
Even though osteochondromas are very common, some of its rare types are misdiagnosed or missed due to their atypical varying presentations. Thus, it is vital for all orthopedicians to thoroughly examine the patients clinically and by imaging modalities to accurately diagnose and manage osteochondroma appropriately.
Dr. Basavaraj M K, Department of Orthopedics, B.L.D.E (DU) Shri B.M. Patil Medical College Hospital and Research Centre, Vijayapua - 586 103, Karnataka, India. E-mail: basavarajk201@gmail.com
Abstract
Introduction: Osteochondromas are very common. They are typically seen in long bones and rarely seen in smaller bones. Some of the rare presentations include flat bones, the body of pelvis, scapula, skull, and small bones of the hand and foot. Their presentation also varies according to the site of presentation.
Case Reports: We have included five cases of osteochondromas occurring at rare locations with variable presentations and their management. We have included one case of metacarpal, one case of skull exostosis, two cases of scapula exostosis, and one case of fibula exostosis.
Conclusion: Osteochondromas can rarely occur at unusual locations. It is important to thoroughly evaluate all patients presenting with swelling and pain over bony regions to accurately diagnose osteochondromas and manage accordingly.
Keywords: Scapula, metacarpal, fibula, skull, excision.
Osteochondromas are the most commonly occurring benign lesions of bone, making up around 12% among all the tumors of bone and 45% among all benign tumors of bone. Osteochondromas are bony protrusions on the outside of bones that are covered in cartilage [1]. It generally involves the metaphyseal region of the long bones, particularly seen surrounding knee joints and the proximal part of humerus [2]. However, the involvement of osteochondroma is significantly low and is <10% of the total cases for the small bones located in the hand. The involvement of pelvis and scapula is reported to be 5% and 4%, respectively [3]. Exostosis is caused by the hyaline cartilaginous cap, which basically functions as a growth plate, experiencing gradual endochondral ossification. The lower limbs are more commonly involved when compared to the upper limbs. The flat bones including the clavicle, the ribs, the scapula, the ilium, the pubic ramus, and the ischium undergo ossification typically during the fetal period by intramembranous ossification and are less likely to be affected [4,5]. Osteochondromas may present as a lone tumor also known as osteocartilaginous exostosis or as group of multiple tumors also known as multiple osteochondromatosis, Osteochondromas may sometimes turn into malignant lesions [6,7]. Most of these exostoses remain asymptomatic and undetected until they grow and achieve adequate size to cause compression of neurovascular bundles or vital organs in their vicinity [8,9]. Excision is usually curative for most of osteochondromas. Recurrence is common, if it is not excised completely. Plain X-rays, CT scans, and MRIs might be needed to diagnose an osteochondroma in addition to the clinical assessment and the necessary laboratory testing [10]. In this article, we report multiple occurrences of osteochondromas in various rare locations, their differing unusual properties, and how they were managed in our hospital. In this study, osteochondromas at various locations such as metacarpal, dorsal aspect of scapula, head of fibula, and skull have been reported.
Case 1-metacarpal
In the month of January in 2021, a 20-year-old male patient visited the hospital with complaints of pain and swelling of the right hand in the metacarpal region over the ulnar aspect on the palmer side for the past 5 years. It was gradually progressive in nature. The patient experienced dull aching pain; the pain aggravated upon the usage of the hand and was relieved by taking rest and medications. The swelling was not associated restriction of daily chores. On further evaluation, the swelling had the size of 4 cm × 3 cm ×2 cm (Fig. 1), the swelling was bony hard, it had an irregular surface and was fixed to the underlying bony structure and was immobile in the coronal or sagittal plane and had no other significant finding. The X-ray depicted a pedunculated bony mass with an outward growth from the distal part of the fifth metacarpal in its metaphyseal region as seen in Fig. 2. 
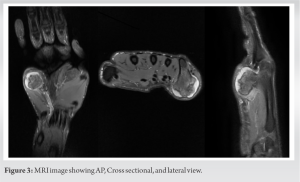 The magnetic resonance imaging, showed of 2 cm × 2.5 cm × 3 cm (Antero-posterior × Transverse × Superoinferior) measuring bony overgrowth seen coming from far end of the fifth metacarpal in its metaphyseal region causing displacement of flexor tendon (5th flexor digitorum profundus tendon) and causing impingment over flexor and abductor digiti minimi muscle belly (Fig. 3) and was diagnosed as osteochondroma. Osteochondroma excision done under general anesthesia, and a posteromedial skin inscision was made to approach the bony mass. Complete tumour excision done from the base of the pedicle (Fig. 4). The mass was removed and sent for histopathological testing and it was reported as osteochondroma showing bony trabecular tissue enclosed by a cartilaginous cap (Fig. 5).
The magnetic resonance imaging, showed of 2 cm × 2.5 cm × 3 cm (Antero-posterior × Transverse × Superoinferior) measuring bony overgrowth seen coming from far end of the fifth metacarpal in its metaphyseal region causing displacement of flexor tendon (5th flexor digitorum profundus tendon) and causing impingment over flexor and abductor digiti minimi muscle belly (Fig. 3) and was diagnosed as osteochondroma. Osteochondroma excision done under general anesthesia, and a posteromedial skin inscision was made to approach the bony mass. Complete tumour excision done from the base of the pedicle (Fig. 4). The mass was removed and sent for histopathological testing and it was reported as osteochondroma showing bony trabecular tissue enclosed by a cartilaginous cap (Fig. 5).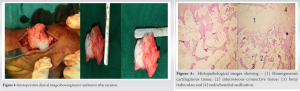 Post-operative radiograph of the hand was done on post-operative day one to confirm complete excision of tumor and suture removal done on post-operative day 12. Patient did not experience any pain and gained complete, pain-free movements at the wrist and metacarpophalangeal joint. The patient underwent clinical and radiographic examination with a satisfactory outcome (Fig. 6 and 7).
Post-operative radiograph of the hand was done on post-operative day one to confirm complete excision of tumor and suture removal done on post-operative day 12. Patient did not experience any pain and gained complete, pain-free movements at the wrist and metacarpophalangeal joint. The patient underwent clinical and radiographic examination with a satisfactory outcome (Fig. 6 and 7).
Case 2-scapula
In January 2022, a healthy 15-year-old kid came with a swelling over the right side of his back, which he had had for the past 3 years. Even though the swelling was first seen by his family members at age of 12, no immediate treatment was taken until now. The mass was the size of marble initially and slowly grew till the presentation. The patient presented with a normal movements of the right arm. He said that the main cause of his visit was cosmetic. On examination, a smooth, rounded, protruding, hard, and sessile lump palpated over the right scapular blade on its dorsal region over its lateral border with no other significant findings (Fig. 8). X-ray imaging showed a sessile outgrowth of the right scapula on the dorsal region near its medial border and was not involving the scapulothoracic joint (Fig. 9). The radiographic findings were consistent with that of a benign tumor and were diagnosed as solitary osteochondroma. The X-ray radiograph showed cortical and medullary bony outgrowth arising from the underlying bone, supporting the diagnosis of osteochondroma. MRI showed evidence of large well-defined sessile type exostosis arising from the posterior medial border of scapula. A lesion measuring 34x29x30mm in size with irregular overlying cartilage (Fig. 10). The patient was operated due to cosmetic purposes and to avoid further mechanical compression on surrounding structures on January 21, 2022 under general anesthesia. A linear open incision was taken over the lateral margin of the scapula centering over the protrusion where it is most protuberent. Muscular traction application done followed by extra periosteal enmassae resection of the mass was done (Fig. 11) and sample of lesion sent for histopathological examination. It showed homogenous cartilaginous material, bony trabeculae, and connective tissue (Fig. 12). Along with the post-operative scar, the patient on 1 and 2 monthly follow-up showed no recurrence of swelling and pain-free complete movements achieved at the right shoulder.
The radiographic findings were consistent with that of a benign tumor and were diagnosed as solitary osteochondroma. The X-ray radiograph showed cortical and medullary bony outgrowth arising from the underlying bone, supporting the diagnosis of osteochondroma. MRI showed evidence of large well-defined sessile type exostosis arising from the posterior medial border of scapula. A lesion measuring 34x29x30mm in size with irregular overlying cartilage (Fig. 10). The patient was operated due to cosmetic purposes and to avoid further mechanical compression on surrounding structures on January 21, 2022 under general anesthesia. A linear open incision was taken over the lateral margin of the scapula centering over the protrusion where it is most protuberent. Muscular traction application done followed by extra periosteal enmassae resection of the mass was done (Fig. 11) and sample of lesion sent for histopathological examination. It showed homogenous cartilaginous material, bony trabeculae, and connective tissue (Fig. 12). Along with the post-operative scar, the patient on 1 and 2 monthly follow-up showed no recurrence of swelling and pain-free complete movements achieved at the right shoulder.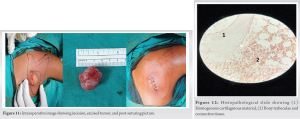
Case 3-skull
In July 2022, a 35-year-old male patient came with complaints of headache and a painless swelling over posterior aspect of skull (Fig. 13), which was insidious in onset and gradually progressed to present state. The patient noticed the swelling 2 months back. The patient had dull aching pain over the swelling and it had no associated symptoms and there was no restriction of day-to-day activities. CT showed a pedunculated growth in the occipital region arising from the inner table near the base of skull (Fig. 14).  The tumor clinically caused a swelling in occipital region of around 2 × 3 × 1 (L × B × D) cm. The patient was operated under general anesthesia in prone position. A vertical incision of around 4 cm was along the midline in occipital region centered over the swelling (Fig. 15). On exposure the growth was removed in chunks with the help of a bone burr and sample was sent for histopathological examination. It reported fragment of bone with cartilaginous elements further confirming the diagnosis of osteochondroma (Fig. 16).
The tumor clinically caused a swelling in occipital region of around 2 × 3 × 1 (L × B × D) cm. The patient was operated under general anesthesia in prone position. A vertical incision of around 4 cm was along the midline in occipital region centered over the swelling (Fig. 15). On exposure the growth was removed in chunks with the help of a bone burr and sample was sent for histopathological examination. It reported fragment of bone with cartilaginous elements further confirming the diagnosis of osteochondroma (Fig. 16).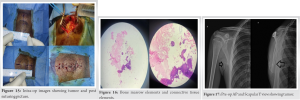
Case 4-scapula
In May 2022, a healthy 16-year-old male complained of painless swelling over his back on the right side for recent 2 years. Even though the patient’s family first saw it 2 years back, nothing was done till now. The mass gradually progressed over a period of time for next 3 years, then its growth came to a halt. At presentation, the patient had normal movements of the right arm and shoulder joint. On examining the patient, a smooth, globular, hard, and sessile swelling was noted in the lateral border of the dorsal region of the scapula on the right side. Even though there was no tenderness on palpatory examination, the movements of the right shoulder were complete with no other significant finding. X-ray imaging showed a sessile outgrowth on the dorsal region of the scapula on right side near its inferior angle and was not involving scapulothoracic joint (Fig. 17). The radiograph findings were suggestive of a benign bone tumor. The radiographic finding of a solitary osteochondroma was more likely. The patient underwent surgical excision to achieve better cosmesis and to avoid mechanical compression on surrounding structures on May 14, 2022 under general anesthesia with patient in the left lateral decubitus position. A linear open incision was made along the lateral border of the scapula. Extraperiosteal enmassae resection (Fig. 18) of the tumor was done, confirmed by post-operative imaging (Fig. 19) and sample of the lesion sent for histopathological examination (Fig. 20). The patient on 1- and 2-month follow-up, showed no recurrence of swelling and full pain-free movements of the right shoulder.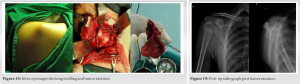
Case 5-fibula
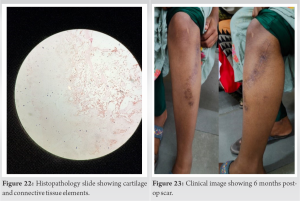
In November 2021, a 21-year-old female patient presented with pain and swelling over left knee and leg for 2 years. Patient initially noticed the swelling 2 years back which was insidious in onset and gradually progressed to current stage. The patient visited a local hospital multiple times with the compliant of pain and swelling over proximal part of the left leg, where patient was radiographed and was prescribed analgesics. The pain aggravated with walking and was relieved on rest and medications. Clinically patient had a palpable swelling over anterolateral aspect of left leg measuring around 3 × 3 cm. There was no involvement of common peroneal nerve. The patient was operated on November 16, 2021, for cosmetic reasons, under spinal anesthesia in supine position. An anterolateral incision of around 10 cm was made to expose the tumor. It was then resected and sent for histopathological examination. Fig. 21 shows the pre-operative, the immediate post-operative and the 6-month post-operative radiographs. The report mentioned bony trabecular elements lined by a cartilaginous cap suggestive of osteochondroma (Fig. 22). Fig. 23 shows post-operative scar.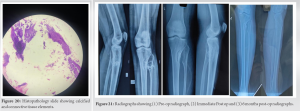
Osteochondromas are frequently asymptomatic and found by chance. A lump or mass that is not painful or tender is part of the clinical presentation. However, discomfort, palpable masses, and pathological fractures, which appear in roughly 17–94% of patients, are the most prevalent symptoms and signs [11]. While compressive neuropathy, bursa development with subsequent bursitis and limb deformity is also mentioned in the literature [8,9]. Osteochondromas involve epiphysis of long bones which have open physeal cartilage. They are believed to have started from the periosteum and are a developmental deformity rather than a real tumor. Diagnosis of osteochondroma can be made with simple radiographs like X-rays; however, flat bones require the use of more advanced techniques like MRI. A small osteochondroma in young patient groups in first and second decade of life needs to be carefully observed and followed cautiously because osteochondroma follows the course of bone growth pattern till the closure of the physeal cartilage. The involvement of the scapula is seen in 4% of all osteochondroma cases [3]. There have been reports of isolated head and neck sites, particularly those originating from the mandibular condyle and coronoid, as well as the intracranial and extracranial skull bases [12,13,14]. For extracranial osteochondromas, total surgical excision is thought to be the ultimate curative option [15]. Particularly, only 2.5% of all primary bone cancers are seen in the proximal fibula [16]. Immobilization by splintage, physiotherapy, NSAIDs, and local anesthetic injections is examples of conservative care strategies. When osteochondromas cannot be treated conservatively, the tumor must be removed surgically under anesthesia. The presence of osteochondroma at multiple sites and abrupt in cease in size after the third decade of life must be considered as warning signs of its malignant transformation, which demands appropriate management. Even though malignant transformation is uncommon in a single osteochondroma lesions. Other indications of malignancy include lobulations, septations, fibrous banding, myxoid altertions, and gadolinium enhancement. To direct ongoing care, clinicians must keep an eye on how an osteochondroma changes over time.
Osteochondromas can arise from rare locations with variable presentations. These are mostly non-symptomatic and most of the presenting symptoms can be attributed to mechanical block at the presenting site, which may vary across different locations making it difficult to diagnose osteochondromas presenting at rare locations. Therefore, it is important to thoroughly evaluate all patients presenting with pain and swelling over bony regions to accurately diagnose osteochondromas and manage accordingly and to monitor for signs of malignancy.
It is important to evaluate all patients presenting with pain and swelling over bony regions to accurately diagnose osteochondromas and manage accordingly.
References
- 1.Dahlin DC, editor. General Aspects and Data on 8542 Cases. 4th ed. United States: Charles C Thomas Pub Ltd.; 1986. [Google Scholar | PubMed]
- 2.Dahlin DC, editor. General Aspects and Data on 8542 Cases. 4th ed. United States: Charles C Thomas Pub Ltd.; 1986. [Google Scholar | PubMed]
- 3.Calafiore G, Calafiore G, Bertone C, Urgelli S, Rivera F, Maniscalco P. Osteochondroma: Report of a case with atypical localization and symptomatology. Acta Biomed Ateneo Parmense 2001;72:91-6. [Google Scholar | PubMed]
- 4.Gökkuş K, Atmaca H, Sağtaş E, Saylık M, Aydın AT. Osteochondromas originating from unusual locations complicating orthopedic discipline: Case series. Eklem Hastalik Cerrahisi 2015;26:100-9. [Google Scholar | PubMed]
- 5.Gökkuş K, Aydın AT, Sağtaş E. Solitary osteochondroma of ischial ramus causing sciatic nerve compression. Eklem Hastalik Cerrahisi 2013;24:49-52. [Google Scholar | PubMed]
- 6.Cho HS, Han I, Kim HS. Secondary chondrosarcoma from an osteochondroma of the proximal tibia involving the fibula. Clin Orthop Surg 2017;9:249-54. [Google Scholar | PubMed]
- 7.Unni KK. Cartilaginous lesions of bone. J Orthop Sci 2001;6:457-72. [Google Scholar | PubMed]
- 8.Wani IH, Sharma S, Malik FH, Singh M, Shiekh I, Salaria AQ. Distal tibial interosseous osteochondroma with impending fracture of fibula-a case report and review of literature. Cases J 2009;2:115. [Google Scholar | PubMed]
- 9.Romero AM, Artazcoz ED, Craven-Bartle Coll A, Calbo AG, Pinero MR. Thrombosed popliteal artery Pseudoaneurysm as herald of tibial osteochondroma. EJVES Short Rep 2016;33:27-31 [Google Scholar | PubMed]
- 10.Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In vivo 2008;22:633-46. [Google Scholar | PubMed]
- 11.Abdel MP, Papagelopoulos PJ, Morrey ME, Wenger DE, Rose PS, Sim FH. Surgical management of 121 benign proximal fibula tumors. Clin Orthop Relat Res 2010;468:3056-62. [Google Scholar | PubMed]
- 12.Chen PK, Chang SC, Huang F, Chen YR, Yeow VK, Williams WG. Transzygomatic coronoidectomy through an extended coronal incision for treatment of trismus due to an osteochondroma of the coronoid process of the mandible. Ann Plast Surg 1998;41:425-9. [Google Scholar | PubMed]
- 13.Vezeau PJ, Fridrich KL, Vincent SD. Osteochondroma of the mandibular condyle (literature review and report of two atypical cases). J Oral Maxillofac Surg 1995;53:954-63. [Google Scholar | PubMed]
- 14.Castillo M, Hudgins PA, Hoffman JC. Lockjaw secondary to skull base osteochondroma (CT findings). J Comput Assist Tomogr 1989;13:338-9. [Google Scholar | PubMed]
- 15.Dorfman HD, Czerniak B. Bone Tumors. St. Louis: Mosby; 1998. p. 331-52. [Google Scholar | PubMed]
- 16.Purandare NC, Rangarajan V, Agarwal M, Sharma AR, Shah S, Arora A, et al. Integrated PET/CT in evaluating sarcomatous transformation in osteochondromas. Clin Nucl Med 2009;34:350-4. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor April 1, 2026 Bilateral Sprengel’s Deformity Treated with Bilateral Modified Woodward Procedure: A Case Report
April 1, 2026 Bilateral Sprengel’s Deformity Treated with Bilateral Modified Woodward Procedure: A Case Report April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report
April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report March 1, 2026 Vascularized fibular flap for gunshot-induced composite foot defects: Two-case report and comprehensive literature review
March 1, 2026 Vascularized fibular flap for gunshot-induced composite foot defects: Two-case report and comprehensive literature review