
Pediatric both bone forearm refracture with Titanium Elastic Intramedullary Nail system in situ is not a common complication and therefore the current modalities for management are surgeon or center specific. Therefore, we aim to share our experience with such a case and present a modality of management with an excellent outcome.
Dr. Ramzi Moucharafieh, Clemanceau Medical Center-Johns Hopkins Medicine International, Balamand University, Beirut, Lebanon. E-mail: ramzi.moucharafieh@gmail.com
Abstract
Introduction: Pediatric both bone forearm fracture is a common injury in children. A multitude of current treatments are available, with Titanium Elastic Intramedullary Nail system becoming very popular. The advantages of this treatment are many; however, refracture of these nails in situ is a reported uncommon complication, and there is a paucity in the literature on the appropriate management in these cases.
Case Report: An 8-year-old girl suffered from a left both bone forearm fracture after a fall from height, for which she was treated with the use of Titanium Elastic Intramedullary Nail system. Despite callus formation and fracture healing on X-rays, the nails were not removed at the intended time of 6 months due to the economic status of the country and the viral outbreak of COVID-19. Therefore, after 11 months of fixation, the patient presented again after a fall from height with the left both bone forearm refracture with the Titanium Elastic Intramedullary Nail system in situ. Intraoperative closed reduction was achieved with removal of the previous bent nails and refixation with new elastic nails. Follow-up of the patient 3 weeks later revealed satisfactory reduction with callus formation.
Conclusion: Pediatric both bone forearm refracture with Titanium Elastic Intramedullary Nail system in situ can be treated by gentle closed reduction and exchange nailing. This is not the first case to be managed with exchange nailing; however, it is one of the very few to have been treated as such and therefore these cases must be reported for further comparison with the different methods described in the literature to attain the optimal modality of treatment.
Keywords: Both bone forearm refracture, titanium elastic intramedullary nail system in situ, exchange nailing.
Both bone forearm fracture is a frequent injury in pediatric patients [1]. The prevalence of this type of fracture varies between 6% and 10% in the general population [2]. Most of these forearm fractures are treated nonoperatively with closed reduction and immobilization in a cast but with a 25% risk of secondary displacement on follow-up X-rays [3]. Surgical treatment is indicated when orthopedic treatment fails, either due to the inability to perform closed reduction or due to an unstable fracture pattern. Internal fixation with titanium elastic intramedullary nailing has become the golden standard of care [3]. To the best of our knowledge, cases of refracture after closed treatment with Titanium elastic intramedullary nail system (TENs) are rare, with no clear guidelines toward the optimal management [4].
A case of an 8-year-old girl brought to the emergency department with the left forearm pain and deformity following a fall from monkey bars of around 2 m in height. Neurovascular examination of the left hand was intact. X-ray (Fig. 1) showed a transverse fracture of the distal third of the radius and ulnar shaft with displacement and dorsal angulation of 40°. Open reduction using a three-centimeter incision at the fracture site to help in fracture reduction and removal of interposed soft tissues with placement of TENs (Fig. 2) through two small incisions at the distal radius and the proximal ulna was performed. Satisfactory fracture site reduction was achieved under fluoroscopy. Placement of posterior above-elbow splint was done and the patient was discharged home. 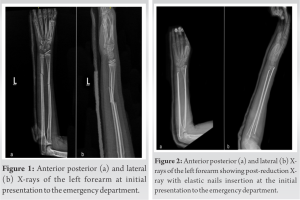 X-rays at 3-week postoperatively (Fig. 3) showed callus formation and the posterior splint was removed. She presented again after 11 months of treatment with a refracture with a bent intramedullary nail in situ (Fig. 4). The patient’s testing for disease causing bone fragility was negative. Clinical picture of the forearm before reduction was taken (Fig. 5).
X-rays at 3-week postoperatively (Fig. 3) showed callus formation and the posterior splint was removed. She presented again after 11 months of treatment with a refracture with a bent intramedullary nail in situ (Fig. 4). The patient’s testing for disease causing bone fragility was negative. Clinical picture of the forearm before reduction was taken (Fig. 5). 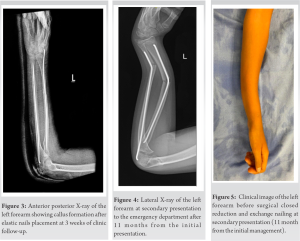 Using gentle closed manipulation of the fracture, straightening of the bent nail was successful (Fig. 6). Using the old incisions at the radial styloid and the ulna proximally, the old nails were removed (Fig. 7) and replaced with elastic nails of the same diameter. At 3-week follow-up, X-ray showed callus formation with satisfactory fracture alignment (Fig. 8). The posterior above-elbow splint was removed as per surgeon preference active and passive range of motion was initiated.
Using gentle closed manipulation of the fracture, straightening of the bent nail was successful (Fig. 6). Using the old incisions at the radial styloid and the ulna proximally, the old nails were removed (Fig. 7) and replaced with elastic nails of the same diameter. At 3-week follow-up, X-ray showed callus formation with satisfactory fracture alignment (Fig. 8). The posterior above-elbow splint was removed as per surgeon preference active and passive range of motion was initiated.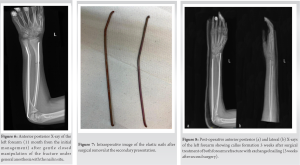
Pediatric forearm fractures are not uncommon and up until the mid-1990s, most of these fractures were treated conservatively with an upper arm cast [5]. Unstable or irreducible fractures, however, have surgical implications and can be treated through different modalities including an internal fixation with either plate and screws, Kirshnerwires, elastic intramedullary nails, or even hybrid fixation [6]. TENs is a widely used state-of-the-art modality that has been commonly used to treat these types of fractures, especially preferred for lesser morbidity for the pediatric patients, from smaller incisions to shorter anesthesia time and shorter hospital stay, as well as easier removal of material [6]. In their series of complications after treating 537 children with TENs, Fernandez et al. [5] encountered only 14 patients with a secondary fracture with the elastic nail in situ. Therefore, pediatric both bone forearm refracture before removal of the intramedullary nails is not a frequent condition, and only a few case series in the literature tackle this issue, with no well-defined guidelines set for the management of this complication. An interesting feature in our case is that the patient presented with refracture at 11 months post-primary fixation which to the best of our knowledge is one of the most distant time-elapsed for refracture since primary fixation to be reported. This might be because TENs are usually removed 6–12 months after primary fixation [7,8]. In our case, we opted to remove the material at 6 months but were unable to do so due to financial issues and the viral outbreak of COVID-19. In their case reports, Zhamilov et al. [9] and O’Neil et al. [10] reported each a case of refracture at 5-month post-primary fixation [9,10]. In their case series, Kelly et al. [11] reported six cases of refracture, four of which refractured after 6 months or less, and two of which refractured at 15 and 19 months [11]. However, the patient that refractured at 15 months had the smallest nail diameter in the case series, and the patient that refractured at 19 months was diagnosed with osteogenesis imperfecta. Since the rate of secondary fractures of pediatric both bone forearm with TENs in situ is relatively low, the only described management in the literature is that done by different institutions in case series, with no single and large study providing any long-term data on the results of the different management modalities. In our case, we opted for a closed reduction of the fracture and the damaged nail, which was uncomplicated and allowed the removal of the elastic nails without the need to open on the fracture site. Exchange nailing was done with nails from the same diameter. Larger diameter nails were considered in our management but could not be done since the nails that were already placed where the largest diameter possible for the patient’s intramedullary canal width. In their case report, O’Neil et al. opted for closed reduction with correction of the angulation of the bent nail aiming for an acceptable result without exchange nailing [10]. However, in the case report presented by Zhamilov et al., closed reduction alone did not yield acceptable alignment; therefore, the authors opted for exchange nailing with larger diameter nails [9]. The authors also argued that the mechanical stability of the TENs is significantly reduced if the nails were bent to more than 21°, as shown by a study done by Muensterer and Regauer [12]. Therefore, they concluded that exchange nailing is adequate for the management of refracture with TENs in situ. The authors of this case report agree and our experience is that exchange nailing yielded excellent results at 3-week post-operative.
TENs is a common surgical treatment for pediatric both bone forearm fracture. Refracture with the nails in place, however, is not usually seen, with a paucity of evidence regarding the appropriate management in the literature. We concluded that closed reduction with exchange nailing using a nail of the same diameter, or a larger diameter, if possible, is an appropriate modality of the management for such cases, with excellent results at 3-week post-operative.
Both bone forearm refractures with TENs in situ are a rare event. Management modalities differ in the literature and similar cases and their management need to be reported for optimal patient care. In our case, both bone forearm refractures in an 8-year-old girl with bent elastic nails in situ were successfully managed with closed manipulation and exchange nailing with excellent result at 3-week follow-up.
References
- 1.Naranje SM, Erali RA, Warner WC Jr., Sawyer JR, Kelly DM. Epidemiology of pediatric fractures presenting to emergency departments in the United States. J Pediatr Orthop 2016;36:e45-8. [Google Scholar | PubMed]
- 2.Bould M, Bannister GC. Refractures of the radius and ulna in children. Injury 1999;30:583-6. [Google Scholar | PubMed]
- 3.Pogorelić Z, Vodopić T, Jukić M, Furlan D. Elastic stable intramedullary nailing for treatment of pediatric femoral fractures; a 15-year single centre experience. Bull Emerg Trauma 2019;7:169-75. [Google Scholar | PubMed]
- 4.Van Egmond PW, van der Sluijs HA, van Royen BJ, Saouti R. Refractures of the paediatric forearm with the intramedullary nail in situ. BMJ Case Rep 2013;2013:bcr2013200840. [Google Scholar | PubMed]
- 5.Fernandez FF, Langendörfer M, Wirth T, Eberhardt O. Failures and complications in intramedullary nailing of children’s forearm fractures. J Child Orthop 2010;4:159-67. [Google Scholar | PubMed]
- 6.Caruso G, Caldari E, Sturla FD, Caldaria A, Re DL, Pagetti P, et al. Management of pediatric forearm fractures: what is the best therapeutic choice? A narrative review of the literature. Musculoskelet Surg 2021;105:225-34. [Google Scholar | PubMed]
- 7.Upasani VV, Li Y. Elastic intramedullary nailing of pediatric both-bone forearm fractures. JBJS Essent Surg Tech 2020;10:e19.00055. [Google Scholar | PubMed]
- 8.Sahu B, Mishra A, Tudu B. Management of pediatric both-bone forearm fractures by titanium elastic nailing system: A prospective study of 40 cases. J Orthop Traumatol Rehabil 2018;10:103-6. [Google Scholar | PubMed]
- 9.Zhamilov V, Reisoglu A, Basa CD, Kacmaz IE, Agus H. Pediatric forearm refracture with intramedullary nail bending in situ: Options for treatment. Cureus 2020;12:e6744. [Google Scholar | PubMed]
- 10.O’Neill CJ, Fitzgerald E, Kaar K, Murphy CG. Refracture of the pediatric forearm with intramedullary nails in situ. J Orthop Case Rep 2019;9:15-8. [Google Scholar | PubMed]
- 11.Kelly BA, Shore BJ, Bae DS, Hedequist DJ, Glotzbecker MP. Pediatric forearm fractures with in situ intramedullary implants. J Child Orthop 2016;10:321-7. [Google Scholar | PubMed]
- 12.Muensterer OJ, Regauer MP. Closed reduction of forearm refractures with flexible intramedullary nails in situ. J Bone Joint Surg Am 2003;85:2152-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Percutaneous Straightening and Exchange Nailing of a Bent Intramedullary Nail Following Tibial Shaft Fracture: A Case Report
March 1, 2026 Percutaneous Straightening and Exchange Nailing of a Bent Intramedullary Nail Following Tibial Shaft Fracture: A Case Report July 10, 2022 Morel-Lavallee Lesion Associated with Subtrochanteric Femur Fracture in a Young Female Resulting in Extensive Soft-Tissue Necrosis and Hypertrophic Non-union Managed with Staged Surgeries and Exchange Nailing: A Rare Injury Pattern and Review of Literature
July 10, 2022 Morel-Lavallee Lesion Associated with Subtrochanteric Femur Fracture in a Young Female Resulting in Extensive Soft-Tissue Necrosis and Hypertrophic Non-union Managed with Staged Surgeries and Exchange Nailing: A Rare Injury Pattern and Review of Literature January 10, 2018 Robot-Assisted Medial Compartment Arthroplasty Following Remote Patellectomy: A Case Report
January 10, 2018 Robot-Assisted Medial Compartment Arthroplasty Following Remote Patellectomy: A Case Report July 11, 2014 An Unusual Variant of Pipkin’s Fracture Dislocation of Hip: A Case Report
July 11, 2014 An Unusual Variant of Pipkin’s Fracture Dislocation of Hip: A Case Report