
Arthroscopic ACL reconstruction with single bundle Hamstring grafts are superior in strength, pre clude extensor mechanism disruption and result in early recovery.
Dr. Sudharsan Arumugam, Department of Orthopedic, Government Sivagangai Medical College, Sivagangai, Tamil Nadu, India. E-mail: sudharsanarumugam@gmail.com
Abstract
Introduction: Anterior cruciate ligament (ACL) injury is the common knee injury consequent to contact sports. There are different techniques recommended for the ACL reconstruction, with different graft materials. The aim of this study is to evaluate the functional outcome of arthroscopic single bundle ACL reconstruction using hamstring tendon graft in ACL deficient knees in adults.
Materials and Methods: Between 2014 and 2017, a prospective study was conducted in Thanjavur Medical College on 10 ACL deficient patients. All patients were evaluated preoperatively using the Lysholm and Gillquist score and IKDC – 2000 score. All patients underwent arthroscopic single bundle ACL reconstruction with hamstring tendon graft, which was fixed with an endo-button CL fixation system on the femoral side and an interference screw on tibial side. They were advised a regular rehabilitation protocol. All patients were evaluated post-operatively at 6 weeks, 3 months, 6 months, and a year by same assessment scores.
Results: Ten patients were available for follow up for a period of 6 months to 2 years. The mean follow-up period was 10.5 months. When compared with their respective pre-operative knee assessment scores, it was found that a definite improvement was there in their knee function. The results were good to excellent in 80% patients, fair in 10%, and poor in 10% cases.
Conclusion: For young active adults, single bundle reconstruction by arthroscopic methods gives acceptable results. The problems which are faced post-operatively can be again settled arthroscopically. A long-term follow-up of these cases is a must to analyze if there is degeneration that happened in the time between injury and ligament reconstruction.
Keywords: ACL reconstruction, hamstring graft, lysholm and gillquist score.
Anterior cruciate ligament (ACL) injury is one of the most common injuries around knee and also poses quite a lot of controversies in the management. ACL has a main role not only in the function but also as a stabilizer of the knee joint. Along with all other ligaments, capsule, and muscles, ACL is a prime stabilizer of the knee preventing the anterior translation of tibia over femur. Furthermore, ACL also restricts valgus and rotational stress to certain degree. When an individual sustains an ACL injury, they will have recurrent episodes of knee instability, knee pain, and decreased knee function. Few patients with less anticipated knee function can be managed non-operatively with intense physiotherapy, bracing, and modification of activity. However, with severe symptoms, young active patients may need reconstruction of the injured ligament. ACL injury is often associated with meniscal injury. If left alone, it can develop early onset of osteoarthritis. There is also a gradual decrease in ligament function and activity of individuals with ACL injured knee. The incidence of associated cartilage damage in acute ACL tears is 15–40% whereas it increases to 79% in chronic tears [1]. A stable knee prevents deterioration of existing chondral lesions as well as occurrence of newer lesions. Arthroscopic reconstruction of torn ACL has become the gold standard in treating ACL tears. The surgical reconstruction of the ACL with hamstring graft establishes knee kinematics. It does not sacrifice other stabilizers of knee. Development of early osteoarthritis, meniscal injuries are delayed and the stability of the joint is restored [2]. Earlier open arthrotomy, extra-articular procedures and intra-articular reconstructions were done. However, in current understanding of knee biomechanics and with current armamentarium of newer arthroscopic instruments and implants, arthroscopic ACL reconstruction is needed. Furthermore, usage of soft-tissue grafts is increasing in number than bone patellar tendon bone graft in recent times. Unlike open procedures, in arthroscopic reconstruction, there are small key hole incisions, decreased post-operative inflammation, almost near absence of post-surgical knee stiffness and possibility of early full range of movements postoperatively. However, there are also certain controversies regarding the ideal graft, ideal time, and technique of reconstruction [3]. Aim of our study is to evaluate the functional outcome of arthroscopic single bundle ACL reconstruction using quadrupled hamstring tendon (gracilis and semitendinosus autograft with endobutton as femoral fixation device and interference screw as tibial fixation device in ACL deficient knees in adults.
This is a prospective study that was conducted in Thanjavur Medical College, Thanjavur, for a period of 2 years. All young and middle-aged patients presenting with unilateral knee complaints and history of trauma to the knee in the orthopedics emergency and outpatient department in Thanjavur medical college, Thanjavur, were evaluated by a thorough general and local clinical examination of the knee. Specific tests were performed for diagnosing ACL deficiency like Lachmann test, Anterior drawer test, lateral pivot shift maneuver. Injuries to the associated structures were assessed by performing various clinical tests. Routine radiographs of both knees in standing position in anteroposterior view and lateral view of the affected knee were taken. MRI of the knee was done in all ACL torn cases for confirmation. Patients with clinical/MRI evidence of symptomatic individuals with ACL deficiency. Radiological evidence of skeletal maturity patient was between 20 and 40 years of age. A normal contralateral knee for comparison and rehabilitation and associated with medial or lateral meniscus tear that may or may not require repair were included in the study whereas asymptomatic individuals, patients with the systemic diseases compromising their pre-anesthetic fitness, associated with PCL tear, patients with osteoarthritic knee, and associated fracture of the tibial plateau, with local skin infections were excluded from study. Informed consent was obtained for all patients who are under this study. All consent was obtained before surgery. Institutional Ethics Committee permission was obtained before study. Post-operative immobilization in knee brace and limb elevation immediate postoperatively. Intravenous antibiotics were given postoperatively for 3 days. Drainage tube was removed on 2nd post-operative day. Wound was inspected on 2th, 5th, and 7th post-operative day. The Sutures were removed on 12th post-operative day. Gradual physical rehabilitation was started from day 1. Postoperatively, patients were followed up at 3, 6 weeks, and 3, 6 months. All patients were subjected to post-operative anteroposterior and lateral radiographs to determine the tunnel placement and position of endobutton in femur and interference screw in the tibia. Patients are followed at 3 weeks, 6 weeks, 3 months, 6 months, and once in 6 months thereafter for assessing functional outcomes. The International Knee Documentation 2000 Score and Lysholm and Gillquist Knee Scoring Scale [4] were used for evaluation of patients.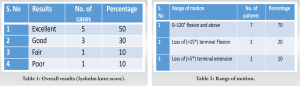
In our study, 10 cases of arthroscopic ACL reconstruction were regularly observed for a period of 4 months up to 2 years in Thanjavur medical college, Thanjavur. The mean follow-up period was 10.5 months. In our study, five patients were between 20 and 25 years, two patients were between 26 and 30 years, two patients were between 31 and 35 years, and one patients were between 36 and 40 years. Among ten patients, nine were male and one was female. The right knee was involved in seven patients and left knee in three patients. Most common mode of injury was sports injury (50%), whereas RTA was 25% and self-fall was 25%. In our study group, the duration of injury was up to 3 months in five patients, 6 months of injury in four patients, in one patient up to 9 months for 3 months, one patients for period of 1 year. The most common presenting complaint was knee pain and instability followed by locking of knee. In our study, five patients had some sort of treatment like aspiration or knee immobilization before surgery. Isolated ACL tear was associated in four patients, medial meniscal tear in three patients, lateral meniscal tear in one patients, and mild chondral changes in two patients. All ten patients in our study underwent arthroscopic single bundle ACL reconstruction using semitendinosus and gracilis as quadrupled graft. Patients are followed at 3 weeks, 6 weeks, 3 months, 6 months, and once in 6 months thereafter for assessing functional outcomes. In our study, eight patients had good to excellent results and the patients had no limp, were able to walk without support, there was no locking, except for a few with mild instability during athletics or heavy exertion [Table 1]. There was no pain or swelling of the knee joints. There was no difficulty in climbing stairs or squatting. In our case series, one of our patient in our study had fair results with the following clinical findings. There was slight limping, occasional locking, with mild instability during daily activities. There was anterior pain and swelling on exertion. Squatting and stair climbing were slightly impaired. Furthermore, in our study, one patient had poor results, with mild pain during weight bearing. The patient walked with support and felt the knee giving way in daily activities. There was constant swelling and pain of anterior knee joint. Squatting and climbing stairs were painful. Furthermore, range of motion was restricted in three patients in our study with two patients having loss terminal flexion and one patient having loss of terminal extension [Table 2].
Incidence of ACL reconstruction had increased significantly in the past decade due to the increased number of road traffic accidents and more involvement in sports activities. Arthroscopic ACL reconstruction has become gold standard [4] and open reconstruction has become almost obsolete nowadays. The arthroscopic procedure has the advantage of reduced morbidity, reduced incidence of patellofemoral adhesions, decreased anterior knee pain following reconstruction. Arthroscopic also has a technical advantage of better visualization of intra-articular structures and helps in accurate placement of tunnels. In some previous studies, Frank and Jackson [5] reported that arthroscopic reconstruction has better functional outcome in short-term but the outcomes were similar to open procedures in long-term. However, Barzegar et al. [6] reported arthroscopic reconstruction is superior to a mini arthrotomy procedures in time taken to return to pre-injury working level. There are only few studies comparing arthroscopic procedure with an open procedure as arthroscopy offers minimally invasive and more cosmetic surgery and have overshadowed open procedures. The arthroscopic reconstruction has been standardized. However, there are controversies regarding graft choice, graft fixation methods, and technique of reconstruction like single bundle or double bundle and transtibial or trans portal are still in debate. In the past decade, ACL has been widely studied and various scientific articles have been published on ACL reconstruction techniques and outcomes. The goal of reconstruction is to provide a normal stable joint with painless full function and to prevent the complications following ACL tear like meniscal injury and early onset of secondary osteoarthritis. Our study is to evaluate the functional outcome of arthroscopic single bundle ACL reconstruction with quadrupled Hamstring graft with transportal technique using endobutton as femoral fixation device and titanium interference screw as tibial fixation device. In our study sports injuries, fall and road traffic accidents predominated as the cause of injury accounting for 50%, 25%, and 25%, respectively. Sports injuries accounted for 50% similar to all international studies. In our study, 45% of patients had meniscal injury at presentation and medial meniscus injury predominated lateral meniscus injury like other studies. None of our patients had significant chondral damage at diagnostic arthroscopy. Lewis et al. [7] reported 58% of meniscal injury associated ACL tear at presentation. Medial meniscus was involved more than the lateral meniscus in his study and he also proposed meniscal repair or resection did not alter the outcome and chondral lesions are a better predictor of functional outcome. Lyman et al. [8] reported more than 50% of meniscal procedures with ACL reconstructions in 2009. The graft choice was of great debate in the recent years. The graft options include bone patellar tendon bone graft, Hamstring graft, Quadriceps tendon graft, allograft, and synthetic grafts. Bone patellar tendon bone graft has been gold standard until recent past as many studies supported patellar tendon graft for its strength and direct bone to bone healing providing early stability. However, recent development and advancement in soft-tissue fixation devices studies have found that hamstring grafts are superior in strength and avoiding extensor mechanism disruption. Harvey et al. [9] in 2005 published histological analysis of soft-tissue graft healing by indirect integration producing Sharpey fibers between the graft and bone and achieves adequate pullout strength by 12 weeks in animal studies. Although the outcomes equalized the donor site, morbidity was less with hamstring graft. Petterikousa based on in his biomechanical study comparing various fixation devices published that the Bone mulch screw is superior to any other device in providing stiffer fixation of soft tissue grafts and endobutton second only to bone mulch screw [10]. We did not use bone mulch screw in our study because of its cost and availability. Studies have proved that interference screws to be inferior to the endobutton and the bone mulch screw. One another concern was the laceration that interference screw can cause to the soft tissue graft. However, despite the concerns, interference screw fixation of soft-tissue grafts have shown comparable results with that of interference screw fixation of bone patellar tendon bone grafts. We used endobuttons as femoral fixation device and titanium interference screw as tibial fixation device. Although there are concerns about the bungee effect of the graft while using endobutton causing movement of graft in the tunnel, tunnel widening, and interference to graft incorporation, a recent study had reported that tunnel widening was more with interference screw than the endobutton and attributed tunnel widening to biological factors rather than mechanical factors of the fixation device. In our study, there was no pull outs or graft fixation site failures and in our patients endobutton was able to withstand the post-operative rehabilitation. We used transportal single bundle reconstruction with quadrupled hamstring graft placing the femoral tunnel between 10:30 and 11 o’clock position in the right knee and between 1’o clock and 1: 30 position in the left knee. This is very close to the position as proposed by John Paul’s placement of graft at 10 30 position and 1 30 position in single bundle reconstruction reconstructs portions of anteromedial and posterolateral bundles [11]. Our patients had 80% good to excellent results, 10% fair results, and 10% poor results were documented. Lewis et al. reported that 81% good results in his review article which showed 19% patients had positive pivot shift postoperatively. In our study, 10% patients presented with <5° extensor lag [12]. Overall patient satisfaction was good in 8 patients. Williams et al. [13] reported 2% infection which required arthroscopic joint lavage, similar 2% in our study which required arthroscopic joint lavage and joint debridement similar to his study. Austin et al. [14] showed fixing of graft in 30° flexion cause loss of extension and he recommended fixation of graft in extension. Lewis et al. reported that 50% of patients had arthritic changes in long-term follow-up. Since our study was a short-term follow-up, we could not comment about the arthritic changes postoperatively. Fox et al. [12] reported 3–17% incidence of anterior knee pain, compared to 10% in our study, Apostolopoulos reported 10% of anterior knee pain. Spindler et al. [15] stated that regular exercise can lead to better outcomes in ACL deficient individuals. Our patients are put on home based physiotherapy program insisting on knee flexion and quadriceps strengthening and mean flexion achieved was 135°. Grant and Mohtadi [16] concluded that home based physiotherapy is cost-effective and not significantly inferior to supervised programs. This several factors influence the functional outcome in arthroscopic ACL reconstruction. Factors such as graft choice, graft fixation, tunnel placement and graft tensioning play a key role in altering the final outcomes.
One of the most common ligament injuries of knee in younger age group is ACL injuries. The excellent treatment options for ACL deficient knee are arthroscopic reconstruction with hamstring autograft (semitendinosus/ gracilis). Postoperatively, results are excellent in pure ACL tear alone whereas fair to good results in individuals with ACL tear and associated menisci injuries. Quadrupled hamstring graft provides both anterior and rotatory stability to knee postoperatively almost similar results to pre-trauma level. ACL single bundle reconstruction with hamstring autograft is preferred over other techniques since it has advantages of less donor site morbidity, early recovery time, less damage to surrounding bony, and soft-tissue structures.
Functional outcome of ACL reconstruction is mainly determined by the position of tibial tunnel but tunnel widening is more with the use of interference screws over endobutton; moreover, single bundle Hamstrings grafts for ACL reconstruction are superior in strength and preclude extensor mechanism disruption with the favor of less donor site morbidity and early recovery reported in our study.
References
- 1.Fu FH, Bennett CH, Ma CB, Menetrey J, Lattermann C. Current trends in anterior cruciate ligament reconstruction: Operative procedures and clinical correlation. Am J Sports Med 2000;28:124-30. [Google Scholar | PubMed]
- 2.Bonnet A. Traite Des Maladies Articulaires. 2nd ed. Paris: Baillire; 1853. p. 354-7. [Google Scholar | PubMed]
- 3.Noulis G. Entorse du Genou. These N 142. Paris: Facultad de Medicina; 1875. p. 1-53 [Google Scholar | PubMed]
- 4.Aune AK, Holm I, Risberg MA. Four-strand hamstring tendon autograft compared with patellar tendon-bone autograft for anterior cruciate ligament reconstruction: A randomized study with two-year follow-up. Am J Sports Med 2017;29:722-8. [Google Scholar | PubMed]
- 5.Frank CB, Jackson DW. The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am 1997;79:1556-76. [Google Scholar | PubMed]
- 6.Barzegar H, Mohseni M, Sedighi A, Shahsavari A, Mohammadpour H. Arthroscopically-assisted vs. Open surgery in repairing anterior cruciate ligament avulsion. Pak J Biol Sci 2011;14:496-501. [Google Scholar | PubMed]
- 7.Lewis DW, Chan D, Fisher O, Lechford R, Mintowt-Czyz WJ. Incidence of meniscal and chondral injuries at the time of acl reconstruction, and their relationship with outcome at 2 years J Bone Joint Surg Br 2012;94:41 [Google Scholar | PubMed]
- 8.Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG. Epidemiology of anterior cruciate ligament reconstruction: Trends, readmissions, and subsequent knee surgery. J Bone Joint Surg Am 2009;91:2321-8. [Google Scholar | PubMed]
- 9.Harvey A, Thomas NP, Amis AA. Fixation of the graft in reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 2005;87:593-603. [Google Scholar | PubMed]
- 10.Kousa P, Järvinen TL, Vihavainen M, Kannus P, Järvinen M. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part I: Femoral site. Am J Sports Med 2003;31:174-81. [Google Scholar | PubMed]
- 11.Rue JP, Ghodadra N, Bach BR Jr. Femoral tunnel placement in singlebundle anterior cruciate ligament reconstruction: A cadaveric study relating transtibial lateralized femoral tunnel position to the anteromedial and posterolateral bundle femoral origins of the anterior cruciate ligament. Am J Sports Med 2008;36:73-9. [Google Scholar | PubMed]
- 12.Fox JA, Nedeff DD, Bach BR. Anterior cruciate ligament recon struction with patellar autograft tendon. CORR 2002;402:53-63. [Google Scholar | PubMed]
- 13.Williams RJ 3rd, Hyman J, Petrigliano F, Rozental T, Wickiewicz TL. Anterior cruciate ligament reconstruction with afour-strand hamstringtendon autograft. J Bone Joint Surg 2004;86:225-32. [Google Scholar | PubMed]
- 14.Austin JC, Phornphutkul C, Wojtys EM. Loss of knee extension after anterior cruciate ligament reconstruction: Effects of knee position and graft tensioning. J Bone Joint Surg Am 2007;89:1565-74. [Google Scholar | PubMed]
- 15.Spindler KP, Warren TA, Callison JC Jr., Secic M, Fleisch SB, Wright RW. Clinical outcome at a mini-mum of five years after reconstruction of the anterior cruciate ligament. J Bone Joint Surg 2005;87:1673-8. [Google Scholar | PubMed]
- 16.Grant JA, Mohtadi NG. Two to four year follow-up of a comparison of home vs. physiotherapy supervised rehabilitation programs following Acl reconstruction. J Bone Joint Surg Br 2008;90:108. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization
May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization November 1, 2024 Functional Outcomes in ACL Reconstruction: A Randomized Controlled Trial Comparing All-Inside and Transportal Techniques
November 1, 2024 Functional Outcomes in ACL Reconstruction: A Randomized Controlled Trial Comparing All-Inside and Transportal Techniques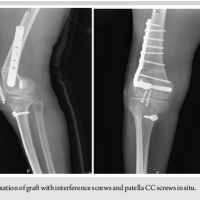 April 10, 2024 ACL Reconstruction using Achilles Allograft in a Case of Genu Recurvatum with Supracondylar Osteotomy
April 10, 2024 ACL Reconstruction using Achilles Allograft in a Case of Genu Recurvatum with Supracondylar Osteotomy June 10, 2023 ACL Reconstruction in a Poliotic Limb with Peroneus Longus Graft
June 10, 2023 ACL Reconstruction in a Poliotic Limb with Peroneus Longus Graft