
With the absence of characteristic chondroid calcifications, curettage with bone grafting provides a good outcome with no recurrence in the case of chondroblastoma.
Dr. Madhan Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr. MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: madhanjeyaraman@gmail.com
Abstract
Introduction: Chondroblastoma is a rare and benign bone neoplasm that accounts for <1% of all bone tumors. Chondroblastomas of the hand are extremely rare, while enchondromas are the most common bone tumor of the hand.
Case Report: A 14-year-old girl had complaints of pain and swelling over the base of her thumb for 1 year. On examination, a solitary and hard swelling was palpable over the base of the thumb, with terminal restriction of first metacarpophalangeal joint movements. Radiographs revealed an expansile and lytic lesion in the epiphyseal region of the first metacarpal. Chondroid calcifications were absent. Magnetic resonance imaging showed a lesion with the hypointense signal on T1 and T2 sequences. These suggested a diagnosis of enchondroma. Excisional biopsy of the lesion, bone grafting, and Kirschner wire fixation was performed. Histological examination showed the lesion to be a chondroblastoma. No recurrence was noted at the 1-year follow-up.
Conclusion: Chondroblastomas can very rarely occur in the bones of the hand. In such cases, differentiating them from enchondromas and ABCs is a challenge. Characteristic chondroid calcifications may be absent in nearly half of such cases. Curettage with bone grafting provides a good outcome with no recurrence.
Keywords: Chondroblastoma, enchondroma, calcifications
Chondroblastoma is a rare and benign bone neoplasm that accounts for <1% of all bone tumors [1]. It most commonly occurs in the tibia or femur [2]. Chondroblastomas of the hand are extremely rare, with only a few cases reported in the literature [3]. On the other hand, enchondromas are the most common bone tumor of the hand [4]. The two tumors pose certain distinguishing radiological appearances. However, we present a case of chondroblastoma of the first metacarpal masquerading as enchondroma in a child.
A 14-year-old female child had complaints of pain and swelling over the base of her right thumb for 1 year. The swelling was initially pea-sized and gradually increased in size over 1 year. Pain in the region start 2 months after noticing the swelling, which was dull aching, non-radiating, and aggravated with movements of the thumb. She has no similar swellings elsewhere in the body. She had no preceding history of trauma, fever, loss of weight, or appetite. She had no history of other medical conditions. She was right-hand dominant. On examination, a solitary and hard swelling of size 2.5 × 2.5 cm was palpable over the region of the head of the first metacarpal. The skin over the swelling showed no dilated veins and was pinchable. The swelling was found to be tender, having a smooth surface, borders were well defined, and the swelling was fixed to the bone. The range of movements of the first metacarpophalangeal (MCP) joint was found to be terminally restricted and painful (Fig. 1). Routine blood investigations were normal. Radiographs of the hand revealed a solitary, expansile, and lytic lesion in the head of the first metacarpal (Fig. 2).
Routine blood investigations were normal. Radiographs of the hand revealed a solitary, expansile, and lytic lesion in the head of the first metacarpal (Fig. 2). 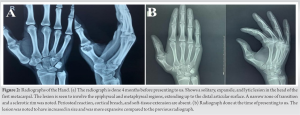 The lesion involved the epiphyseal and metaphyseal regions, extending up to the distal articular surface. A narrow zone of transition and a sclerotic rim were noted. Periosteal reaction, cortical breach, and soft-tissue extension were absent. On magnetic resonance imaging (MRI) of the hand, the lesion showed a hypointense signal on T1 and T2 sequences and was hyperintense on STIR sequences (Fig. 3).
The lesion involved the epiphyseal and metaphyseal regions, extending up to the distal articular surface. A narrow zone of transition and a sclerotic rim were noted. Periosteal reaction, cortical breach, and soft-tissue extension were absent. On magnetic resonance imaging (MRI) of the hand, the lesion showed a hypointense signal on T1 and T2 sequences and was hyperintense on STIR sequences (Fig. 3).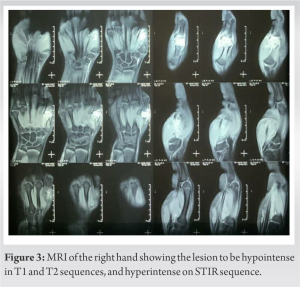 Endosteal scalloping was also noted. The radiological appearance led the radiologist to suggest a diagnosis of enchondroma of the first metacarpal. The location of the tumor in the hand and the benign radiological appearance led to the primary diagnosis to be considered as enchondroma of the first metacarpal head. This was also based on the fact that enchondromas are the most common chondrosarcomas of the hand. The closest differential to enchondroma we had to consider was low-grade chondrosarcoma. Low-grade chondrosarcomas share many of the same radiological features as enchondromas [5]. The presence of cortical breach was also favoring the possibility of low-grade chondrosarcoma. However, the absence of a cortical breach, permeative appearance, and soft-tissue involvement suggested enchondroma was more likely. An aneurysmal bone cyst (ABC) and chondroblastoma were two other less likely differential diagnoses that needed to be considered. However, the absence of septations and fluid-fluid levels on MRI made the diagnosis of ABC unlikely [6]. Chondroblastoma was considered unlikely due to the absence of calcifications and the fact that the location was very uncommon for chondroblastomas. Furthermore, chondroblastomas usually do not produce expansion of bone [1]. The child underwent an excisional biopsy of the lesion (Fig. 4).
Endosteal scalloping was also noted. The radiological appearance led the radiologist to suggest a diagnosis of enchondroma of the first metacarpal. The location of the tumor in the hand and the benign radiological appearance led to the primary diagnosis to be considered as enchondroma of the first metacarpal head. This was also based on the fact that enchondromas are the most common chondrosarcomas of the hand. The closest differential to enchondroma we had to consider was low-grade chondrosarcoma. Low-grade chondrosarcomas share many of the same radiological features as enchondromas [5]. The presence of cortical breach was also favoring the possibility of low-grade chondrosarcoma. However, the absence of a cortical breach, permeative appearance, and soft-tissue involvement suggested enchondroma was more likely. An aneurysmal bone cyst (ABC) and chondroblastoma were two other less likely differential diagnoses that needed to be considered. However, the absence of septations and fluid-fluid levels on MRI made the diagnosis of ABC unlikely [6]. Chondroblastoma was considered unlikely due to the absence of calcifications and the fact that the location was very uncommon for chondroblastomas. Furthermore, chondroblastomas usually do not produce expansion of bone [1]. The child underwent an excisional biopsy of the lesion (Fig. 4). The distal end of the first metacarpal was reconstructed with a bone graft obtained from the iliac crest and fixed with two Kirschner wires (Fig. 5).
The distal end of the first metacarpal was reconstructed with a bone graft obtained from the iliac crest and fixed with two Kirschner wires (Fig. 5).  The biopsy showed classical sheet-like proliferation of chondroblasts. The presence of a fine network of pericellular “chicken wire” calcifications was characteristic of chondroblastoma. Since chondroblastoma is also a benign lesion with recommended treatment being curettage and bone grafting, the excision biopsy was deemed adequate for its treatment. A radial slab was kept for 8 weeks. After 8 weeks, the Kirschner wires were removed and mobilization of the thumb started. The child was found to have no residual pain in the thumb. The child was followed up for 1 year and was not found to have a recurrence of the lesion. The movements of the first MCP joint, however, remained limited at 1-year follow-. The patient was offered for further surgical work-up to regain MCP movements. But the patient and her attenders denied the surgical procedure and the patient is still under follow-up.
The biopsy showed classical sheet-like proliferation of chondroblasts. The presence of a fine network of pericellular “chicken wire” calcifications was characteristic of chondroblastoma. Since chondroblastoma is also a benign lesion with recommended treatment being curettage and bone grafting, the excision biopsy was deemed adequate for its treatment. A radial slab was kept for 8 weeks. After 8 weeks, the Kirschner wires were removed and mobilization of the thumb started. The child was found to have no residual pain in the thumb. The child was followed up for 1 year and was not found to have a recurrence of the lesion. The movements of the first MCP joint, however, remained limited at 1-year follow-. The patient was offered for further surgical work-up to regain MCP movements. But the patient and her attenders denied the surgical procedure and the patient is still under follow-up.
Chondroblastoma is a cartilage-forming neoplasm occurring due to the abnormal proliferation of chondroblasts. They are considered to be benign; however, they may recur, and very rarely metastasize to the lung [7]. The exact etiology of the condition is still not known. It usually involves the epiphyseal regions of bones and occurs in skeletally immature individuals [8]. More than three-fourths of cases involve long bones, with the most common anatomical sites including the proximal and distal femur, proximal tibia, and proximal humerus [9]. Pain is the most common symptom, but patients can often have nonspecific complaints. Examination usually only reveals tenderness, effusion, and restriction of joint movements [10]. The typical radiological appearance is of a well-demarcated eccentric and lytic lesion with a thin rim of sclerotic bone. MRI shows edema of surrounding tissue and variable intensity on T2-weighted images [11]. The treatment of choice for chondroblastoma is surgical. The most commonly performed procedure for it is curettage and bone grafting, which is effective in almost all cases. Wide resection or amputation is very rarely required [7]. Chondroblastomas very rarely occur in the hand. Only single case reports of such occurrences are available in the literature [3]. Among the bones of the hand, the phalanx is more commonly involved [12]. When they occur in the hand, distinguishing them from other lesions, like ABC and enchondroma, is a challenge [13]. In our case as well, the absence of calcifications, presence of expansion of bone, and hypo intensity on T2-weighted MRI made the diagnosis more challenging. Calcifications have been reported to be absent in 46% cases of chondroblastomas involving small joints of the hand or feet [3]. In such cases, only a histological examination can confirm the diagnosis. Similar to chondroblastomas elsewhere in the body, curettage and bone grafting have been reported to produce excellent results for these lesions, with no recurrence [14]. Only eight cases of chondroblastoma of the phalanx have been reported to date [13]. Curettage and bone grafting have shown good results in all cases. While some authors have only used a slab for immobilization [15], some authors have stabilized using a plate and screws [13]. Ours is most likely, the only such case fixed with Kirschner wires.
Chondroblastomas can very rarely occur in the bones of the hand. In such cases, differentiating them from enchondromas and ABCs is a challenge. Characteristic chondroid calcifications may be absent in nearly half of such cases. Curettage with bone grafting provides a good outcome with no recurrence.
Differentiating enchondromas from ABCs poses a great clinical challenge. With the rare occurrence in hand and the absence of characteristic chondroid calcifications, curettage with bone grafting provides a good outcome with no recurrence in the case of chondroblastoma.
References
- 1.1. Limaiem F, Tafti D, Rawla P. Chondroblastoma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. Available From: https://www.ncbi.nlm.nih.gov/books/NBK536947 [Last accessed on 2022 Jan 17]. [Google Scholar | PubMed]
- 2.Garin IE, Wang EH. Chondroblastoma. J Orthop Surg (Hong Kong) 2008;16:84-7. [Google Scholar | PubMed]
- 3.Davila JA, Amrami KK, Sundaram M, Adkins MC, Unni KK. Chondroblastoma of the hands and feet. Skeletal Radiol 2004;33:582-7. [Google Scholar | PubMed]
- 4.Farzan M, Ahangar P, Mazoochy H, Ardakani MV. Osseous tumours of the hand: A review of 99 cases in 20 years. Arch Bone Jt Surg 2013;1:68-73. [Google Scholar | PubMed]
- 5.Afonso PD, Isaac A, Villagrán JM. Chondroid tumors as incidental findings and differential diagnosis between enchondromas and low-grade chondrosarcomas. Semin Musculoskelet Radiol 2019;23:3-18. [Google Scholar | PubMed]
- 6.Pai SN, Rajappa S, Pavithra V. Primary aneurysmal bone cyst of the phalanx. J Hand Microsurg 2021 (In Press). [Google Scholar | PubMed]
- 7.Masui F, Ushigome S, Kamitani K, Asanuma K, Fujii K. Chondroblastoma: A study of 11 cases. Eur J Surg Oncol 2002;28:869-74. [Google Scholar | PubMed]
- 8.Negri S, Wangsiricharoen S, Chang L, Gross J, Levin AS, Morris CD, et al. Clinicopathologic analysis of chondroblastoma in adults: A single-institution case series. Int J Surg Pathol 2021;29:120-8. [Google Scholar | PubMed]
- 9.Turcotte RE, Kurt AM, Sim FH, Unni KK, McLeod RA. Chondroblastoma. Hum Pathol 1993;24:944-9. [Google Scholar | PubMed]
- 10.Chen W, DiFrancesco LM. Chondroblastoma: An update. Arch Pathol Lab Med 2017;141:867-71. [Google Scholar | PubMed]
- 11.Oxtoby JW, Davies AM. MRI characteristics of chondroblastoma. Clin Radiol 1996;51:22-6. [Google Scholar | PubMed]
- 12.Peh WC, Shek TW, Ip WY. Metadiaphyseal chondroblastoma of the thumb. Skeletal Radiol 2000;29:176-80. [Google Scholar | PubMed]
- 13.Kudo T, Okada K, Hirano Y, Sageshima M. Chondroblastoma of a metacarpal bone mimicking an aneurysmal bone cyst: A case report and a review of the literature. Tohoku J Exp Med 2001;194:251-7. [Google Scholar | PubMed]
- 14.Gregory JR, Lehman TP, White JR, Fung KM. Chondroblastoma of the distal phalanx. Orthopedics 2014;37:e504-7. [Google Scholar | PubMed]
- 15.Bliss DG, Mann RJ. Chondroblastoma of a metacarpal. Report of a case and review of the literature. Clin Orthop Relat Res 1985;194:211-3. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report
August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report
July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report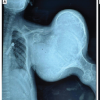 July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report
July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report