
Rheumatoid arthritis can be a cause of a neuropathic osteoarthropathy of the foot and ankle (Charcot foot).
Dr. Josephine Berger-Groch, Clinic of Trauma and Orthopaedic Surgery, Kriegsbergstr, 60, 70714 Stuttgart, Germany. E-mail: j.berger@uke.de
Abstract
Introduction: Neuropathic osteoarthropathy of the foot and ankle (Charcot foot) is a disease that can lead to progressive malpositioning and deformation up to complete collapse of the foot. In most cases, diabetic polyneuropathy is the underlying disease, but polyneuropathy of any cause can lead to neuropathic osteoarthropathy. Pathogenesis is still not completely understood. Due to the non-specific clinical presentation, the symptoms of Charcot arthropathy are generally easily misdiagnosed and proper therapy is delayed, especially in patients with an underlying disease other than diabetes mellitus. To date, published literature on patients with rheumatoid arthritis who develop neuropathic osteoarthropathy of the foot is scarce.
Case Report: We present a rare case of a 61-year-old patient with Charcot foot and rheumatoid arthritis. The patient presented with an extreme foot deformity after a failed conservative treatment. The surgical procedures, complications, and outcome are described. The pitfalls in this special patient group are highlighted.
Conclusion: If necessary, a variety of surgical options are available to maintain ambulation and prevent infection from open ulcers and amputation. For surgical management of patients with rheumatoid arthritis, the overall statics of the lower extremity and the influence of antirheumatic drugs must be considered.
Keywords: Rheumatoid arthritis, neuropathic osteoarthropathy, foot deformities, arthrodesis, Charcot foot.
Neuropathic osteoarthropathy of the foot and ankle (Charcot foot) is a disease involving bones, joints and soft tissue of the foot that can lead to a progressive malpositioning and deformation up to complete collapse of the foot [1]. The most common developing deformity is the so-called rocker-bottom deformity – a collapse of the arch in the metatarsus (Sanders and Frykberg II, Table 1). The malalignment of the foot can cause pressure damage to the skin, open wounds, and secondary bone infection. The presence of a rocker-bottom foot increases the risk of a major lower extremity amputation by 15–40 times [2]. The cause of neuropathic osteoarthropathy is a polyneuropathy. Numerically, most patients suffer from diabetic polyneuropathy, but polyneuropathy of any cause can lead to neuropathic osteoarthropathy [3]. Pathogenesis is still not completely understood, mainly, two different mechanisms are discussed: One is a neurovascular cause with increased blood flow and bone resorption, and the other a neurotraumatic cause with increasing deformities due to mishealed fractures. It is assumed that the reduced pain sensation leads to an inflammatory cascade with incorrect loading after a fracture and with the corresponding consequential damage. Overall, due to increased blood flow and proinflammatory processes, patients have increased osteoclast activity with high-turnover osteopenia [4]. Because the occurrence of neuropathic osteoarthropathy in connection with rheumatism is rare, there are only a few reports in the literature all without surgical focus. The present work intends to explain how to deal with this specific group of patients and to point out the pitfalls in the treatment of affected patients.
We present the case of a 61-year-old Caucasian male patient treated between 2018 and 2022 in our clinic. In 2015, the patient was diagnosed with chronic polyarthritis, and in 2017, he additionally received the diagnosis Charcot foot (Sanders and Frykberg type 3, Eichholtz type 1b Table 2, Fig. 1a and b). Consistent with this, MRI shows a bone bruise, soft-tissue edema, and joint effusion in stage 0. These increase markedly in stage 1, decrease again in stage 2, and leave residual edema and the resulting deformity in stage 3 (Chantelau E, Poll LW. [2006]. Evaluation of the diabetic Charcot foot by MR imaging or plain radiography – an observational study Exp Clin Endocrinol Diabetes. 2006. 114(8),428–431.  https://doi.org/10.1055/s-2006-924229). The foot had been immobilized, but, in 2018, he could no longer cope with it. Clinically, the patient presented with polyneuropathy at the plantar side of the foot, the foot was swollen, slightly hyperthermic and showed instability of the midfoot. As X-ray and MRI could not clearly distinguish between septic arthritis, rheumatoid arthritis, and Charcot foot a surgical bone sampling talonavicular and calcaneocubioidal was performed in this case. Here, neuropathic osteoarthropathy was confirmed. The patient developed a post-operative local wound infection ending in talus osteitis with the need for 16 follow-up surgeries until the soft tissue was closed again. Seven months later, the foot showed an osseous collapse in the hindfoot and metatarsus (Sanders and Frykberg type 2-4, Eichholtz type 3, Fig. 1c). A two-stage procedure was carried out. Due to the tense soft-tissue situation, an arthrodesis by external fixator of the upper and lower ankle joint and the midfoot was performed. The fixator was removed 4 months later. Since instability remained in the hindfoot, the patient received a nail arthrodesis (Expert HAN, Depuy Synthes, Massachusetts, USA) (Fig. 1d and e) under the idea of preserving the mobility in the Chopart joint line. Eight months later, the patient was again able to fully bear weight on the foot without a walking aid. In the clinical and radiological follow-up 2.5 years later (Fig. 1f), the patient is pain-free and mobile with full weight-bearing in a custom orthopedic boot. In patients with the need for a stable midfoot or hindfoot arthrodesis, a conscious effort is made to maintain mobility in the Chopart joint line.
https://doi.org/10.1055/s-2006-924229). The foot had been immobilized, but, in 2018, he could no longer cope with it. Clinically, the patient presented with polyneuropathy at the plantar side of the foot, the foot was swollen, slightly hyperthermic and showed instability of the midfoot. As X-ray and MRI could not clearly distinguish between septic arthritis, rheumatoid arthritis, and Charcot foot a surgical bone sampling talonavicular and calcaneocubioidal was performed in this case. Here, neuropathic osteoarthropathy was confirmed. The patient developed a post-operative local wound infection ending in talus osteitis with the need for 16 follow-up surgeries until the soft tissue was closed again. Seven months later, the foot showed an osseous collapse in the hindfoot and metatarsus (Sanders and Frykberg type 2-4, Eichholtz type 3, Fig. 1c). A two-stage procedure was carried out. Due to the tense soft-tissue situation, an arthrodesis by external fixator of the upper and lower ankle joint and the midfoot was performed. The fixator was removed 4 months later. Since instability remained in the hindfoot, the patient received a nail arthrodesis (Expert HAN, Depuy Synthes, Massachusetts, USA) (Fig. 1d and e) under the idea of preserving the mobility in the Chopart joint line. Eight months later, the patient was again able to fully bear weight on the foot without a walking aid. In the clinical and radiological follow-up 2.5 years later (Fig. 1f), the patient is pain-free and mobile with full weight-bearing in a custom orthopedic boot. In patients with the need for a stable midfoot or hindfoot arthrodesis, a conscious effort is made to maintain mobility in the Chopart joint line.
Our unusual case shows surgical possibilities, but also the risks in patients with neuropathic Charcot osteoarthropathy of the foot related to rheumatoid arthritis. As a destructive joint disease, untreated it often results in extreme deformity. In the active stage, conservative therapy with unloading and immobilization is recommended. Once conservative therapy methods are no longer promising, surgical therapy steps are indicated. The goal of such interventions is to prevent ulceration and to achieve a stable and plantigrade foot so that it is suitable for ambulation. In addition to the limited literature on patients with Charcot foot and rheumatoid arthritis, this case report highlights the difficulties of this particular disease combination [5,6]. Surgery To choose the right timing of surgery, it should be noted that stage II according to ichenholtz should be finished in order not to trigger the bony remodeling process. Since the foot is still undergoing remodeling during stage II, early surgery can cause the development or progression of bone necrosis, which subsequently leads to instability, screw loosening , or screw fracture and the risk of provoking pseudoarthrosis is also higher than in stage III [7,8]. The range of extremity-preserving surgical options is very broad including exostectomy (resection of plantar bony prominence located under a chronic ulcer), tenotomy/tendon lengthening, isolated or multiple fusions with external and/or internal fixation. Often, different methods are combined to prevent collapse due to the softer bone. The one method of choice does not exist, and each method must be adapted to the natural conditions of the disease [9]. In addition, the soft-tissue situation (ulcers) must be given special attention during surgical planning. In total, all treatment options have a high potential for complications and require frequent follow-ups for a long time. An exact post-operative regimen is hard to find in the literature, as the duration of unloading and immobilization varies greatly with the stage and method of surgical care. Normally, the time of unloading or partial weight-bearing increases in the case of presence of a charcot arthropathy. Finally, after successful rehabilitation, a custom orthopedic shoe must be fitted. Special characteristics of the rheumatoid patient versus diabetics Compared to diabetic patients, there are more joints affected in the foot in rheumatoid patients. In addition, chronic polyarthritis alters the whole skeleton, which significantly affects statics of the entire leg (Fig. 2). This must be included in the pre-operative planning. Postoperatively, it must be taken into account that many rheumatics suffer from arthrosis in the hands and mobilization on conventional crutches is difficult. The micro- and macroangiopathy often seen in diabetics, with consequent circulator y disturbances and increased susceptibility to infection, as well as partial previous amputations in parts, are not commonly seen in patients with rheumatoid arthritis. Patients with rheumatoid arthritis are often treated with combination therapy of a disease-modifying anti-rheumatic drugs (DMARDs) and glucocorticoids. Both groups of drugs are known to have a wide range of side effects. From a surgical point of view, the risk of wound healing disorders with infection in the surgical area must be considered. Further specific risks of DMARDs as the risk of pseudarthrosis under leflunomide [10] and the Methotrexate osteopathy are repeatedly described [11].
Neuropathic Charcot osteoarthropathy is a rare but serious complication of peripheral neuropathy that can mimic many other diseases (cellulitis, gout, deep venous thrombosis, osteomyelitis, or a minor sprain). MRI is the tool of choice to detect this condition. A variety of surgical options are available to maintain ambulation and prevent infection from open ulcers and amputation. In patients with rheumatoid arthritis, the overall statics of the lower extremity and the influence of antirheumatic drugs must be considered.
Patients with rheumatoid arthritis can rarely develop a Charcot osteoarthropathy. The primary treatment is conservative. After failure, a range of surgical possibilities are available. Patients’ statics and regular medication needs to be paid attention during therapy decision.
References
- 1.Harris A, Violand M. Charcot neuropathic osteoarthropathy. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/pubmed/29261935. [Google Scholar | PubMed]
- 2.Marmolejo VS, Arnold JF, Ponticello M, Anderson CA. Charcot foot: Clinical clues, diagnostic strategies, and treatment principles. Am Fam Physician 2018;97:594-9. [Google Scholar | PubMed]
- 3.Rosskopf AB, Loupatatzis C, Pfirrmann CW, Böni T, Berli MC. The Charcot foot: A pictorial review. Insights Imaging 2019;10:77. [Google Scholar | PubMed]
- 4.Lobmann R. The Charcot foot. In: Komplikationen des Diabetes Mellitus: Praxisorientiertes Wissen zu Begleit-und Folgeerkrankungen. 2nd ed. Berlin: Walter de Gruyter GmbH & Co.; 2022. p. 183-97. [Google Scholar | PubMed]
- 5.Grear BJ, Rabinovich A, Brodsky JW. Charcot arthropathy of the foot and ankle associated with rheumatoid arthritis. Foot Ankle Int 2013;34:1541-7. [Google Scholar | PubMed]
- 6.Uslu S. Charcot arthropathy due to rheumatoid arthritis. Oxf Med Case Reports 2021;2021:omab088. [Google Scholar | PubMed]
- 7.McCann L, Zhu S, Pollard JD, Weintraub ML, Dickinson JD. Success and sur v ivorship following Charcot reconstruction: A review of 151 cases. J Foot Ankle Surg 2021;60:535-40. [Google Scholar | PubMed]
- 8.Mehlhorn AT, Illgner U, Lemperle S, Huber V, Hoerterer H, Gottschalk O, et al. Does inflammatory activity of Charcot foot affect successful corrective arthrodesis. Orthopadie (Heidelb) 2022;51:499-506. [Google Scholar | PubMed]
- 9.Ferreira RC, Gonçalez DH, Filho JM, Costa MT, Santin RA. Midfoot Charcot arthropathy in diabetic patients: Complication of an epidemic disease. Rev Bras Ortop 2015;47:616-25. [Google Scholar | PubMed]
- 10.Fiehn C, Bauhammer J. Drug-induced osteopathy in rheumatology. Z Rheumatol 2022;81:189-97. [Google Scholar | PubMed]
- 11.Rolvien T, Jandl NM, Stürznickel J, Beil FT, Kötter I, Oheim R, et al. Clinical and radiological characterization of patients with immobilizing and progressive stress fractures in methotrexate osteopathy. Calcif Tissue Int 2021;108:219-30. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series
August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series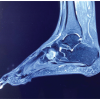 May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management April 1, 2026 Interest of a V-Y Quadricepsplasty in Bilateral Total Knee Arthroplasty for Ankylosed Flexion Knees in a Patient with Rheumatoid Arthritis – A Case Report
April 1, 2026 Interest of a V-Y Quadricepsplasty in Bilateral Total Knee Arthroplasty for Ankylosed Flexion Knees in a Patient with Rheumatoid Arthritis – A Case Report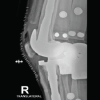 March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report
March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report