensity signals on T2-weighted images (Fig. 3).
Three weeks after his first visit to our department, magnetic resonance imaging (MRI) of the lesser trochanter of the femur showed low-intensity signals on T1-weighted images and high-intensity signals on T2-weighted images (Fig. 3).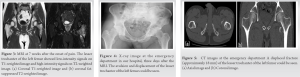 No obvious hip labral tear was observed. Therefore, he was diagnosed with a hemorrhage and edematous changes due to bone bruise of the lesser trochanter and was planned to be followed up. Three days after the MRI, he stumbled when trying to get into a car and his left hip joint pain worsened; he was brought to our hospital as an emergency case. He had difficulty walking due to severe pain. His left hip joint was slightly flexed and difficult to extend.
No obvious hip labral tear was observed. Therefore, he was diagnosed with a hemorrhage and edematous changes due to bone bruise of the lesser trochanter and was planned to be followed up. Three days after the MRI, he stumbled when trying to get into a car and his left hip joint pain worsened; he was brought to our hospital as an emergency case. He had difficulty walking due to severe pain. His left hip joint was slightly flexed and difficult to extend. 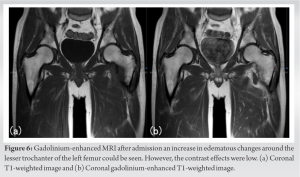 X-ray image (Fig. 4) and a computed tomography scan (Fig. 5) revealed an avulsion fracture of the lesser trochanter of the left femur. He was admitted to our hospital and placed on bed rest. He underwent gadolinium-enhanced MRI (Fig. 6) and technetium scintigraphy (Fig. 7) for detecting neoplastic lesions.
X-ray image (Fig. 4) and a computed tomography scan (Fig. 5) revealed an avulsion fracture of the lesser trochanter of the left femur. He was admitted to our hospital and placed on bed rest. He underwent gadolinium-enhanced MRI (Fig. 6) and technetium scintigraphy (Fig. 7) for detecting neoplastic lesions.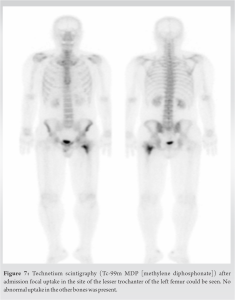 Gadolinium-enhanced MRI showed an increase in edematous changes; however, the contrast effects were mild. Technetium scintigraphy showed focal uptake in the site of the lesser trochanter of the femur; however, there was no abnormal uptake in other bones. Furthermore, blood biochemistry was unremarkable. Therefore, his condition was diagnosed as a stress avulsion fracture of the lesser trochanter of the femur. In addition, he received conservative treatment, because the displacement was relatively mild (18 mm). After 2 weeks of non-weight-bearing on the left lower extremity, partial (1/2) weight-bearing was permitted. At week 4 and beyond, full weight-bearing was permitted; no further fracture displacement occurred. The patient returned to active sports after 12 weeks. At his final follow-up, 1 year after the onset of pain (Fig. 8), we observed non-union of the lesser trochanteric fracture. However, he experienced no pain and had no signs of a limited range of motion in his left hip joint. In addition, he had no problem with his daily activities and sports.
Gadolinium-enhanced MRI showed an increase in edematous changes; however, the contrast effects were mild. Technetium scintigraphy showed focal uptake in the site of the lesser trochanter of the femur; however, there was no abnormal uptake in other bones. Furthermore, blood biochemistry was unremarkable. Therefore, his condition was diagnosed as a stress avulsion fracture of the lesser trochanter of the femur. In addition, he received conservative treatment, because the displacement was relatively mild (18 mm). After 2 weeks of non-weight-bearing on the left lower extremity, partial (1/2) weight-bearing was permitted. At week 4 and beyond, full weight-bearing was permitted; no further fracture displacement occurred. The patient returned to active sports after 12 weeks. At his final follow-up, 1 year after the onset of pain (Fig. 8), we observed non-union of the lesser trochanteric fracture. However, he experienced no pain and had no signs of a limited range of motion in his left hip joint. In addition, he had no problem with his daily activities and sports.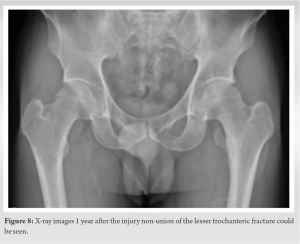
Avulsion fractures of the lesser trochanter of the femur occur most commonly among individuals aged approximately 13–18 years, that is, between the appearance of the secondary ossification center of the lesser trochanter and the closure of the epiphyseal line [1]. Before epiphyseal line closure, mechanical strength of the area is low. In addition, an imbalance between growth hormones and sex hormones [2] and repeated stress [3] may lead to the softening and weakening of the epiphyseal line. Moreover, the additional traction due to the iliopsoas muscle attached to the lesser trochanter of the femur could lead to avulsion fractures. Some studies have reported acute avulsion fractures that occurred while running in children between the ages of 13 and 18 years [4,5]. Contrastingly, there are few studies on avulsion fractures in healthy adults (such as the patient in this study). Because such fractures are very rare in adults, they need to be differentiated from neoplastic lesions [6]. Therefore, we performed a gadolinium-enhanced MRI and a technetium scintigraphy to detect any neoplastic lesions and none were found. Nevertheless, the patient had an avulsion fracture of the lesser trochanter of the left leg femur (the stepping leg of a right-handed pitcher). In baseball pitching, the range of motion of the non-dominant hip (the side of the stepping leg) correlates with the ball velocity [7]; therefore, the hip joint function of the stepping leg is important. It is possible that the muscles around the patient’s hip joint were less flexible, because he played baseball only a few times a year for recreation. In that condition, the hip joint of the stepping leg is flexed, adducted, and internally rotated during baseball pitching and is accompanied by the contraction of the hip extensors after the foot contacts the ground. This repetitive motion might have caused a stress fracture of the lesser trochanter, leading to prodromal symptoms, and the bone fragment might have displaced during hip flexion, 2 months after the onset. There are some studies on avulsion fractures of the lesser trochanter of the femur with prodromal symptoms in children [8,9]; however, to the best of our knowledge, no study has reported this condition in adults so far. Retrospective analysis of X-ray images taken during the patient’s first visit to our department showed an irregular outline of the lesser trochanter (Fig. 2). Instructions to rest at the prodromal stage might have prevented the displacement of the fracture. Regarding the treatment methods for avulsion fractures of the lesser trochanter of the femur, Anderson et al. highlighted the need to consider surgical treatments for displaced fractures of ≥20 mm [10]. Moreover, there are studies on the removal of the lesser trochanteric fracture fragments [11] and internal fixation under arthroscopy [12]. However, in most studies, conservative treatment achieves bone union without residual pain or limited range of motion [13]. The patient in this study received conservative treatment because the displacement of the fracture was <20 mm. However, bone union was not achieved, because he was an adult and his bones were already mature. Due to the dis appearance of pa in and no limitation of the range of motion, he currently has no problem with daily activities and sports. However, if pain persisted, the internal fixation or the removal of the lesser trochanteric fracture fragment was required for the non-union. In addition, high-performance adult athletes with an avulsion fracture of the lesser trochanter of the femur may require surgical treatments to prevent weakening of the iliopsoas muscle.
This case report presents a 40-year-old man with a stress avulsion fracture of the lesser trochanter of the femur after throwing a ball as a baseball pitcher. His condition was diagnosed and successfully managed through a conservative approach. This is the first report of a stress avulsion fracture of the lesser trochanter of the femur with prodromal symptoms in an adult and may serve as a reference in the management of such rare occurrences and, thus, may pave the way for further understanding of this condition.
An avulsion fracture of the lesser trochanter of the femur in adults is very rare. The fracture needs to be differentiated from neoplastic lesions. In the absence of neoplastic lesions and mild displacement (<20 mm) of the fracture, conservative treatment can facilitate good results.
References
- 1.Hamsa WR. Epiphyseal injuries about the hip joint. Clin Orthop 1957;10:119-24. [Google Scholar | PubMed]
- 2.Harris WR. The endocrine basis for slipping of the upper femoral epiphysis. An xperimental study. J Bone Joint Surg 1950;32-B:5-11. [Google Scholar | PubMed]
- 3.Alexander C. The etiology of epiphyseolysis. J Bone Joint Surg 1966;48-B:299. [Google Scholar | PubMed]
- 4.Memminger MK. Avulsion fracture of the trochanter minor in the adolescent. Acta Biomed 2018;90:175-6. [Google Scholar | PubMed]
- 5.Tahir T, Manzoor QW, Gul IA, Bhat SA, Kangoo KA. Isolated avulsion fractures of lesser trochanter in adolescents-a case series and brief literature review. J Orthop Case Rep 2019;9:11-4. [Google Scholar | PubMed]
- 6.Afra R, Boardman DL, Kabo JM, Eckardt JJ. Avulsion fracture of the lesser trochanter as a result of a primary malignant tumor of bone. J Bone Joint Surg Am 1999;81:1299-304. [Google Scholar | PubMed]
- 7.Robb AJ, Fleisig G, Wilk K, Macrina L, Bolt B, Pajaczkowski J. Passive ranges of motion of the hips and their relationship with pitching biomechanics and ball velocity in professional baseball pitchers. Am J Sports Med 2010;38:2487-93. [Google Scholar | PubMed]
- 8.Papacostas NC, Bowe CT, Strout TD. Lesser trochanter avulsion fracture. J Emerg Med 2013;45:256-7. [Google Scholar | PubMed]
- 9.Homma Y, Baba T, Ishii S, Matsumoto M, Kaneko K. Avulsion fracture of the lesser trochanter in a skeletally immature freestyle footballer. J Pediatr Orthop B 2015;24:304-7. [Google Scholar | PubMed]
- 10.Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med 2001;29:521-33. [Google Scholar | PubMed]
- 11.Quarrier NF, Wightman AB. A ballet dancer with chronic hip pain owing to a lesser trochanter bony avulsion: The challenge of a differential diagnosis. J Orthop Sports Phys Ther 1998;28:168-73. [Google Scholar | PubMed]
- 12.Khemka A, Raz G, Bosley B, Ludger G, Al Muderis M. Arthroscopically assisted fixation of the lesser trochanter fracture: A case series. J Hip Preserv Surg 2014;1:27-32. [Google Scholar | PubMed]
- 13.Dimon JH 3rd. Isolated fractures of the lesser trochanter of the femur. Clin Orthop Relat Res 1972;82:144-8. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Tibial Tubercle Avulsion Fractures in Adolescence in Sports Injury about Four Cases Series
February 10, 2024 Tibial Tubercle Avulsion Fractures in Adolescence in Sports Injury about Four Cases Series January 10, 2024 Bilateral Avulsion Fractures of Extensor Carpi Ulnaris: A Case Report
January 10, 2024 Bilateral Avulsion Fractures of Extensor Carpi Ulnaris: A Case Report December 10, 2023 Posterior Epidural Migrated Lumbar Disc Fragment at L2–3 Level Mimicking an Extradural Spinal Tumor: A Case Report
December 10, 2023 Posterior Epidural Migrated Lumbar Disc Fragment at L2–3 Level Mimicking an Extradural Spinal Tumor: A Case Report April 1, 2026 Subchondral Insufficiency Fracture of the Femoral Head in a Terminal Cancer Patient Treated by Total Hip Arthroplasty
April 1, 2026 Subchondral Insufficiency Fracture of the Femoral Head in a Terminal Cancer Patient Treated by Total Hip Arthroplasty