
Biological therapy with adult live cultured osteoblasts remains a viable treatment modality for AVN femoral head with a long-term follow-up.
Dr. Madhan Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr. MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: madhanjeyaraman@gmail.com
Abstract
Introduction: Avascular necrosis (AVN) of the femoral head is a type of osteonecrosis with the disruption of blood supply to the head of the femur. Management of AVN femoral head depends on the stage of the disease. In this case report, we elaborated on the biological therapy for bilateral AVN of the femoral head.
Case report: A 44-year-old male presented with pain in both hips for 2 years with a history of rest pain in both hips. Radiologically, the patient was diagnosed with bilateral AVN of the femoral head. The patient was offered bone marrow aspirate concentrate (BMAC) in the right femoral head, followed up for 7 years, whereas the adult autologous live cultured osteoblasts in the left femoral head, followed up for 6 years.
Conclusion: Biological therapy with differentiated osteoblasts remains a viable option for AVN femoral head when compared with an undifferentiated BMAC cocktail.
Keywords: Avascular necrosis, femoral head, cultured osteoblasts, bone marrow.
Avascular necrosis (AVN) of the femoral head is a common condition that leads to the progressive collapse of the head due to a lack of blood supply eventually leading to hip arthritis. This can lead to severe pain and loss of joint function and can ultimately lead to the need for hip joint replacement [1,2]. Treating AVN of the femoral head presents a complex challenge, and various surgical and non-surgical treatments have been developed over time. Studies have revealed a reduction in the number of mesenchymal stromal cells (MSCs) in the bone marrow (BM) and stroma of femoral heads, leading to the idea of injecting these deficient stem cells back into the femur head as a treatment option [3]. Among the regenerative modalities, the implantation of culture-expanded MSCs, autologous BM aspirate concentrate (BMAC), a stromal vascular fraction (SVF), and adult autologous live cultured osteoblasts (AALCO) have shown promising results. We present a case of bilateral AVN of the femoral head treated with the right hip autologous BMAC and left hip AALCO implantation with a follow-up for 6 years.
A 44-year-old male presented with pain in both hips for 2 years along with a history of rest pain in both hips. The patient had a BMI of 28.4 and complained of difficulty in walking and prolonged standing with restricted movements in both hips. No history of any trauma/covid/steroid/ alcohol use in the past was elicited. On examination, tenderness was demonstrable on both the hip joints over the Scarpa triangle with the telescopy test being negative. No evidence of swelling or deformity was noted over both hip joints. Trendelenberg test was positive with an antalgic gait. The terminal range of movements was restricted in both hips. A plain radiograph of the pelvis with bilateral hips showed evidence of AVN of bilateral femoral heads as depicted in Fig. 1.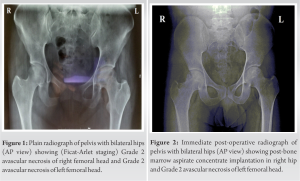 Magnetic resonance imaging (MRI) of both hips showed AVN of the bilateral femoral head with 10–30% involvement (Ficat-Arlet stage I) with the visualization of the hypointense line of demarcation. BM edema was demonstrated in the head, neck, and proximal shaft of the right femur with mild joint effusion in both hips. Based on the MRI and clinical findings, the patient was advised to undergo surgical intervention for both hips and the patient was informed about the potential for AVN progression on the opposite side.
Magnetic resonance imaging (MRI) of both hips showed AVN of the bilateral femoral head with 10–30% involvement (Ficat-Arlet stage I) with the visualization of the hypointense line of demarcation. BM edema was demonstrated in the head, neck, and proximal shaft of the right femur with mild joint effusion in both hips. Based on the MRI and clinical findings, the patient was advised to undergo surgical intervention for both hips and the patient was informed about the potential for AVN progression on the opposite side. 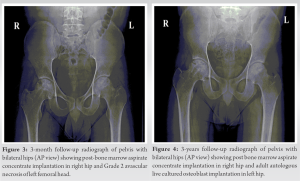 However, the patient was hesitant and only agreed to have surgery done on his right hip, which was more symptomatic at the time and was therefore treated first using decompression and BMAC injection as depicted in Figs. 2, 3, 4, 5. The patient noticed a gradual reduction in pain and also the ability to do his daily routine activities without any restriction. One year later, the patient similar complaints of pain, restricted movement, and difficulty in activities of daily living in the left hip for which he underwent decompression along with the injection of AALCO implantation as depicted in Figs. 4 and 5. BMAC implantation: 80 ml of BM was aspirated from the right anterior iliac crest and was processed with the help of Ficoll solution by differential centrifugation to obtain 16 mL of autologous BMAC injectate. A total of 48 million BMAC cells were obtained. AALCO implantation: 12 mL of BM was aspirated from the right anterior iliac crest and sent to Regrow Biosciences laboratory for the further ex-vivo culture of MSCs. Then MSCs are directed towards osteoblastic lineage till third passage. A total of 48 million AALCO were obtained. OSSGROW® (from Regrow Biosciences Pvt Ltd., Mumbai, India) is a commercially FDA-approved technology that involves implanting autologous adult live-cultured osteoblasts (AALCO), which are derived from mesenchymal stem cells sourced from the BM aspirate, for the treatment of osteonecrosis of the hip. The patient reported a gradual reduction of pain and symptoms on both sides following the procedure and there was a gradual improvement in the modified Harris hip score (mHHS) from 29 to 77 on the right side and from 31 to 83 on the left side. However, comparing VAS and functional scores of both hips at the same follow-up intervals, the left hip (AALCO) was found to have better function and pain scores when compared to the right hip (BMAC) which was found to be statistically significant (p<0.05). The serial radiographs of both hips show the impact of both surgeries on the necrotic process of the femur head.
However, the patient was hesitant and only agreed to have surgery done on his right hip, which was more symptomatic at the time and was therefore treated first using decompression and BMAC injection as depicted in Figs. 2, 3, 4, 5. The patient noticed a gradual reduction in pain and also the ability to do his daily routine activities without any restriction. One year later, the patient similar complaints of pain, restricted movement, and difficulty in activities of daily living in the left hip for which he underwent decompression along with the injection of AALCO implantation as depicted in Figs. 4 and 5. BMAC implantation: 80 ml of BM was aspirated from the right anterior iliac crest and was processed with the help of Ficoll solution by differential centrifugation to obtain 16 mL of autologous BMAC injectate. A total of 48 million BMAC cells were obtained. AALCO implantation: 12 mL of BM was aspirated from the right anterior iliac crest and sent to Regrow Biosciences laboratory for the further ex-vivo culture of MSCs. Then MSCs are directed towards osteoblastic lineage till third passage. A total of 48 million AALCO were obtained. OSSGROW® (from Regrow Biosciences Pvt Ltd., Mumbai, India) is a commercially FDA-approved technology that involves implanting autologous adult live-cultured osteoblasts (AALCO), which are derived from mesenchymal stem cells sourced from the BM aspirate, for the treatment of osteonecrosis of the hip. The patient reported a gradual reduction of pain and symptoms on both sides following the procedure and there was a gradual improvement in the modified Harris hip score (mHHS) from 29 to 77 on the right side and from 31 to 83 on the left side. However, comparing VAS and functional scores of both hips at the same follow-up intervals, the left hip (AALCO) was found to have better function and pain scores when compared to the right hip (BMAC) which was found to be statistically significant (p<0.05). The serial radiographs of both hips show the impact of both surgeries on the necrotic process of the femur head.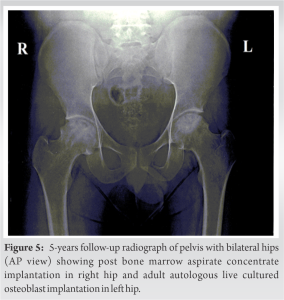 At 4-year follow-up, the right hip (BMAC) started showing signs of AVN progression with femoral head flattening and sclerotic margins whereas the left hip (AALCO) does not show any significant disease progression even at the final follow-up of 6 years.
At 4-year follow-up, the right hip (BMAC) started showing signs of AVN progression with femoral head flattening and sclerotic margins whereas the left hip (AALCO) does not show any significant disease progression even at the final follow-up of 6 years.
There is no published literature comparing the mid-term outcomes of BMAC versus AALCO in the same patient with a comparable grade of AVN on the femoral heads using one technique per side. The novelty of this case report lies in the fact that it evaluates the impact of two different interventions in the same patient with idiopathic AVN on serial follow-ups in terms of clinical, functional, and radiological outcomes. The traditional method of treating AVN through core decompression alone has become less popular as studies have indicated that up to 50% of patients experience progression to clinical failure. As a result, the use of adjuvants such as MSCs, BMAC, SVF, and AALCO has become more widespread. These treatments have been shown to eliminate the need for a total hip replacement (THR) in up to 70% of patients and have also shown evidence of reversing disease progression [4,5]. The use of stem cells in therapy was previously a concern due to issues of rejection, heterotopic ossification, and the potential for tumor induction, which were mainly related to the use of allogenic stem cells [6,7,8]. However, studies have shown that autologous stem cell therapy is a safer alternative, with minimal risk of side effects in the long-term [9,10]. Xu et al. concluded that core decompression along with transplantation of autologous marrow stem cells showed greater efficacy in the early stages of AVN and significantly reduced total hip arthroplasty conversion rate when compared to decompression alone [11]. Hauzeur et al. reported that the use of autologous osteoblasts delayed the progression of subchondral fracture and reduced VAS in patients with AVN of the head when compared to BMAC which was similarly evident in this case [12]. The conversion rates of patients to THA which was as high as 75% with the natural progression of the disease reduce up to 47% with BMAC, and now with the use of AALCOs, this has further dropped to around 20% as reported by Hauzeur et al. [12]. Jeyaraman et al. gave a level 2 recommendation on the usage of core decompression along with derived BM-MSCs are more efficacious in the management of osteonecrosis of the femoral head than core decompression alone. They reported that BM-MSCs offer better pain relief with an excellent functional outcome and delay the conversion of total hip arthroplasty [13]. Gangji et al. reported that osteoblast cell transplantation in AVN of the femoral head is more efficacious than concentrated BM implantation by delaying the evolution to subchondral fracture of the femoral head and reducing the pain in AVN of the femoral head [14]. Both BMAC and AALCOs are based on the principle that osteoprogenitor cells in the BM facilitate and induce new bone formation. However, the main limitation of BMAC is the fact they contain heterogeneous BM cells and it has been shown that bone alkaline phosphatase-characterized osteoblasts offer significantly higher bone regeneration potential which explains the efficacy of AALCO [15]. The use of AALCOs in the treatment of AVN is a relatively new regenerative modality for osteogenesis since it contains differentiated osteoblast cells. The advantages of AALCOs include the ability to control the number and quality of cells used in the treatment, which can lead to more consistent results. However, there are also disadvantages to both BMAC and ACOs. The major disadvantage of BMAC is the invasiveness of the procedure, as it requires the extraction of BM from the patient which may result in pain, bleeding, and a risk of infection. In addition, there is a risk of contamination of the BM during the processing and handling of the cells, which can reduce the effectiveness of the treatment. The disadvantages of AALCOs are production cost as it requires specialized equipment and expertise and a well-qualified surgical team. The efficacy of AALCOs in later stages of AVN (Stage 3 onward) is not proven [16,17]. This report has a few limitations which include the 1-year gap between the two interventions and no availability of MRI on serial follow. This is a single case follow-up and further larger sized randomized trials are needed to determine the efficacy in delaying THR and long-term outcomes of both procedures in the management of AVN.
Biological therapy in the form of AALCO implantation may be superior to BMAC implantation in the management of AVN of the femoral head due to the differentiated nature of osteoblasts in AALCO cells compared to undifferentiated MSCs in BMAC concentrate.
Proper surgical technique of harvesting, preparation, and implantation of differentiated osteoblasts into the necrosed part of the femoral head along with proper rehabilitation protocol may be a more effective solution than autologous undifferentiated BMAC in patients with early stages of idiopathic AVN thereby allowing them to get back to their daily routine activities with lesser down time and longer lasting results.
References
- 1.Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World J Orthop 2015;6:590-601. [Google Scholar | PubMed]
- 2.Vardhan H, Tripathy SK, Sen RK, Aggarwal S, Goyal T. Epidemiological profile of femoral head osteonecrosis in the North Indian population. Indian J Orthop 2018;52:140-6. [Google Scholar | PubMed]
- 3.Gangji V, Hauzeur JP, Matos C, De Maertelaer V, Toungouz M, Lambermont M. Treatment of osteonecrosis of the femoral head with implantation of autologous bone-marrow cells. A pilot study. J Bone Joint Surg Am 2004;86:1153-60. [Google Scholar | PubMed]
- 4.Kang JS, Suh YJ, Moon KH, Park JS, Roh TH, Park MH, et al. Clinical efficiency of bone marrow mesenchymal stem cell implantation for osteonecrosis of the femoral head: A matched pair control study with simple core decompression. Stem Cell Res Ther 2018;9:274. [Google Scholar | PubMed]
- 5.Palekar G, Bhalodiya HP, Archik S, Trivedi K. Retrospective study on implantation of autologous-cultured osteoblasts for the treatment of patients with avascular necrosis of the femoral head. Orthop Res Rev 2021;13:15-23. [Google Scholar | PubMed]
- 6.Berkowitz AL, Miller MB, Mir SA, Cagney D, Chavakula V, Guleria I, et al. Glioproliferative lesion of the spinal cord as a complication of “stem-cell tourism”. N Engl J Med 2016;375:196-8. [Google Scholar | PubMed]
- 7.Shimono K, Tung WE, Macolino C, Chi AH, Didizian JH, Mundy C, et al. Potent inhibition of heterotopic ossification by nuclear retinoic acid receptor-γ agonists. Nat Med 2011;17:454-60. [Google Scholar | PubMed]
- 8.Yin Z, Hu JJ, Yang L, Zheng ZF, An CR, Wu BB, et al. Single-cell analysis reveals a nestin(+) tendon stem/progenitor cell population with strong tenogenic potentiality. Sci Adv 2016;2:e1600874. [Google Scholar | PubMed]
- 9.Wakitani S, Okabe T, Horibe S, Mitsuoka T, Saito M, Koyama T, et al. Safety of autologous bone marrow-derived mesenchymal stem cell transplantation for cartilage repair in 41 patients with 45 joints followed for up to 11 years and 5 months. J Tissue Eng Regen Med 2011;5:146-50. [Google Scholar | PubMed]
- 10.Wong RS. Mesenchymal stem cells: Angels or demons? J Biomed Biotechnol 2011;2011:459510. [Google Scholar | PubMed]
- 11.Xu S, Zhang L, Jin H, Shan L, Zhou L, Xiao L, et al. Autologous stem cells combined core decompression for treatment of avascular necrosis of the femoral head: A systematic meta-analysis. Biomed Res Int 2017;2017:6136205. [Google Scholar | PubMed]
- 12.Hauzeur JP, Toungouz M, Lechanteur C, Beguin Y, Baudoux E, De Maertelaer V, et al. Autologous osteoblastic cells (PREOBy) versus concentrated bone marrow implantation in osteonecrosis of the femoral head: A randomized study. Rev Chir Orthop Traumatol 2016;102 Suppl 7:S73. [Google Scholar | PubMed]
- 13.Jeyaraman M, Muthu S, Jain R, Khanna M. Autologous bone marrow derived mesenchymal stem cell therapy for osteonecrosis of femoral head: A systematic overview of overlapping meta-analyses. J Clin Orthop Trauma 2021;13:134-42. [Google Scholar | PubMed]
- 14.Gangji V, Toungouz M, Lechanteur C, Beguin Y, Baudoux EP, De Maertelaer V, et al. THU0540 autologous osteoblastic cells versus concentrated bone marrow implantation in osteonecrosis of the femoral head: A Randomized controlled single blind study. Ann Rheum Dis 2016;75 Suppl 2:387. [Google Scholar | PubMed]
- 15.Prins HJ, Braat AK, Gawlitta D, Dhert WJ, Egan DA, Tijssen-Slump E, et al. In vitro induction of alkaline phosphatase levels predicts in vivo bone forming capacity of human bone marrow stromal cells. Stem Cell Res 2014;12:428-40. [Google Scholar | PubMed]
- 16.Hauzeur JP, De Maertelaer V, Baudoux E, Malaise M, Beguin Y, Gangji V. Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis: A randomized controlled double-blind trial. Int Orthop 2018;42:1429-35. [Google Scholar | PubMed]
- 17.Xu Y, Jiang Y, Xia C, Wang Y, Zhao Z, Li T. Stem cell therapy for osteonecrosis of femoral head: Opportunities and challenges. Regen Ther 2020;15:295-304. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes April 10, 2023 Short-term Follow-up of Autologous Adult Live-Cultured Osteoblasts Implantation in Avascular Necrosis of Femoral Head Secondary to Sickle Cell Anemia-Case Series
April 10, 2023 Short-term Follow-up of Autologous Adult Live-Cultured Osteoblasts Implantation in Avascular Necrosis of Femoral Head Secondary to Sickle Cell Anemia-Case Series June 10, 2022 Avascular Necrosis of the Hip Triggered by COVID-19 Infection in a Patient with Sickle Cell Disease: A Case Report
June 10, 2022 Avascular Necrosis of the Hip Triggered by COVID-19 Infection in a Patient with Sickle Cell Disease: A Case Report July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach